
Abstract
Purpose:
Distal chevron osteotomy (DCO) is used more frequently than other methods for the correction of mild-to-moderate hallux valgus deformity because it is markedly more stable. Here, we evaluated the use of a capsuloperiosteal flap to stabilize DCO and presented our last longer follow-up.
Methods:
This study included a total of 57 patients (86 feet) made up of 50 women (79 feet) and 7 men (7 feet) with a mean age of 37.8 years who were diagnosed with hallux valgus and met the inclusion criteria. These patients received treatment using a capsuloperiosteal flap to stabilize DCO from 1994 to 2000. Clinical outcomes of the patients were assessed using the American Orthopaedic Foot and Ankle Society hallux scale.
Results:
The mean follow-up duration was 14.8 years. The score increased from a preoperative mean of 52 points to a mean of 90.5 points at last follow-up. The mean hallux valgus angle changed from 30.3° preoperatively to 14.4° postoperatively at the last follow-up. The first to second intermetatarsal angle changed from 13.6° preoperatively to 10.5° postoperatively. The correction in the range of motion proved to be consistent with only an average of 1° correction loss and 5.5° loss. Eighty-four feet (97.6%) were pain-free. Discomfort with shoe wear was absent in 82 feet (95.3%) postoperatively, and 23 of 24 (95.8%) patients were fascinated cosmetically.
Conclusion:
Correction of mild-to-moderate hallux valgus deformity with the use of capsuloperiosteal flap for stabilization of DCO provided findings comparable with the literature regarding clinical and radiological outcomes at long-term follow-up.
Introduction
Hallux valgus is one of the most seen deformities of the first ray. Numerous surgical techniques have been proposed since the term “hallux valgus” was introduced by Carl Hueter in 1871. 1 The purpose of surgical treatment is to eliminate the deformity without creating range of motion restriction and to remove pain. Chevron osteotomy has been preferred as an alternative surgical method to the modified McBride bunionectomy in patients with mild-to-moderate hallux valgus deformity. 2 The surgical procedure of chevron is usually accompanied by either internal fixation of the osteotomy or use of a short leg cast, postoperatively. 4 The senior surgeon has described the method of capsuloperiosteal flap for stabilization, without using internal fixation material or method and cast. Nonoperative treatments are the first choice to manage symptomatic hallux valgus deformity; when it fails surgeons have to correct the first intermetatarsal angle (IMA) less than 15° with a modified chevron osteotomy. The purpose of our study was to discuss clinical and radiographic results of a large number of patients with 15 years of follow-up.
Patients and methods
A total of 96 chevron osteotomies were performed in 65 patients with hallux valgus deformity who followed up in our clinic between 1994 and 2000. A total of 57 patients (86 feet), who were available for clinical and radiological analyses, have been followed up over a mean of 14.8 years (range 13.4–19.5). Six patients with different reasons were lost to follow-up. Two patients died. There were 50 women (79 feet, 82.3%) and 7 men (7 feet, 7.3%). The average age at the time of surgery was 37.8 years with the range of 19.2–51.5 years.
The patients’ major complaint was pain. The inclusion criteria of these patients were as follows: (1) failure of nonoperative treatment; (2) first to second IMA less than 15°; (3) hallux valgus angle less than 40°; (4) no degenerative findings of the first metatarsophalangeal (MTP) joint.
Patients were examined for the presence of callosities and toe deformities and range of motion of the first MTP joint, and the presence of pain with movement. Standing anteroposterior (AP) and lateral X-rays of affected feet were taken. The radiographs were repeated in follow-ups (postoperative first and seventh day, sixth month, first year). Radiographs were repeated every 5 years after 5 years of follow-up.
Pre- and postoperative assessments were conducted according to the American Orthopaedic Foot and Ankle Society hallux scale. 5,6 In AP radiography, the angle between the first and second intermetatarsals, hallux valgus, and relative lengths of the first and second metatarsals were measured. 7 The position of the tibial sesamoid and subluxation of the first MTP joint were defined.
