
Abstract
Purpose:
To compare the bone fusion of freeze-dried allograft alone versus freeze-dried allograft combined autograft in spinal instrumentation due to spondylodiscitis.
Methods:
A randomized prospective trial of patients with spondylodiscitis treated with surgical debridement and spinal fixation with freeze-dried bone allograft and autograft (Group 1) or freeze-dried bone allograft alone (Group 2) was performed. Patient follow-up was assessed with a CT-scan for bone fusion; consecutive serum inflammatory marker detection (C-reactive protein, [CRP], and erythrocyte sedimentation rate, [ESR]) and clinical assessment (pain, functional disability, and spinal cord injury recovery) were other outcome parameters. The primary outcome was the grade of bone allograft integration with the scale of Tan (which ranges from 1 to 4, with lower scores indicating a better fusion rate) at 1 year after surgery.
Results:
A total of 20 patients were evaluated, 13 (65%) men and 7 (35%) women with a mean age of 47.2 (±14.3) years. Homogeneous distribution of demographic data was observed. A similar satisfactory bone graft fusion grade was observed in both graft groups at 1 year after surgery (p = 1.0000). Serum inflammatory markers gradually decreased in both groups after surgical intervention (CRP, p < 0.001; ESR, p < 0.01). At one-year follow-up, gradual improvement of pain, functional disability, and neurological spinal injury recovery in both graft groups were achieved.
Conclusion:
Freeze-dried allograft alone could be a therapeutic option for spinal fixation surgery due to spondylodiscitis since it achieves a satisfactory graft fusion rate and clinical improvement.
Level of Evidence:
Level 1. Treatment
ClinicalTrials.gov register:
NCT03265561
Keywords
Introduction
Spondylodiscitis accounts for 95% of all spinal infections. 1,2 This destructive infectious process spreads to contiguous spaces and affects the disc space and the two adjacent vertebral bodies. 1,3 Spondylodiscitis treatment aims to eliminate the focus of infection, restore spinal functionality, and reduce pain. 4 Surgical debridement treatments are associated with vertebral instability due to extensive removal of all damaged tissue. To achieve vertebral stabilization, spinal instrumentation (anterior or posterior) has been indicated in cases of extensive bone destruction, severe kyphosis, or failure of conservative treatment. 1,5 Also, bone grafts (autografts and allografts) have been previously used to obtain adequate stability of the affected spinal segment. Autografts were first employed in spondylodiscitis surgeries because of their osteoinductive, osteogenic, and osteoconductive properties. However, they are a limited resource in size and quantity and are also associated with surgical complications such as pain, neurovascular injury, infection, cosmetic deformity, increased blood loss, and donor site structural weakness or fracture. 6 Therefore, other therapeutic options, such as allografts have been under study. 6,7 Compared with an autograft, a bone allograft can be obtained in unlimited quantities, can provide immediate structural support, no donor site morbidity occurs and surgical time might be importantly reduced. 6
There are different types of bone grafts. Fresh-frozen allografts are obtained from a post mortem donor and preserved at −80°C until use. Their advantages are that they are a stronger graft and they had more complete integration with the host bone; their disadvantages are that they might incite an immune response that is responsible for a delay in vascularization and osteoblast and osteoclast activity. Freeze-dried allografts are obtained in the same way but they are lyophilized, allowing them to be stored at room temperature. This allograft is less immunogenic than fresh-frozen allografts. 7
It has been reported that host age, gender, nutritional condition, associated diseases; type of fusion, length of fusion, and type of spinal instrumentation can affect bone graft integration. 8 In spinal instrumentation due to infections, whether the allograft should be used alone or in combination with the autograft has not yet been defined, since some authors 9 indicate that the autograft is superior to the freeze-dried allograft, and others 10 that there is no difference in the fusion or the clinical evaluations when comparing both grafts. Thus, this study aimed to compare the bone graft integration grade of freeze-dried allograft alone or combined with an autograft in spinal instrumentation due to spondylodiscitis in a randomized controlled trial.
Methods
Trial design
We conducted a prospective, randomized, controlled clinical trial in patients with spondylodiscitis who were randomly assigned in a 1:1 ratio to undergo either spinal fixation with freeze-dried allograft and autograft (Group 1) or freeze-dried allograft alone (Group 2). Institutional Ethics in Research Committee approval was obtained and the study was registered at ClinicalTrials.gov (register no. NCT03265561).
