
Abstract
While the pathological manifestation of atlantoaxial rotatory dislocation has been well described in the medical literature, the combined dislocation of the atlantoaxial and atlanto-occipital joints, or OAARD – short for occipital-atlantoaxial rotatory dislocation – is a condition which has been poorly elucidated and probably underdiagnosed. We believe that the pathogenesis of combined atlantoaxial and atlanto-occipital dislocation is most likely a result of untreated atlantoaxial rotatory dislocation leading to chronic secondary compensation measures occurring at the occiput-C1 joints. Unique clinical and radiological features lead to difficulty in diagnosis, and conventional treatment algorithms may not apply. This paper describes a combination of clinical and radiological features which can help clinicians correctly diagnose and treat OAARD.
Introduction
Background
The craniocervical and atlantoaxial articulations represents a unique and complex set of structures consisting of bony articulations, ligamentous stabilizers, and synovial linings. 1,2 While these structures normally interact with each other to allow the harmonious movement of neck flexion-extension and rotation, disturbances to one or more of these structures could lead to pathological subluxations or fixed dislocations, causing pain, deformity, functional loss, and in serious situations neurological compromise. The syndrome of atlantoaxial subluxation was first documented in 1830 by Sir Charles Bell, and subsequently popularized after Pierre Grisel described a series of patients with pharyngitis and torticollis presenting with dislocation of the C1–C2 joint. 3 In this eponymous syndrome coined by Grisel, children typically under the age of 12 years present with torticollis following upper respiratory tract infections or surgical procedures of the head and neck. 4 The condition of Grisel syndrome with concomitant rotational dislocation at the occiput-C1 level is in fact not uncommon, but has been poorly described in the current available literature.
Anatomical foundation
Atlantoaxial motion
Normal atlantoaxial joint motion contributes up to 60% of skull rotation, and this is made possible by the articulation between the unique ring-like structure of C1, and peg-like structure of C2. Following the initiation of skull motion by the sternocleidomastoid muscle (SCM), the atlantoaxial relationship passes through three phases of motion. 5 This is important to understand for the diagnosis of C1/2 rotatory subluxation.
In the first (single-motion) phase, C2 remains stationary until C1 rotates to 23 degrees; this is made possible by a normal physiological subluxation of C1/2. In the second (double-motion) phase, C2 begins to rotate and is yoked by the skull through the strong alar ligaments; thus C1 and C2 rotate together but C1 moves at a greater rate. In the final (unison-motion) phase, when C1/2 rotation difference is at 45 degrees, C1/2 ligaments become taut and both vertebrae rotate at the same rate. Further neck rotation from 65 to 90 degrees occurs at segments below C2. 5
Occipital-C1 motion
The atlas carries the skull on the well conformed occipital-C1 joints at each side. As the atlas does not itself have any independent muscle action, skull rotation relies on the powerful turning moment created by the sternocleidomastoid (SCM) muscles on each side. The rotation of the skull to one side is caused by contraction of the contralateral SCM, and the ring of the atlas is passively driven into motion by a ‘cranking’ action that the skull exerts. The normal occipital-C1 joint in children is tightly held together by strong ligaments, and there is great left-right asymmetry in the conformation of this articulation. The occipital condyle-C1 interval (CCI) is normally constant in both the sagittal and coronal planes and should be less than 2 mm when measured on high-resolution computed tomography (CT). There is no significant change with age from birth to 18 years, and CCI is also not affected by congenital anomalies of the C1 arches, odontoid, clivus, and foramen magnum. 6,7 In terms of rotational motion, there is very little relative motion between C1 and the occiput during normal head rotation, and the separation angle should be less that 3 degrees even up to 65 degrees of head turning. 5 It is worth mentioning, however, that ligamentous laxity is not uncommon in children, and the normal stressed limits of CCI in dynamic situations have not been defined.
Concomitant atlanto-occipital and atlantoaxial dislocation
While the pathological manifestation of atlantoaxial rotatory dislocation has been well described in the medical literature, 3,5,8 –14 the combined dislocation of the atlantoaxial and atlanto-occipital joints, or OAARD – short for occipital-atlantoaxial rotatory dislocation – is a condition which has been poorly elucidated and probably underdiagnosed. In the available literature there have been only nine cases reported, 11,15 –21 and this radiological feature was also present in a subgroup of chronic AARD cases reported by Pang and Li in 2005. 9 We believe that the pathogenesis of combined atlantoaxial and atlanto-occipital dislocation is most likely one of chronic compensation of the occipital-C1 joint, rather than initial double dislocation. Without deliberate attention paid, these radiological features may be difficult to identify, and normal treatment algorithms may not apply. Finally, the long-term outcome of both conservative and surgical management has not been well described.
Case presentation
An 11-year-old girl first presented to a general practitioner with neck pain and torticollis, without preceding upper respiratory tract symptoms or trauma. The diagnosis of atlantoaxial rotatory dislocation was not identified at the time. The patient attended multiple sessions of physiotherapy, and gradually regained a normal forward gaze. However, over the course of the subsequent few weeks the patient experienced repeated bouts of acute neck pain and spasm, and experienced a great deal of limitation in activities in daily living because of her symptoms. She was eventually referred to us for further management.