Surgical technique
The surgical technique was represented in two papers previously. 3,4 All the patients were prepared in supine position under selective spinal anesthesia. Tourniquet (pneumatic) was applied for all patients. A Y-shaped capsulotomy was performed following dorsomedial longitudinal skin incision. The first MTP joint was seen when the capsuloperiostal flap was removed with sharp dissection. The bunion was excised. A V-shaped distal metatarsal osteotomy, the apex of which was at the center of the metatarsal head, with a 60° angle was performed. The distal fragment was lateralized after osteotomy approximately one-third the size of the metatarsal head, and the medial cortical prominence was cut. A double cortex tunnel drilled from dorsal to plantar was made solely proximal to the V-shaped osteotomy by a 2.5-mm drill. While holding the hallux in the wanted position, powerful absorbable stitches (No. 2 Vicryl) were crossed through this tunnel, attaching the top of the V-shaped capsuloperiosteal flap to the bone. The stability of the osteotomy was controlled manually by observing the passive range of motion. The residue of the capsule was sewed onto the capsuloperiosteal flap, intertwining the plantar flap more for sesamoid reduction, and internal fixation was not required. A lateral and AP radiograph or a fluoroscan of the operation area was acquired in the operating room. The subcutaneous tissues and skin were sutured with absorbable stitches. The first night, a bulky bandage and a night splint were implemented. The next day, the dressing was made. An elastic bandage and a night splint were recommended for 4–6 weeks. When they could tolerate walking on their heel with a hallux valgus shoe, the