We enrolled patients over 18 years of age who had received a diagnosis of spondylodiscitis by imaging studies (radiography, computed tomography [CT], and/or magnetic resonance imaging [MRI]), had a prior pathogen identification (thorough radiographic fluoroscopic-guided needle biopsy and culture), and who agreed to participate and signed written informed consent. Patients with morbid obesity or malnutrition or immunodeficiency were excluded and those participants with incomplete follow-up, incomplete chart information, or who requested to leave were eliminated from the study. The diagnosis of spondylodiscitis was based on clinical (disease symptoms), radiological changes (bone degeneration), laboratory (serum inflammatory markers), and microbiological (pathogen detection) findings. 4 Simple randomization was performed with the use of a Web-based system that enabled computer-generated random treatment assignment. One senior orthopedic surgeon specialized in spine performed all trial surgeries.
Data collection
Demographic data, patients’ history, clinical symptoms, radiological changes as well as pathogen identification, were collected. The Charlson Comorbidity Index was calculated for all patients. 11,12 This index evaluates comorbid conditions as an independent predictor of surgical mortality (scored from 1 to 6; higher scores indicate more surgical mortality) and long-term survival. 13 Also, initial serum inflammatory markers (C-reactive protein, [CRP] and erythrocyte sedimentation rate, [ESR]), and initial spinal kyphosis or lordosis, measured by the Cobb method in lateral projection x-rays, or sagittal sections in CT-scan or RMI, were noted.
Surgical technique
The surgical approach depended on the affected spinal segment. Patients with a thoracic and/or lumbar infection were approached through staged anterior and posterior procedures, whereas patients with cervical lesions were approached only through anterior instrumentation. Spinal cord or thecal sac decompression and radical debridement of all infected and necrotic tissue, including the infected vertebral body and disc, were performed. Corpectomy was extended backward to the healthy bleeding bone to allow subsequent bone fusion and tissue healing. Then, the structural freeze-dried allograft alone or combined with autograft was placed in the corpectomy site. Our institution’s bone and tissue bank provided the structural freeze-dried allograft. The autograft source was from the patients’ ribs or spinous process. The medullary canal of the allograft used was filled with autologous bone (ribs or spinous process) as described by Munting et al. 14 and Chang et al. 15
The surgical approach, the vertebral level fixation (single or multiple), the type of implant, and the type of autograft and allograft employed were recorded. Also, the operating time, evaluated from initial surgical incision to the closure of the surgical wound, the mean blood loss before and after spinal instrumentation, and intraoperative transfusions were noted. Kyphosis/lordosis correction was achieved immediately after surgery and acute complications were also recorded.
All patients received integral management with antimicrobial target therapy as soon as the pathogen was detected (before spinal surgery). Target therapy was established by specialists in infectious disease from the Department of Internal Medicine of our institution. Patient follow-up was at 3, 6, and 12 months after surgery.
Outcomes
The primary outcome was the grade of spine bone allograft integration on the scale of Tan et al. 16 (which ranges from 1 to 4, with lower scores indicating better fusion rate). A CT-scan was performed at the 26th and 52nd week and a blinded radiologist evaluated the CT-scan and classified it according to its respective bone fusion grade.
The secondary outcomes were radiological, laboratory, and clinical. The radiological outcome was the correction of kyphosis initially caused by the destruction of the vertebral body due to the spinal infection; this was measured by the Cobb method before and after the surgical procedure. Mean grade results were calculated per group, and then the respective kyphosis/lordosis correction was calculated. Laboratory outcomes evaluated the response to antimicrobial therapy using the decrease in CRP and ESR inflammatory markers as a follow-up. 17 Clinical outcomes were evaluated by the visual analog scale (VAS-10 cm), 18 the Oswestry Disability Index (ODI; which ranges from 0 to 100 with higher scores indicating more severe disability) 19 and the Frankel classification (range from A to E, with lower scores indicating more severe spinal cord injury) 20 and were compared with baseline (before surgery) and final (one-year after surgery) values.
Statistical analysis
Data are expressed as median and range (min-max) or as frequencies (n) and percentages (%). Categorical variables were analyzed with the Chi-square test or Fisher’s exact test, and quantitative variables were analyzed with the Mann–Whitney test (between-group comparisons) or Wilcoxon matched-pairs signed-rank test (intra-group comparisons). Statistical tests were performed by GraphPad Prism Software v5.00 (GraphPad Software, La Jolla, CA, USA). A p-value ≤ 0.05 was considered significant.