Clinically the patient had a neutral head posture but had limited bilateral rotation to approximately 45 degrees without any obvious head tilting. There was upper posterior neck tenderness on end range of rotation to the left side. Bilateral sternocleidomastoid muscles were not spastic and the patient did not have any neurological deficit. Radiologically, open mouth view X-ray showed an asymmetric lateral atlanto-dens interval and gross overlapping of the C1 lateral mass shadows with the C2 facets (Figure 1(a)). Dynamic CT scans confirmed a Fielding type 1 fixed atlantoaxial rotatory dislocation, with left C1 lateral mass dislocated anteriorly and C1/2 separation angle of 51.6 degrees in neutral head position (Figure 1(c) and (d)). Interestingly, the C1 ring was also dislocated with reference to the skull, forming an occiput-C1 separation angle of 40 degrees, signifying a concomitant occipital-C1 dislocation in the counter direction (Figure 1(b)).
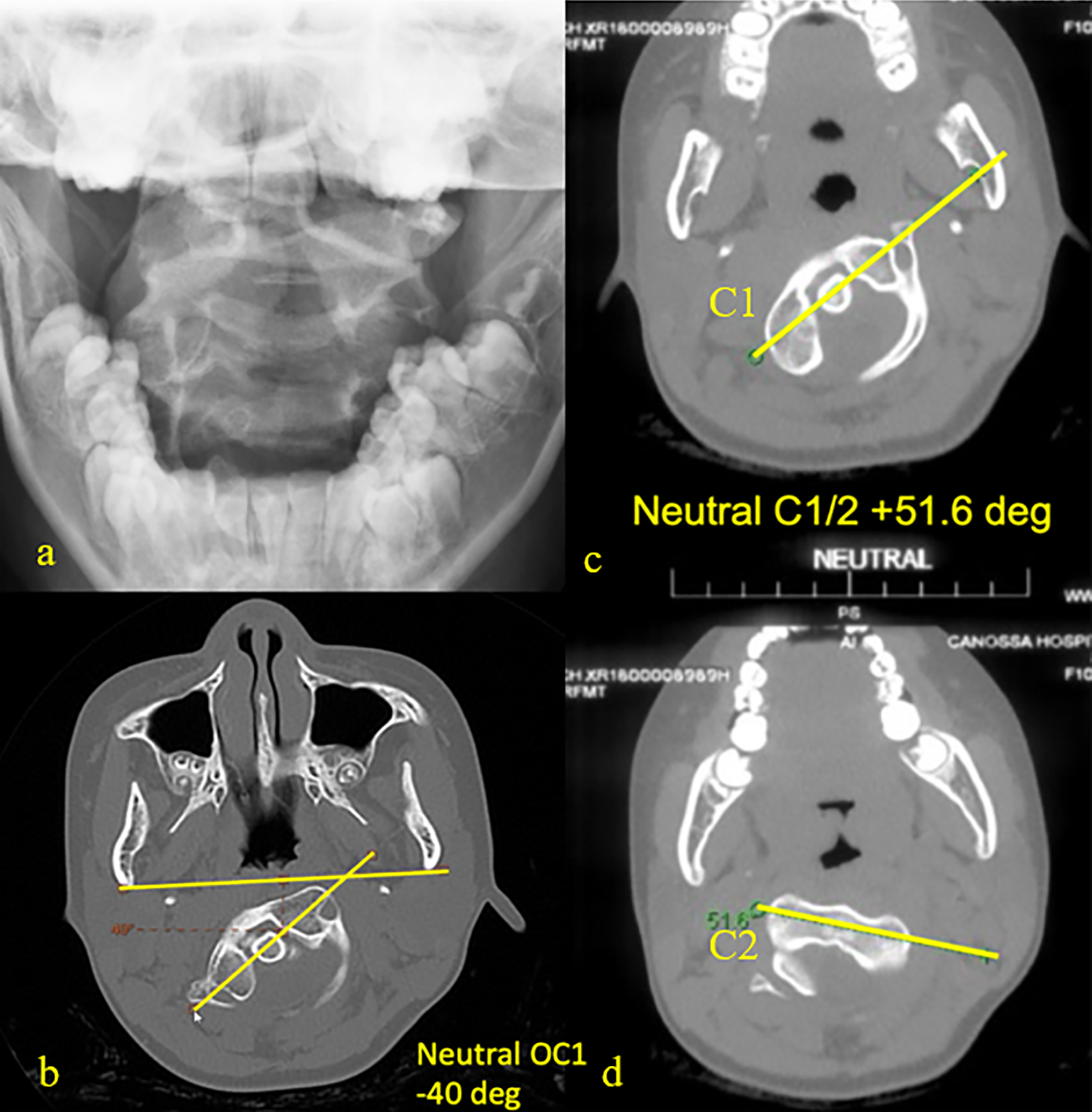
(a) Open mouth view on presentation, (b) occiput-C1 rotational relationship (negative value denotes rotation counter to C1/2 dislocation), (c and d) C1/2 rotational dislocation.
The patient eventually underwent halo-traction up to ×10 kg for 3 weeks, but this failed to reduce the C1 dislocation and a dynamic CT scan demonstrated a persistent double dislocation and locked C1/2 motion on head turning. Treatment options were discussed with the family including fusing C1/2 in best-reducible position followed by an additional period of halo-vest immobilization for the occiput-C1 dislocation, or directly fusing occiput to C2. The patient’s family hoped to preserve occiput-C1 motion and therefore she eventually underwent a posterior open reduction of C1/2 with instrumented fusion, followed by 3 months of post-operative halovest immobilization. The patient recovered uneventfully and solid fusion was achieved at 3 months post-op. At 1 year the patient experienced no significant symptoms relating to the cervical spine, had bilateral head rotation of 60 degrees and did not report any restriction in activities of daily living. Reassessment dynamic CT scan at 1.5 years showed remodelling over the occipital-C1 joints, with satisfactory conformity achieved in neutral and bilateral head rotation (Figure 2).