patients were countenanced to walk. A night splint was used for 6 weeks until a solid union occurred. For the cases that were bilateral, the second operation was applied at a mean of 9.8 (range 6–12) weeks following the first operation. Figure 1 illustrates the schematic graph of the surgery. Figure 2 demonstrates the images obtained during operation.
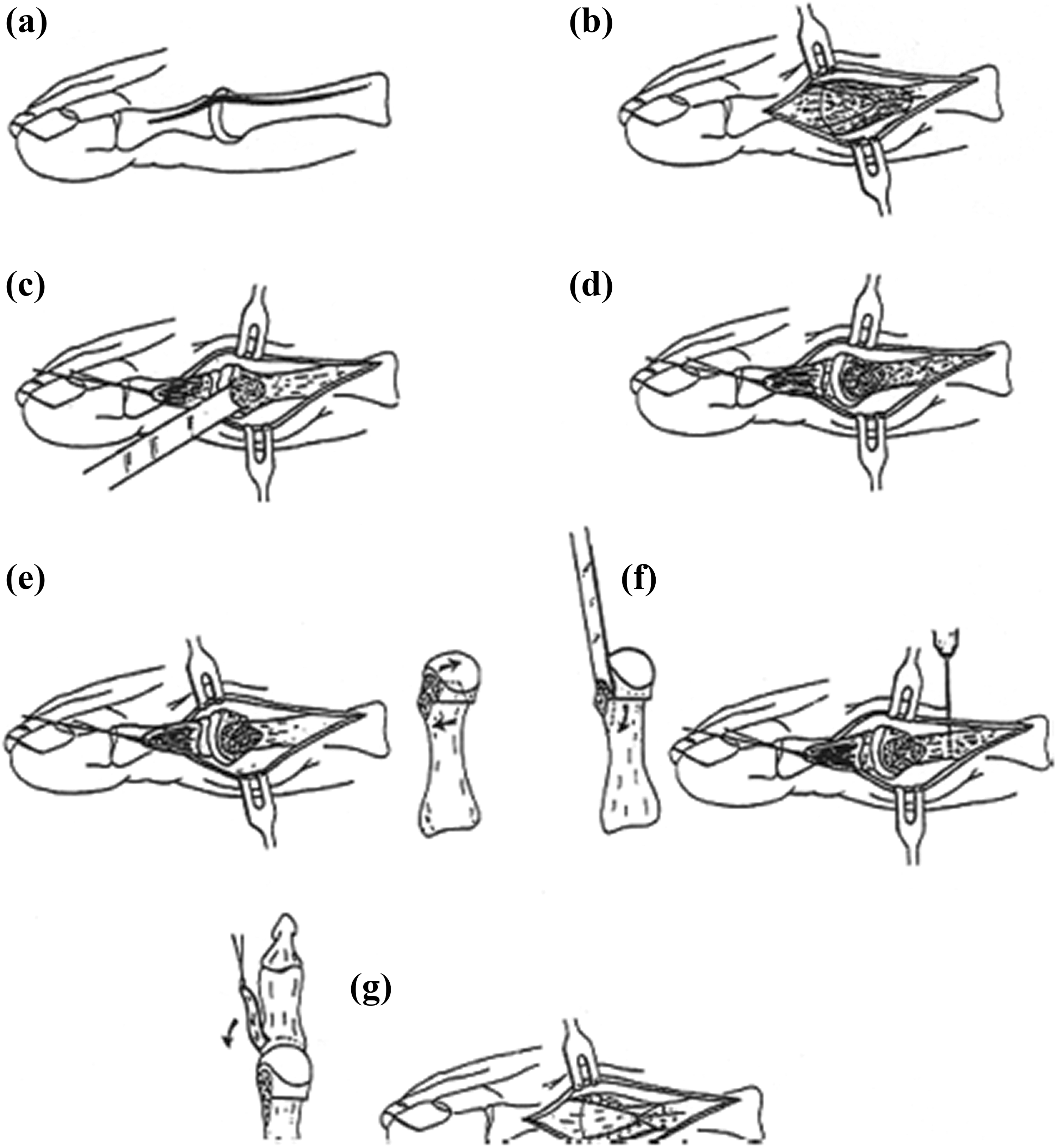
Illustration of the modified distal chevron procedure and capsuloperiosteal flap stabilization (image originally appeared in The Journal of Foot and Ankle Surgery, 28(1): 4, 1999; used with permission). 3
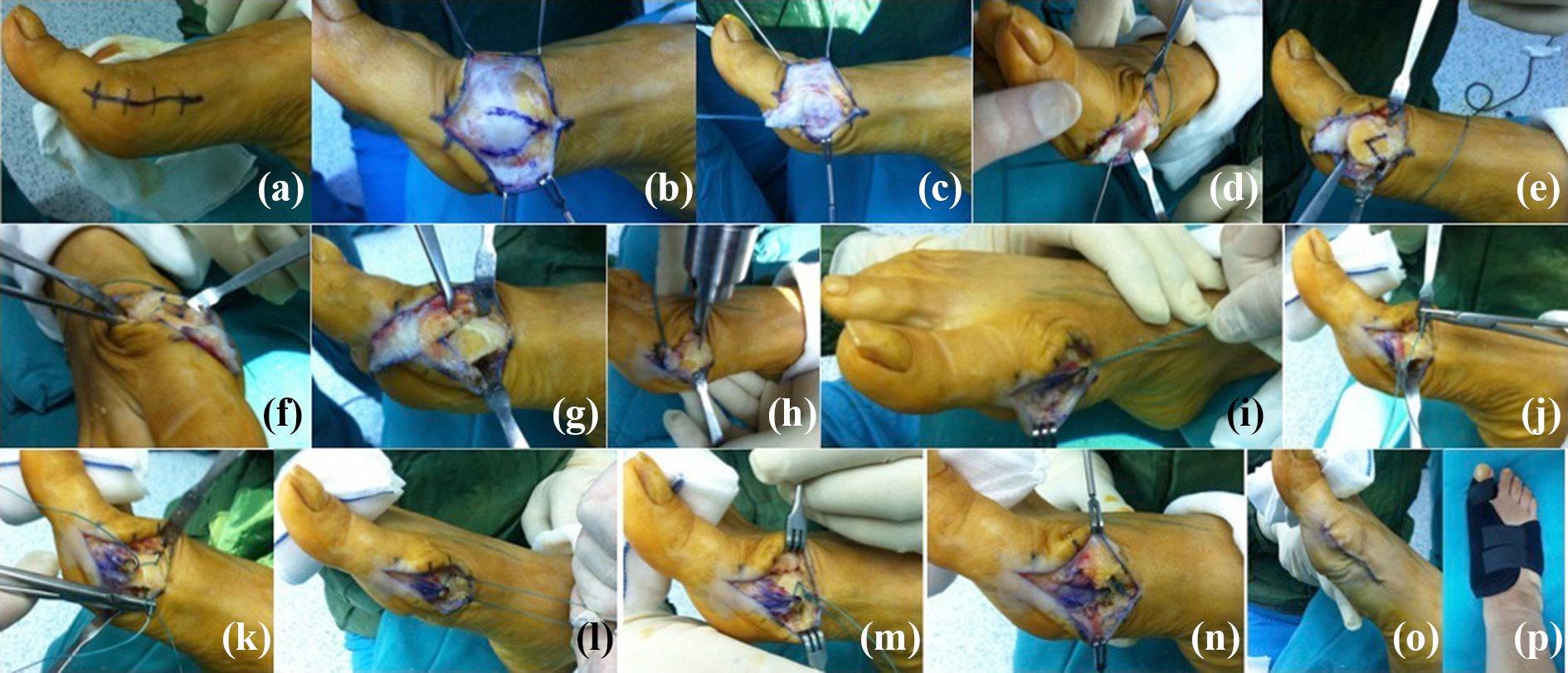
Intraoperative pictures: (a, b) Surgical incision and joint capsule; (c) capsuloperiosteal flap elevated and tagged by suture; (d) bunion removed; (e) chevron osteotomy performed; (f, g) distal fragment lateralized and prominence removed; (h) metatarsal shaft drilled; (i, j, k, l, m, n) sutures passed through canal for attaching capsuloperiosteal flap to the bone. The rest of the capsule sutured over this flap and imbricated; (o, p) operation completed.
Results
The mean range of combined dorsiflexion and plantar flexion motion of the first MTP joint was 74.7° with the range of 30–130° in preoperative examinations. At the last follow-up, the mean range of motion of the first MTP joint was 69.2° with the range of 24–123°. The mean motion lost between the preoperative period and the last follow-up was 5.5°. The mean correction of the IMA between the first and second metatarsals was 3.1° (preoperative and last follow-up mean values were 13.6° and 10.5°, respectively). The mean correction of the first MTP angle was 15.9° (preoperative and last follow-up mean values were 30.3° and 14.4°, respectively) (Table 1).