Results
Participants
A total of 38 patients were evaluated for eligibility. Fifteen patients were excluded for different reasons. We randomized a total of 23 patients, and during the period of study three more patients were lost, two in the group of freeze-dried allografts plus autograft and one in the group of freeze-dried allografts. At the end of the study, a total of 20 patients were evaluated (Figure 1).
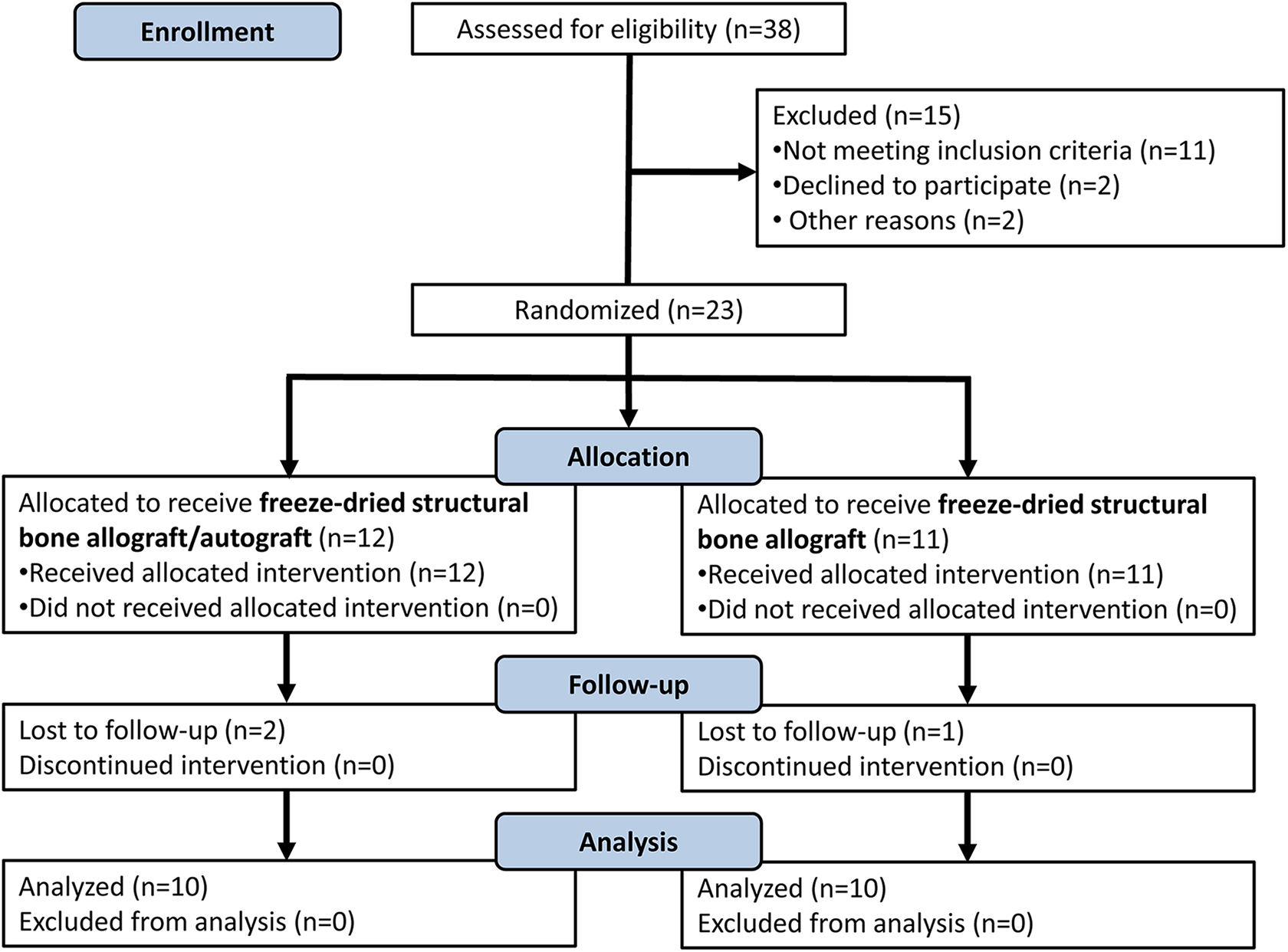
Flow chart of patients included in our study.