OAARD patient at 1.5 years after C1/2 fusion, with solid C1/2 fusion and bilateral occipital-C1 joints showing remodelling with good conformity.
Discussion
Pathophysiology
We believe that most of OAARD start with the more common AARD, where patients typically present with torticollis and neck pain. If not recognized early, secondary compensation measures occur at the occiput-C1 joints over time, leading to counter-dislocation that brings the head position either partially or even completely to the centre once again. In some instances, this may be mistaken as having clinically ‘resolved’ atlantoaxial rotatory subluxation. Factors such as neck manipulation and intermittent traction are possible attributing factors to this phenomenon. 21
Like in the case illustrated above, the child may have a forward-facing head upon examination, but rotation is usually limited due to locked atlantoaxial motion. In this situation rotational motion is contributed primarily by the subaxial cervical segments, and the pathological occipital-C1 rotation. This hypothesis is supported by Pang’s published series of AARD, 9 where we saw the mean occipital-C1 rotation increased from 5 degrees in acute cases of AARD to over 30 degrees in chronically unreduced cases, suggesting a progressive compensatory process with increased chronicity, likely secondary to the patient’s subconscious and persistent effort to counteract a misaligned visual axis.
Radiological features
Plain radiograph
While a standard radiograph of the cervical spine may not be sufficient to properly visualize the rotational changes at C1 and C2, there are tell-tale signs on a lateral cervical X-ray which may be useful. One of which is what we have termed the radiological sign of “trapezoidal anterior C1 shadow” (Figures 3 and 4), which represents the lateral mass of C1 translated anteriorly and occupying the normal position of the anterior C1 arch. This is visualized as a trapezoidal bony contour on the ventral aspect of the odontoid peg and is a useful sign for recognizing abnormal rotation of C1.

Illustration of trapezoidal anterior C1 shadow using 3D printed model and digital X-rays. (a) The normal and (b) oblique lateral profile of the lateral mass of C1. Digital X-ray projection of C1/2 relationship in (c) normal reduced position and (d) dislocated position.
‘Trapezoidal anterior C1 shadow’ in a patient with AARD.
In addition to rotation, in a well taken true lateral X-ray (where bilateral subaxial facets are well overlapped with each other), one may also appreciate the abnormal tilting of the C1 ring by looking for the ‘oval posterior arch sign’ (Figure 5).

‘Oval posterior C1 arch’ sign.
If there is a clinical suspicion of AARD or OAARD, then a standard AP radiograph of the cervical spine will not be adequate, and an open-mouth view is mandatory. An asymmetrical lateral atlantodens interval (LADI) should raise suspicion that there is pathological subluxation or dislocation of the ring of atlas over the axis. It is usually possible to discern which lateral mass of atlas has subluxed forward as this will project as larger on the open mouth view (Figure 6).
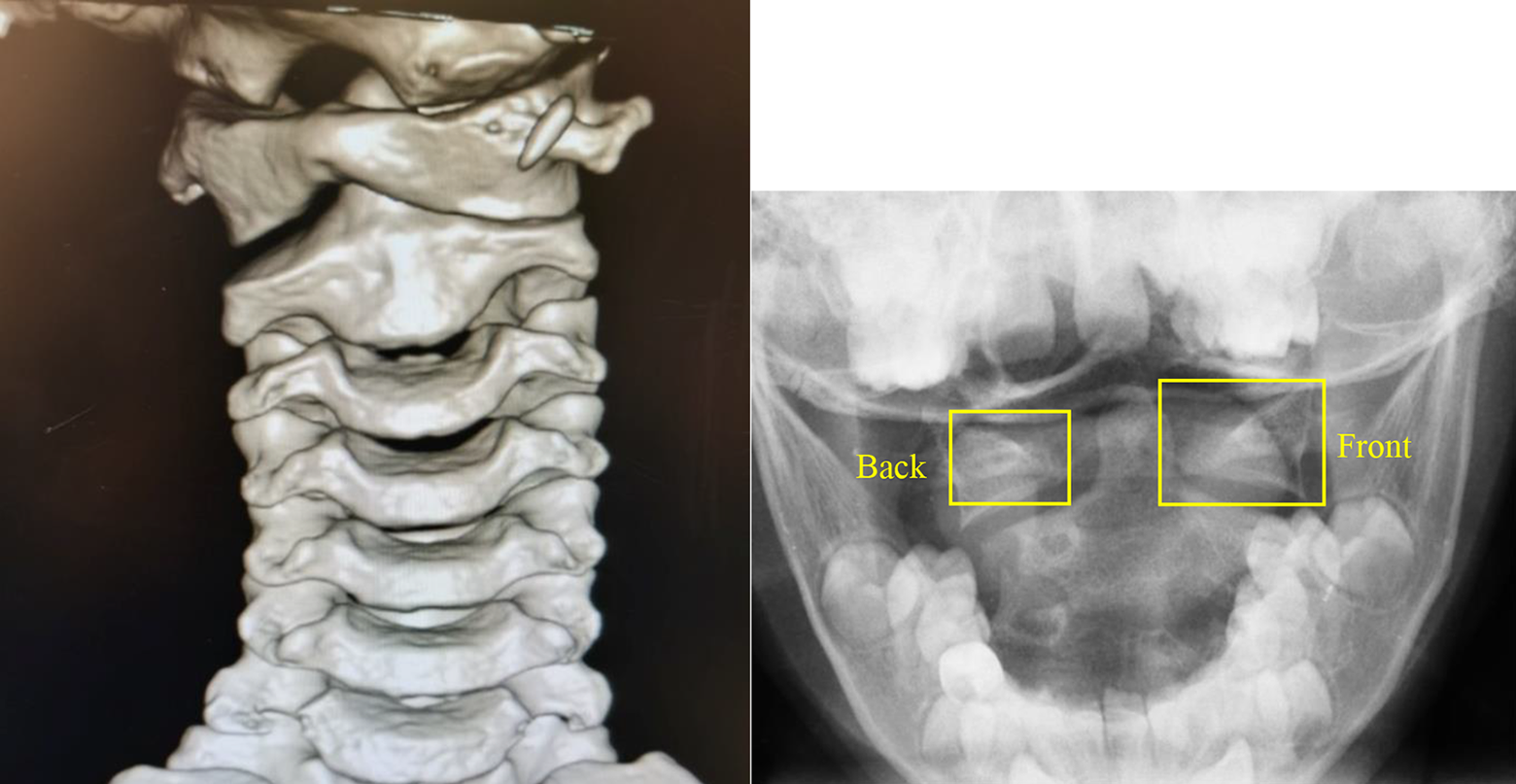
Relative size difference of C1 lateral masses on open mouth view.