Clinical and radiographic data of 88 feet with follow-up after 5–11, 3–14.8 years.

AOFAS: American Orthopaedic Foot and Ankle Society; MTP: metatarsophalangeal; IMA: intermetatarsal angle; ns: nonsignificant.
aSignificance levels refer to differences between the two follow-up investigations: preoperative assessment, 5 and 11, 3 years after surgery. Bonferroni adjusted Wilcoxon sign rank test.
bNegative value indicates first metatarsal is shorter than the second.
A postoperative X-ray revealed that 46 (of total 49) laterally located sesamoids were settled into normal anatomic location. Forty-one of the 86 feet had subluxation of the first MTP joint preoperatively, and 39 (95%) regained normal anatomic congruency postoperatively. The mean hospitalization duration was 2 days with the range of 1–7 days. Radiographic changes of union of the osteotomies in all patients were seen at the sixth week of surgery. Forty-six (80.8%) patients returned to work before the sixth postoperative week, 11 (19.2%) patients required an extra 2 weeks of rest.
At the last follow-up, assessments were performed according to the American Orthopaedic Foot and Ankle Society hallux scale. There was no pain in 84 (97.6%) of the 86 feet. Only one patient who had bilaterally operated, also decreased complaints, although occasionally one of the feet would experience pain. Complaints about pain while wearing shoes were absent in 82 (95.3%), improved in 2, and still present in 2 feet. In general, our patients become able to wear conventional, wide shoes from the sixth week postoperatively and fashionable shoes without any insert or modification at a range of 11–15 weeks postoperatively (mean 12 weeks).