There were 13 (65%) men and 7 (35%) women with a mean age of 47.2 (±14.3) years. The demographic analysis did not reveal significant differences between the two groups. The most frequently pre-existing disease observed was type 2 diabetes mellitus in 7 (35%) patients, followed by pulmonary tuberculosis in 1 (5%) and 1 (5%) patient who had previous spine surgery. The Charlson Comorbidity Index Score was similar (p = 0.5578) in both treated groups. Affected segments were more frequently the thoracic 9 (45%) and lumbar 6 (30%) areas. The initial spinal deformity was predominantly greater in kyphosis, with 19 (95%) cases. The most frequently found pathogen was Staphylococcus aureus in 6 (30%) patients, followed by Mycobacterium tuberculosis in 5 (25%). Complete patient characteristics are presented in Table 1.
Demographic data of patients.

BMI, body mass index; CCI, Charlson Comorbidity Index.
Data are presented as median and range (min-max) or as frequencies (n) and percentages (%) for demographic data. *Chi-square; †Mann–Whitney test; f Fisher’s exact test.
Surgery outcomes and complications
No differences were found in the surgical time between the two treated groups even though the surgeries in Group 2 required less time (p = 0.1854). However, the average blood loss during surgery was higher in Group 1, finding a statistically significant difference (p = 0.0222) when compared with Group 2. As a consequence of this, the blood transfusion rate was also higher in Group 1 is statistically significant (p = 0.0198) when compared with Group 2.
Three acute postoperative complications occurred: meningitis in 3 (15%) patients, 2 (10%) were caused by coccidioidomycosis and 1 (5%) case by tuberculosis; 1 (5%) patient had implant failure and in the last 1 (5%) case, wound dehiscence occurred. The patients with meningitis received clinical management according to our specialists in infectious disease from the Department of Internal Medicine and were finally resolved. The patient with implant failure was operated on again and resolved. The patient with dehiscence was managed by secondary closure of the wound and resolved. The complete results of surgery and complications are presented in Table 2.
Spine surgery outcomes.

N/A, not applicable.
Data are presented as median and range (min-max) or as frequencies (n) and percentages (%) for spine surgery outcomes. *Chi-square; †Mann–Whitney test; f Fisher’s exact test.
Primary outcomes
Similarly, satisfactory bone graft fusion grade was observed in both groups at 1 year after surgery (p = 1.000). Complete fusion (grade 1) was achieved in 8 patients in each group (80%). Partial allograft fusion (grade 2) was achieved in 4 (20%) patients, 2 in each group; no additional symptoms were observed in these patients (Table 3).
Bone allograft fusion grade at 12 months after surgery.
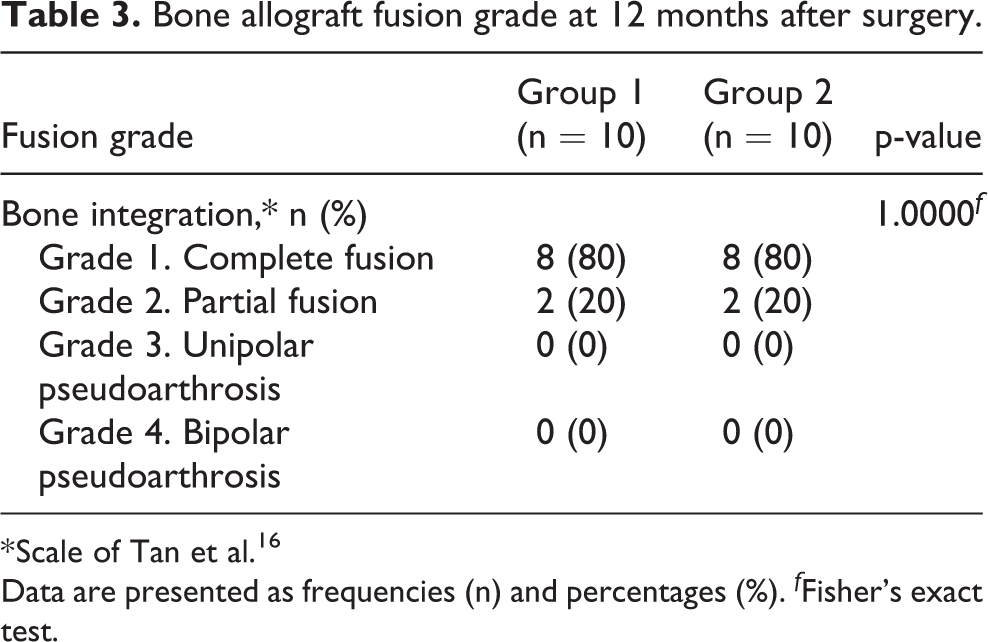
* Scale of Tan et al. 16
Data are presented as frequencies (n) and percentages (%). f Fisher’s exact test.