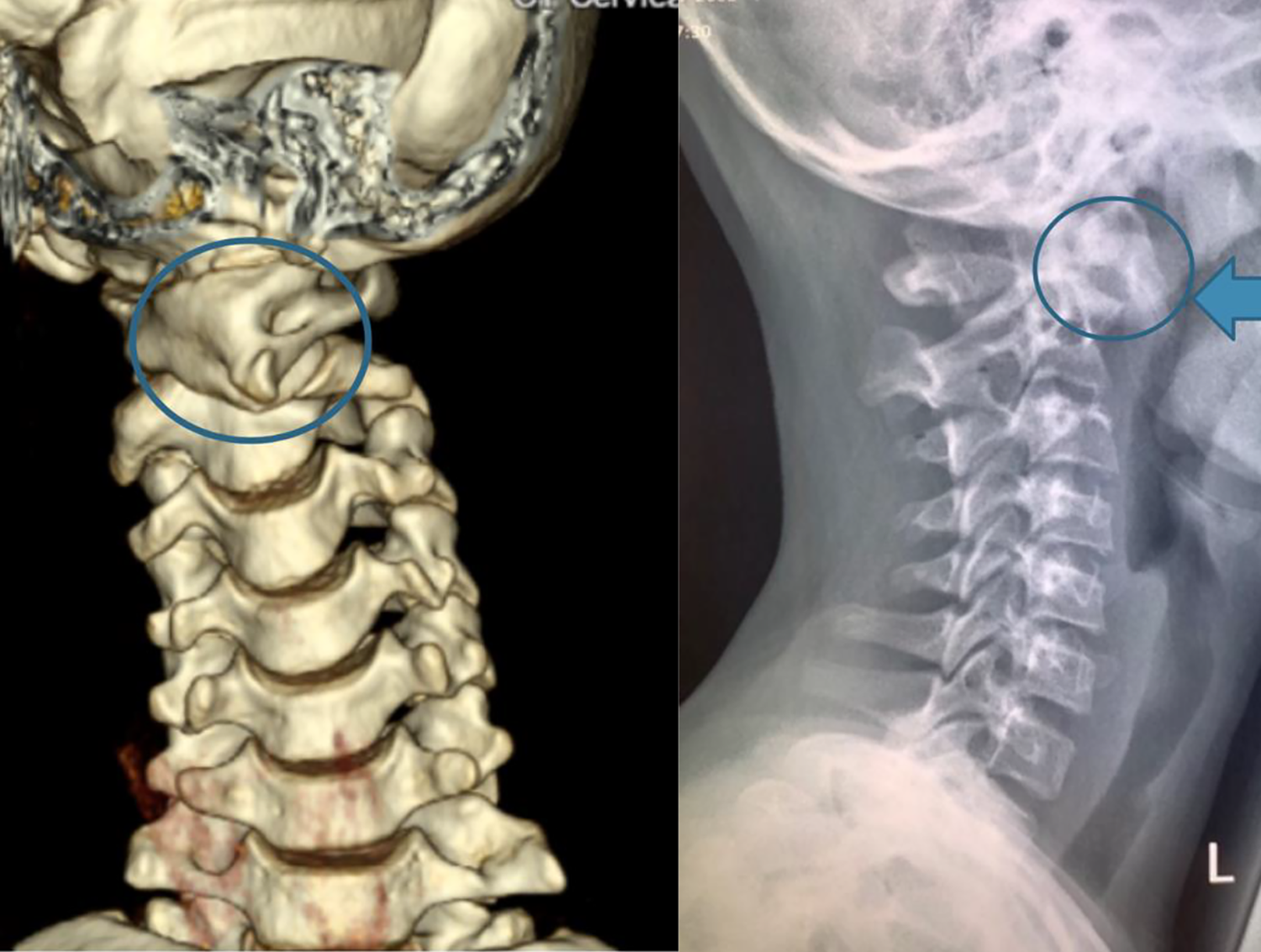
More importantly, a grossly abnormal open mouth view with a central head position should raise suspicion of a concomitant occipital-C1 dislocation in addition to C1/2 dislocation, i.e. OAARD. Rotation of the skull in these cases may be minimal or absent, and this can sometimes be identified by the central position of the nasal septum (Figure 7). We term this radiological phenomenon ‘isolate C1 spin-out’, and this can be readily appreciated on a three dimension reconstructed CT image.