Twenty-three out of 24 patients who were unhappy with the appearance of their feet were pleased with their appearance after the surgery. Patients with metatarsalgia had improvements within the first 6 months after the surgery. Forty of the 42 (95.2%) callosities resolved, while 2 persisted. Four of the patients (6.15%) evolved severe early postoperative swelling.
We did not have any recurrences of the deformity and malunion, delayed union, nonunion, or comminution of the fragments. Dysesthesia and/or hypoesthesia occurred at the incision site of two feet. One of the cases had a stiff MTP joint with no complaints. On the radiographic images taken at last follow-up, increased density of the metatarsal head without any sign of osteoarthritis and avascular necrosis was detected in two patients. Only one patient developed cystic changes of the metatarsal head with no degenerative changes. In the first postoperative month, four (4.5%) cases of superficial infection were observed and completely resolved with antibiotic therapy.
Discussion
Many surgical techniques have been described for correction of hallux valgus deformity up to the present. The chevron technique is the most popular method; it is easy, reliable, and effective. It was first described by Corless 8 and popularized by Johnson et al. 9 This operation was named for the V-shaped cut that was made from the medial side of the head of the first metatarsal. The osteotomy line has been carried proximally for better stability, more bony contact, less joint stiffness, and for the ability to correct more severe deformities. The advantage of the chevron technique is the further correction of the IMA and hallux valgus angle while the disadvantage of the distal chevron osteotomy (DCO) is the potential for nonunion, malunion, and avascular necrosis of the first metatarsal head. 10 There are ongoing discussions about internal fixation of osteotomy. Kirschner wires or screws have been suggested; however, some authors advised using cast postoperatively to protect them from complications related to internal fixation such as pin tract infection, loss of stabilization, soft tissue irritation, migration of wires, pain around wires, and stress shielding effect on bone. 11,12 Although, casting has been shown to increase the MTP stiffness, in the stiffness rates of between 4.8% and 42% reported in the literature, it has been shown to decrease the rate of lost correction. 13,14 Only one case was observed with a range of motion loss greater than 30°. After union was completed without complications, for easier and more comfortable rehabilitation, the use of night splints only was suggested. In a series by Ozkurt et al., the mean duration of return to work was 6 weeks, which is similar to our study. 2
As one of the most common complications of surgically treated hallux valgus, loss of correction and recurrence of the deformity are reported at around 10% in the literature. 14,15 We have observed an average of 1° (7.4%) correction loss in the MTP angle between the postoperative period and the last follow-up period, and we did not observe any recurrence in follow-up examinations. Malunion, delayed union, nonunion, or comminution of the fragments were absent; however, these were prevented by better stabilization and compression by suturing the distal capsular flap to bone, which achieved stable fixation of the osteotomized fragments. We have an idea that compression provided by the capsular attachment to the metatarsal helped achieve solid union.
Adductor or lateral capsular release was not performed on any patients because the necessary correction was achieved with proximal advancement and fixation of the medial capsular flap. As Resch et al. have proposed, adductor release adds an insignificant increase of correction. 16 Also, carrying out more soft tissue release increases the risk of avascular necrosis, 17 although some recent studies have shown that lateral release does not impair the circulation of the metatarsal head. 18,19
Our long-term outcomes have shown that promotion of union by compression and better maintenance of correction could be achieved by advancing the capsular flap medially and attaching it to the medial metatarsal shaft. In this way, the osteotomy site can be internally fixated easily and safely, and above all, cast-associated complications are avoided, thus increasing comfort and patient adherence to the treatment protocols.
Conclusion
Correction of mild-to-moderate hallux valgus deformity with the use of capsuloperiosteal flap for stabilization of DCO provided findings comparable with the literature regarding clinical and radiological outcomes at long-term follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.