A preoperative MRI of one patient in which spondylodiscitis could be diagnosed due to its radiographic changes (vertebral body bone destruction) in L1/L2, was treated with posterior spinal instrumentation and freeze-dried allograft alone. One year after surgery, in a lumbar CT-scan, the bone fusion achieved was grade 1 according to the scale of Tan (Figure 2).

Patient with spondylodiscitis. (A) Lumbar MRI in sagittal view before surgery, in which spondylodiscitis could be diagnosed, 50% of the vertebral body is destructed in L1/L2. Surgery with posterior spinal instrumentation and freeze-dried allograft alone was performed. (B) Lumbar CT-scan 1 year after surgery, the grade of fusion observed is grade 1 according to the scale of Tan.
Secondary outcomes
Radiological outcome revealed a similar (p = 0.7292) kyphosis/lordosis correction in both groups. Similar values were observed between both groups before and after surgery. No, statistically differences were observed when an intra-groups comparison was realized (Table 4).
Kyphosis/lordosis correction according to the Cobb method.
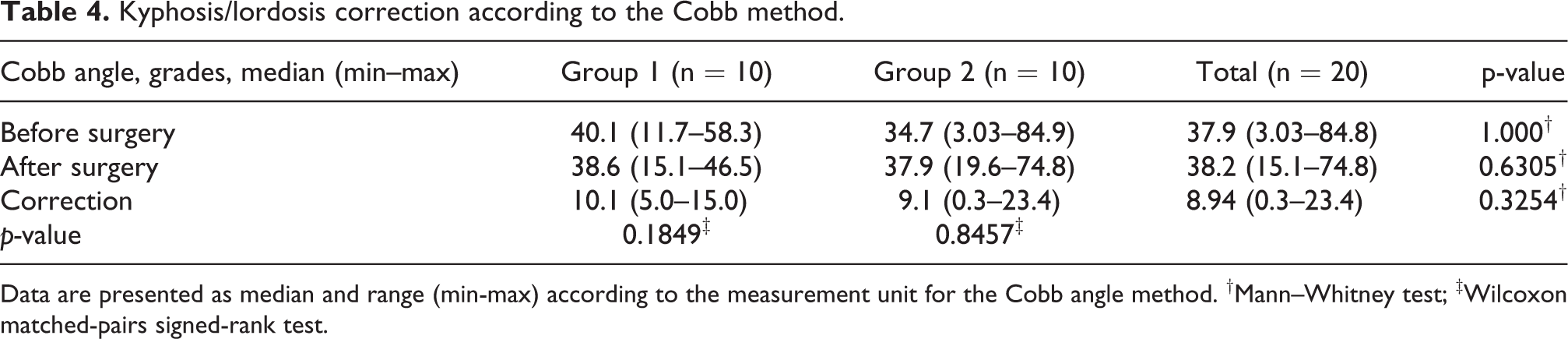
Data are presented as median and range (min-max) according to the measurement unit for the Cobb angle method. †Mann–Whitney test; ‡Wilcoxon matched-pairs signed-rank test.
Laboratory outcomes indicated similar initial values of CRP (p = 0.7052) and ESR (p = 0.4715) levels in both groups at baseline. After surgery, CRP and ESR levels decreased statistically significant among time (3, 6, and 12 months). A statistical significance difference (p = 0.0045) in CPR values was observed when comparing both groups at 12 months. No statistically significant difference in ESR values was observed when comparing both groups at 12 months (Figure 3(A) and (B)).

Laboratory outcomes: serum inflammatory markers. (A) C-reactive protein (CRP) and (B) erythrocyte sedimentation rate (ESR) during follow-up. Data are presented as mean and 95% CI. *p = 0.0045; Mann–Whitney test (between-group comparison). #p < 0.01; Friedman test with Dunn’s Multiple Comparison Test (intra-group 1 comparison). §p < 0.01; Friedman test with Dunn’s Multiple Comparison Test (intra-group 2 comparison).