(a) 3D CT scan, and (b) plain radiograph demonstrating ‘isolated C1 spin-out’: severe dislocation of C1 with a centralized skull position.
Computerized tomography (CT)
C1 and C2 relationship
The next stage in imaging is a dynamic plain computerized tomography (CT) scan in neutral and bilateral active rotations of the head. In this dynamic CT scan, any separation of C1 and C2 in the neutral position is pathological and confirms AARD. The separation angle should be measured (Figure 8(b)). One can usually notice an exacerbation of is separation angle when turning away from the side of the anterior C1 dislocation (i.e. exacerbating the dislocation). When turning towards the side of anterior C1 dislocation (i.e. attempted reverse of the dislocation), failure to attain normal physiological subluxation to the contralateral side then confirms locked AARD (Figure 8(a) and (c)).

Dynamic CT scans for rotational deformity (a) exacerbation of dislocation, (b) neutral position, (c) attempted reverse of dislocation (negative value denoting failed normal contralateral rotation).
Three dimensionally reconstructed images and models are very useful for assessing dysplastic changes secondary to chronic subluxation. One should look closely for abnormal sloping of the C2 facet joint surfaces resulting from chronic compression (Figure 9).

(a and b) 3D reconstructed images and (c to e) 3D printed model of the same patient showing deformity of the right C2 facet.
Occipital-C1 and C1/C2 relationship
As the C1 ring carries the skull on its tightly conformed occipital condyles, the direction of the skull should remain always in line with the ring of C1. Any rotational separation between C1 and the skull should raise concern of OAARD. A line joining the posterior angles of both mandibles can serve as a consistent surrogate for the skull position and can be measured against a line connecting the transverse foramina of C1 (Figure 10). Normal separation should be less than 3 degrees. 5

Transmadibular line and C1 transverse line, demonstrating counter occipital-C1 dislocation in OAARD.
Furthermore, sagittal and coronally reformatted images must be assessed for abnormal diastasis of the occipital-C1 joints, which may suggest a more sinister pathology of atlanto-occipital dislocation. The occipital condyle-C1 interval (CCI) (Figure 11) is a direct measure of the occipital-C1 joint integrity has been proposed as one diagnostic method with high sensitivity and specificity for atlanto-occipital dislocation. 6
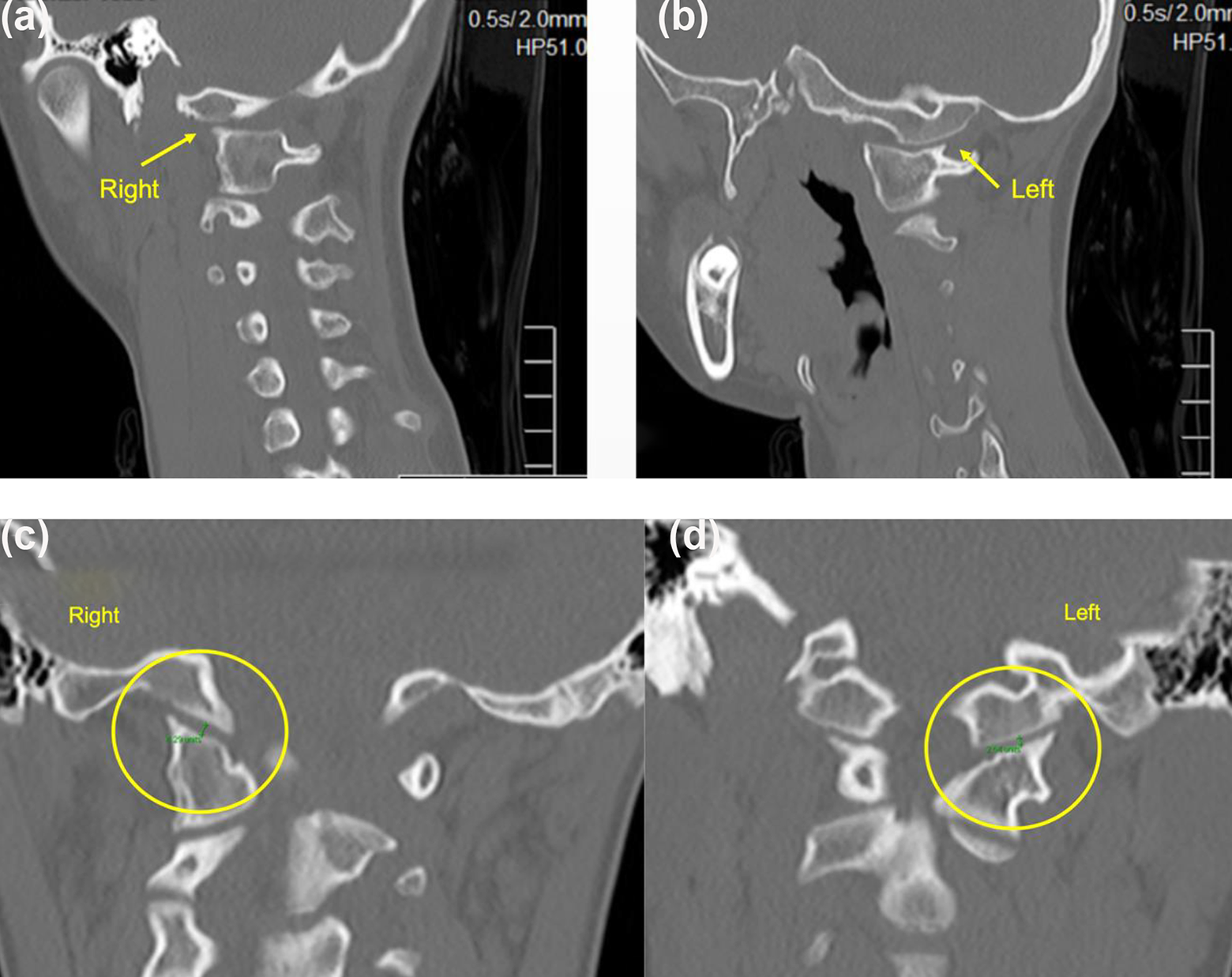
(a and b) Abnormal rotational separation of occipital-C1 joints in OAARD and (c and d) intact CCI in the same patient.