Clinical outcomes (pain, functional disability, and spinal cord injury recovery) reported similarly high levels of pain before surgical treatment (p = 0.594) and similarly low levels after one-year post-surgery (p = 1.0964) in both groups. However, a statistical significance difference (p < 0.0001) in pain levels was observed when an intra-groups comparison was realized. Functional disability proved to be similar (p = 1.0000) before surgery, in which 16 (80%) patients had initial severe disability. One year after surgery, an improvement could be observed in both groups (p = 1.0000), there was no severe disability, but moderate disability was observed in 10 (100%) patients in Group 1 and 9 (90%) patients in Group 2. Patients’ initial (before surgery) spinal cord injury was similar in both groups (p = 0.1229), all the cases presented as an incomplete lesion. After 12 months after surgery, spinal cord injury recovery was similar (p = 0.1393) in both groups, 14 (70%) patients reported free of neurological symptoms. Complete clinical outcomes are presented in Table 5.
Clinical outcomes.

ODI, Oswestry Disability Index; VAS, Visual Analog Scale.
Data are presented as median and range (min-max) according to the measurement unit for pain outcome and as frequencies (n) and percentages (%) for disability and spine cord injury recovery outcomes. *Chi-square; †Mann–Whitney test; ‡Wilcoxon matched-pairs signed-rank test; f Fisher’s exact test.
Discussion
An adequate radiographic and clinical evolution of patients with spondylodiscitis and vertebral destruction was observed when was treated with cortical allograft freeze-dried alone, similarly when an autograft was applied; some additional advantages of the use of allograft alone has diminished bleeding during the surgical procedure and less blood transfusion. Surgical treatment of an infectious process in the spine usually requires the use of a bone graft as support. In the past, the use of allografts (mainly freeze-dried) as substitutes for the affected segments had a low integration rate, and this problem supposed an aggregated complication for these patients. 9 This might be due to the use of bone allografts without associated instrumentation since the correction of segmental kyphosis is less efficient. 10 The instrumentation used for stabilization depends on the affected segment; in the cervical spine, plates are used, and in the thoracic or lumbar spine, posterior instrumentation is used to stabilize the bone graft. 21 –23 A retrospective report of 21 patients with pyogenic vertebral osteomyelitis, treated with a titanium mesh cage combined with allograft chips and demineralized bone matrix showed a good radiographic evolution in the correction of kyphosis and without instrumentation failures at ≈3-year follow-up, but no bone allograft integration was analyzed. 24
The spine instrumentation provides stable fixation, allows early ambulation, rehabilitation, promotes spontaneous healing mechanism, and has been shown to have an increased rate of bone allograft integration with good results in patients with spinal infections at ≈2 years follow-up. 10,25,26 In an attempt to improve allografts integration therapy, a combination of structural allograft and autograft has been used. A recent systematic review compared different bone grafts used in lumbar spinal fusion including the iliac crest bone graft (autograft), local autograft (spinous process), or allograft in patients with degenerative joint disease. They conclude similar efficacy in fusion rates, functional outcomes, and pain scores; however, this study does not include cases with spinal infections. 27 An et al. performed a retrospective study of 15 patients with pyogenic lumbar discitis treated with posterior lumbar interbody fusion with either allograft and autograft combination or allograft alone, finding an adequate bone consolidation in an average of 15.2 weeks, at ≈2 years follow-up. 25 Dobran et al. 28 reported good stability and restoration of neurological impairment in 18 patients with pyogenic spondylodiscitis treated with posterior pedicle screw fixation without formal debridement of the infected tissue, and compared allograft transplantation alone or bone graft with both the allogeneic bone and the autologous bone; however, the type of the allograft used was not reported. 27
The use of autograft (spinous process or laminae) has been reported in 48 patients with pyogenic spondylodiscitis treated with long posterior instrumentation with or without posterior decompression and autogenous bone graft mixed with tobramycin impregnated calcium sulfate pellets, at 6 months success bone fusion was evaluated in X-rays and correction of kyphotic angle of 8.5° (±6.3°). 29 These autografts are referred to as local autografts, and it is not necessary to perform another surgical approach to obtain the bone graft. In our study, both groups of patients showed an acceptable fusion grade, being grade 1 or 2 on the scale of Tan. The patients with partial fusion (grade 2) did not show any associated instability symptoms. We adhere to a CT-based classification to evaluate the spinal allograft fusion, 16 unlike the previously mentioned observational studies in which bone consolidation was evaluated by less objective instruments. Although the mean correction of the Cobb angle was 8.94 (±3.40), this correction re-established normal to quasi-normal spine biomechanics in most of our patients. It should also be noted that while most of the knowledge regarding the use of autografts, allografts, or their combination to treat spinal infections come from observational studies, our results are derived from a randomized controlled trial that implicates a higher quality level of evidence.