Magnetic resonance imaging (MRI)
Even though MRI is not a standard modality of imaging in OAARD, it may provide useful information in chronic and refractory cases, and especially cases with history of cervical injury. The tectorial membrane – which is a continuation of the upper portion of the posterior longitudinal ligament – should be assessed for its continuity to the clival insertion, and any discontinuation, attenuation, or peri-ligamentous oedema and fluid (Figure 12), may suggest the more sinister pathology of atlanto-occipital dislocation, 6 especially in the context of prior injury. While it is not uncommon for partial attenuation of the transverse atlantal ligament to occur in chronic AARD, rupture of this ligament should be carefully sought as it would represent an orthopaedic emergency, as this may result in devasting spinal cord compression, respiratory compromise or even death.

(a) Tectorial membrane continuity and (b) attenuated transverse atlantal ligament.
Diagnostic pitfalls
Clinical interpretation of head position
Head tilt: Tilt can be a misleading clinical feature in terms of alluding to the direction of dislocation. A tilt can be either a result of bony deformity in the C1/2 facet caused by the forwardly subluxed C1 lateral mass. This gives rise to a classic cock robin deformity in chronic cases, with head tilted to the side of anterior C1 dislocation. Head tilt can also be a result of a contralateral spastic SCM muscle trying to oppose a rotational deformity. This is usually seen in acute and milder cases, with head tilt to the side opposite the anterior C1 dislocation. In the situation of OAARD, head tilt may also be absent as a result of counter occipital-C1 dislocation. To avoid this, we suggest using head rotation as the primary clinical feature to describe the direction of dislocation.
Head rotation: In case of OAARD, a central head position may give a false impression of clinically resolved atlantoaxial subluxation, when in fact the head is brought to neutral by the compensating occipital-C1 joints rotating in the contralateral direction. Clinical head rotation is usually diminished in these situations as the rotation is contributed from subaxial segments and the pathological occipital-C1 counter-rotation. A high index of suspicion is needed to diagnose these cases, and radiological features such as the trapezoidal anterior C1 shadow (Figure 4), asymmetric open mouth view with a central nasal septum (Figure 7) should raise suspicion, and the diagnosed can be subsequently confirmed with a dynamic CT scan.
Exposure of CT scan
If OAARD is suspected, then a CT scan only covering C1 and C2 will not suffice as this does not adequately demonstrate the position of the skull in relation to C1. We recommend that the clinical suspicion of OAARD be communicated with the involved radiologist so that the scan will extend cranially up to at least the mastoid processes, and a line connecting the posterior angles of the mandibles can serve as a surrogate landmark for the position of the skull (Figure 10 above). 1 mm cuts are preferred in order not to miss key anatomical landmarks, and superimposed axial images of the skull, C1 and C2, if can be provided by the radiographer, will be helpful for visualization of separation angles. Having fine cuts on the CT will also be useful for future surgery if navigation is used.
Defining radiological resolution of OAARD
When scrutinizing the effect of attempted active reduction on a dynamic CT scan, it is important to note that return of C1 to central position without normal physiological subluxation to the opposite direction should not be accepted as satisfactory resolution of AARD, as this suggests either a persistent mechanical blockage, or asymmetrical ligamentous tension. If OAARD is present, any attempted active reduction may also give rise to further separation of occipital-C1 joints and this can usually be readily appreciated on CT.
Management principles
Conservative management
With the rare exception of traumatic occipital-C1 and C1/2 dislocations in which neurological structures are at risk, all attempts should be made to preserve the occipital-C1 and C1/2 motion in children. The application and limitations of conservative management should be well understood.
Medical management alone
Published treatment recommendations 13 suggest that acute presentations of AARD within 2 weeks can be treated with collar and NSAIDs alone. While we do not entirely disagree with this recommendation, we strongly believe that a proactive and early aggressive approach tends to give rise to better results, especially in settings where close follow-up is not feasible. Early halter traction, combined with NSAIDs and muscle relaxants, tend to be well tolerated by children and can lead to earlier resolution of the dislocation, and help avoid problems arising from fixed and irreducible deformities later on, including OAARD. In certain clinical settings where immediate set-up of a traction system is logistically not feasible, we recommend weekly follow-ups until clinical and radiological resolution is observed.
Halter and halo-gravity traction
Atlantoaxial rotatory dislocation
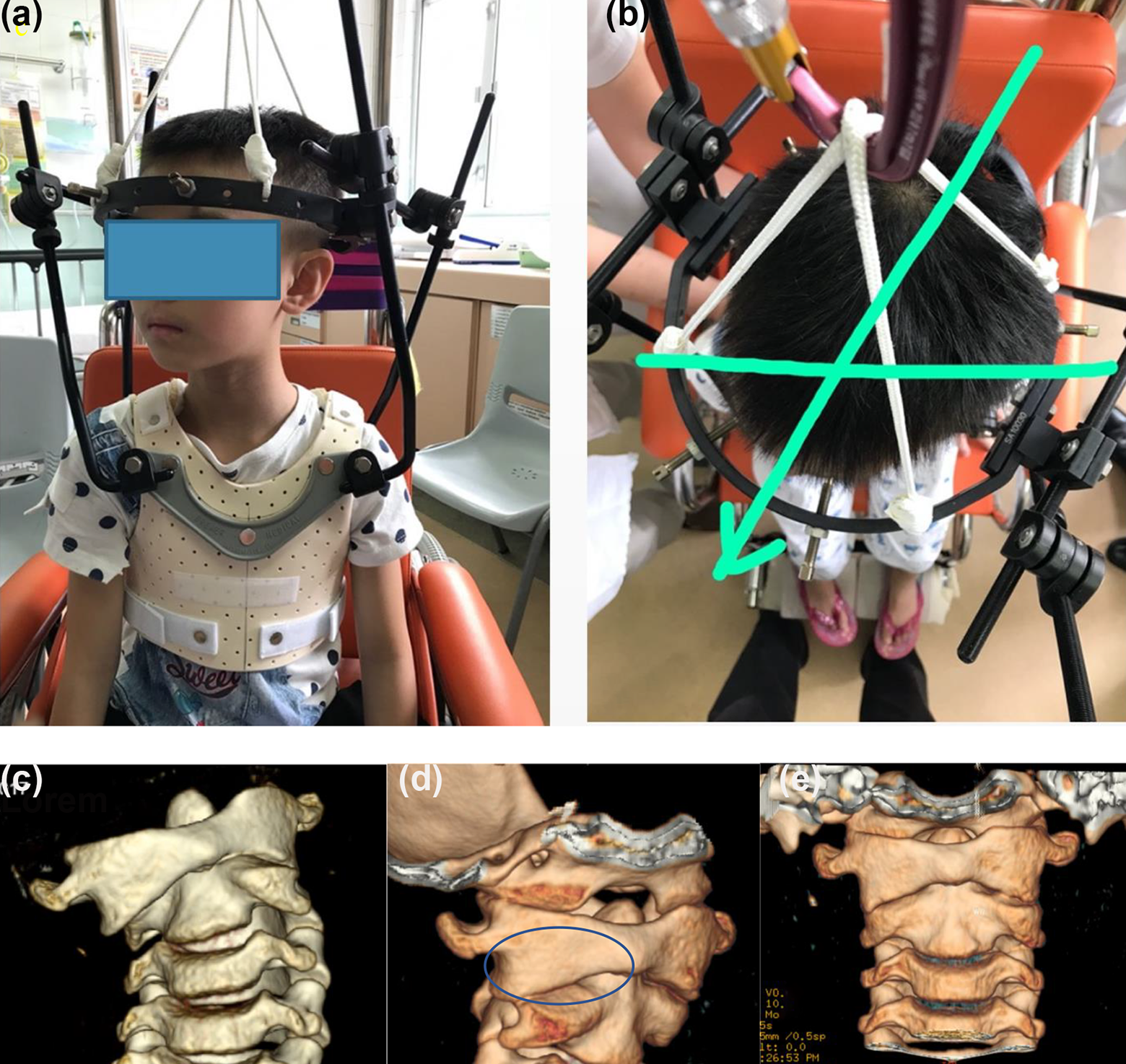
Halter traction is a very useful tool for acute and subacute AARD (Figure 13) and can be easily set up in most hospital settings. Patients are typically placed on 2–3 kg traction for 6–8 hours at a time and allowed short intermittent rests for feeding and bathing. Halo-gravity traction should be considered in chronic presentations and recurrent dislocation cases. Attention must be paid to daily examination of cranial nerves during any form of skull traction. When prolonged traction is required, a halo-chair with reversible pulleys can allow the patient to carry out daily activities outside the confines of the bed and is very useful to mitigate the psychological stress of children undergoing prolonged treatment (Figure 14).

(a) Halter traction set up and (b) C1/2 reduction seen on open mouth view.

Halo-chair with a reversible pulley system.
Occipital atlantoaxial rotatory dislocation
Because of the concomitant occipital-C1 subluxation in OAARD, longitudinal traction forces applied by halter or halo will not be effectively transferred into a rotational force on the C1 ring, and the efficacy of this method to reduce C1/2 dislocations will be diminished. Indeed, for all nine OAARD cases reported in the literature, not one was successfully reduced by traction. 8,15 Because the endpoint for attempting OAARD reduction by method of traction has not been well defined, we recommend conducting a dynamic CT scan with the traction apparatus set up in the CT gantry. In such cases where there is a maintained fixed rotation of C1/C2 while on traction, or persistent occipital-C1 dislocation, earlier surgical intervention may be indicated.