The different laboratory studies used to evaluate patients with spondylodiscitis are unspecific. 30 The CRP is elevated in the large majority of patients with spondylodiscitis and has been suggested as the preferred marker for monitoring treatment response. 31 The normal CRP concentration in healthy human serum is usually <1 mg/dL, increases with age, and higher levels are observed in inflammation, infections (viral or bacterial), and burns. 32,33 The ESR is a sensitive marker for infection and is elevated in >90% of patients, but it is nonspecific and has no relationship with the severity of the infection. 31 The ESR is useful to rule out infection because it is unlikely that an infection is present if the ESR is within normal limits. 30 The mean value of CRP in our patients was 20.3 mg/dL independent of the pathogen, whereas the ESR has a mean value of 28.4 mm/h during the follow-up period. After the treatment, we observed decreased levels of both markers, and even though these two values were not yet at normal levels, the patients did not show evidence of residual infection.
A systematic review reported that 6 weeks of antibiotic treatment have similar mortality, relapse, and failure rate as 12 weeks of treatment. 34 This recommendation was followed in our patients. As reported in the literature, S. aureus is considered to be the most common bacterial pathogen that causes osteomyelitis and accounts for about half of non-tuberculous infections. 35 This pathogen was identified in a third of our patients, while the second most common infection (a quarter of our patients) was caused by M. tuberculosis.
We intended to evaluate the minimum clinically important difference (MCID) in our patients, but there are no reports focused specifically on patients with a spinal infection. Parker et al. 36 reported the MCID for the VAS in 2.0 to 3.2 points and the ODI in 4–16.6% in patients with symptomatic pseudo arthrosis. Considering the a fore mentioned MCID, all of the patients showed a meaningful improvement in pain, disability, and spinal cord injury recovery at 1 year of follow-up.
We identify several limitations of this study. First, the population available for the final analysis in each group was small, but as reported in the literature, one of the common limitations observed in this kind of studies it is the small sample size and they have been mostly evaluated in retrospective cohorts. 37 Second, we used anterior stabilization with plate, posterior screws, or Luque bars according to the level of affection and as we know, the biomechanics of the spine is different according to the involved segment. Nevertheless, other studies have reported different spine-affected levels (thoracic and lumbar) in pyogenic spinal infections and evaluated them as retrospective cohorts with a combination of bone auto and allografts as treatments. 25,28 As mentioned, several affected levels and different kinds of allografts were used in our study. Similarly, Munting et al. 14 included several diagnoses in different levels of affection which were treated with several kinds of allograft. Notwithstanding these variabilities, an adequate bone integration of the allograft was showed. Lu et al. 38 evaluated patients with vertebral osteomyelitis with several levels of affection, and infection by several microorganisms (S. aureus, M. tuberculosis, Coccidioides immitis) compared bone autograft with bone allograft, with no differences between groups. Moreover, we decided to include patients with tuberculosis, as our objective was to evaluate bone integration of the allograft in spine infections. One of the main differences in the management of patients with spinal tuberculosis is the antibiotic therapy used, while for the stabilization of the spine, the bone graft and spinal instrumentation used is the same as in other types of infection with vertebral destruction. 39
Our study was a prospective, randomized, controlled, blinded trial, in which 86.95% of our enrolled patients had complete follow-up. After a year, we did not observe any re-infections in our study patients.
Conclusions
In conclusion, our results demonstrated that freeze-dried bone allografts alone could be a therapeutic option for spinal fixation surgeries due to spondylodiscitis. In terms of bone fusion, deformity correction, postsurgical complications, control of infection, and clinical improvement were achieved in both treated groups. By avoiding autograft procurement, the mortality rate, surgical time, blood loss, and transfusion rate, as well as economic aspects associated with the surgical procedure could be decreased. The results of this study must be confirmed in larger clinical trials.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.