Immobilization in external braces
Atlantoaxial rotatory dislocation
After reduction is attained, external immobilization by way of a cervicothoracic orthosis or halovest is necessary in all cases. The duration is arbitrary and several published guidelines suggest a period of up to 3 months. 9,13 For patients with CT evidence of C1/2 facet deformity prior to reduction, we recommend using an overcorrection brace or halovest so that the deformed facet can be uncovered and allowed to remodel over time (Figure 15). This has been shown to be useful to prevent recurrent subluxation in chronic cases, 14 and overcorrection bracing also has the theoretical benefit of rebalancing the tension of the paired alar ligaments and periarticular soft tissues.
AARD case (a and b) overcorrection applied by halovest, (c) pre-reduction, (d) uncovering of the deformed C2 facet surface by overcorrection immobilization, and (e) reduced and remodelled C2 facet after removal of halovest 3 months later.
Occipital atlantoaxial rotatory dislocation
Due to the fact that occiput-C1 rotation is dissociated in this situation, positioning in an overcorrection brace or halovest could potentially exacerbate occipital-C1 counter dislocation and is not recommended. We suggest that in these case the head be immobilized in a neutral position that best reduces occiput-C1–C2 relationship, without deliberate overcorrection. Any recurrence of dislocation during or after the immobilization period is a surgical indication.
Surgical intervention
Indications of surgery
Rigid surgical fixation is the last resort when it comes to management of AARD and OAARD. The indications for surgery include deformities which are irreducible upon halo traction, and recurrences while in halo or after removal of halo at the endpoint of 3 months immobilization. 9 Specifically in OAARD, the role of non-operative management is diminished as chronic dislocation and dysplastic changes of occiput-C1 joints have already occurred. The surgical strategy is controversial and there is to date no consensus in the published literature.
Various methods of surgical stabilization for C1/2 have been described, including classic methods of Gallie or Brooks wiring, 22,23 or techniques of C1–2 posterior fixation using Harms-Goel technique of C1 lateral mass screws and C2 pedicle or translaminar screws, 24 and Magerl method of transarticular screws. 25 A plate and rod construct is typically used when fusing up to occiput. Special considerations in paediatric patients include immature bone quality, extensive anatomical variability, and smaller osseous structures. 26 The complication rate also varies and has been quoted to be over 60%, including non-union, neurological complications, inadvertent adjacent level fusion, and pedicle or C1 posterior arch fracture during screw insertion. 26 Furthermore, the long-term effects of posterior cervical spine fusion in skeletally immature spine has not been well described.
While it is not within the scope of this article to review the individual techniques of surgical fixation, it is important that the surgeon is aware of the limitations and merits of each approach. Pertinent considerations are discussed below.
Success of pre-operative C1/2 reduction
The method of transarticular screws requires successful reduction of C1 before screw placement and cannot be used in cases of failed reduction by traction. C1 lateral mass screw and C2 pedicle screw technique is a better option in these cases and they allow for intra-operative, direct manipulation of C1 and C2 before fixation. 24 The correct trajectory for C1 lateral mass screws may be difficult to attain if C1 ring reduction is not attained prior to surgery (Figure 16), and as such it may also be difficult to judge the adequacy of reduction intra-operatively by observing screw head position alone. We believe that this may be one situation where computer navigated screw insertion and intra-op CT may be of use. Staged anterior transoral release followed by further traction and subsequent posterior fixation is a method described for irreducible cases and is suggested to be superior to in-situ fusion when considering the long term degenerative changes in the chronically compensated subaxial spine and occipital-C1 joints. 27

Post-operative CT scan showing lack of normal convergence of C1 lateral mass screws due to rotated C1 position at the time of screw insertion.
Choice of fusion levels in occipital-atlantoaxial dislocation
The concomitant counter-dislocation at the occipital-C1 joints presents a management dilemma when it comes to choice of fusion levels and there is to date no consensus on this. To the best of our knowledge, there are only nine previous reports on OAARD. 8,15 Among these nine cases, three required C1/2 fusion, four required occiput to C2 fusion, and two cases went into spontaneous occiput to C2 fusion. Considerations include the uncertain long-term results of occipitocervical fusion in children, the uncertain remodelling potential of the occipital condyles after successful C1/2 reduction and stabilization, and finally the possibility of chronic neck pain resulting from unfused but degenerated occipital-C1 joints. In the absence of sinister radiological features such as discontinuation of tectorial membrane and diastasis of the CCI, one option is for reduction and fusion of C1/2, followed by post-operatively immobilization by halovest for an additional 3 months to allow for occipital-C1 joint remodelling, such as in the case we have shown. While fusion to the occiput is probably the safest option, it comes at the expense of significant reduction of head rotation, as well as flexion-extension. Finally, internal fixation of occiput-C2 without fusion (with subsequent implant removal) remains to be a viable option, however the long-term outcome has not been reported.
Conclusion
Concomitant occiput-atlantoaxial dislocation is a unique condition that is probably underdiagnosed in common daily practice. We emphasize the need for clinicians to exercise a high index of suspicion in children presenting with neck pain and torticollis. Early diagnosis and aggressive treatment of isolated atlantoaxial dislocation may help prevent chronic secondary dislocation at the occiput-C1 level. This paper describes a combination of clinical and radiological features which can help clinicians correctly diagnose and treat OAARD. More research is required on the long-term outcome following upper cervical spinal fusion in children.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.