
Abstract
Background:
Percutaneous insertion of third-generation straight humeral nails is a recent alternative to the conventional open method. Rather than splitting, retracting and subsequently repairing the supraspinatus fibers to visualize the humeral head entry site, the percutaneous approach utilizes a cannulated awl to enter the intramedullary canal through the supraspinatus fibers without visualizing internal shoulder structures. Despite recent evidence demonstrating satisfactory outcomes in the percutaneous method, the potential for iatrogenic injury to the rotator cuff and other shoulder structures is not fully understood.
Materials and Methods:
We performed an anatomical study of 46 shoulders in 23 cadavers to compare damage caused to internal shoulder structures between the open and percutaneous techniques. Dimensions and morphologies of supraspinatus and humeral head perforations were recorded.
Results:
The percutaneous technique produced greater latitudinal tearing (p = 0.002) and less longitudinal tearing (p < 0.001) of muscle fibers, however there was no difference in supraspinatus hole area (p = 0.748). The long head biceps tendon was within 3 mm of the bone entry hole in 13 (28%) shoulders, with one shoulder in the open group exhibiting full tendon transection.
Conclusions:
Percutaneous insertion of intramedullary nails using a cannulated awl appears to produce similar soft tissue and bone entry site morphology as compared to the conventional open technique. The percutaneous method was associated with slightly greater latitudinal tearing, however the effects of this remain to be clarified through clinical studies. External rotation should be avoided during instrumentation to reduce the risk of biceps tendon transection.
Introduction
Proximal humerus fractures are the third most frequent fracture in the elderly, 1 with an increasing incidence due to the aging population. 2,3 While minimally displaced fractures can generally be treated conservatively, displaced and comminuted types run the risk of malunion, nonunion and postoperative stiffness, and may therefore be indicated for surgery. 4 Despite the development of several surgical interventions, including plate fixation, intramedullary nailing, suture fixation, and joint replacement, studies have failed to produce an evidence-based consensus on the optimal treatment method. 5
Intramedullary (IM) nailing is an accepted and widely used fixation method for displaced proximal humerus fractures. Previous second-generation IM nails were curvilinear, requiring a lateral entry that tended to violate the supraspinatus insertion, contributing to postoperative morbidity. 6 Modern third-generation nails are straight or minimally angulated which allows a medial entry that is less likely to violate the supraspinatus tendon. An open approach is generally recommended in the literature 7,8 and in manufacturers’ surgical technique guides in order to visualize, split and repair the rotator cuff fibers. There are, however, several concerns related to this technique. In order to visualize the cuff fibers and humeral head, the surgeon may detach the deltoid origin from the anterior acromion, and the coracoacromial ligament may be partially transected. 7 Both may result in altered biomechanics leading to impaired motion and strength. 9,10 More commonly, the surgeon may dissect the deltoid raphe to visualize the underlying structures. Visualization of cuff fibers, however, can be challenging because they are not readily distinguishable from the subdeltoid bursal layer, and a split in the cuff fibers larger than that required for nail entry is generally necessary to view the underlying articular cartilage. Moreover, it is unknown whether suture repair of the supraspinatus muscle fibers eventually constitutes better healing.
Surgeons have recently begun using a percutaneous technique wherein the nail entry site is prepared using an awl rather than splitting the deltoid, without subsequent repair of the cuff fibers. This minimizes deltoid detachment and eliminates the need to visualize the cuff fibers. Other benefits include a shorter operative duration and reduced bleeding without impacting early rehabilitation. One randomized clinical trial found that straight nails inserted percutaneously led to better function and fewer rotator cuff symptoms than previous-generation curvilinear nails. 6 More recently, a series of 41 patients nailed percutaneously were found to have excellent clinical outcome scores with no morbidity related to penetration of the rotator cuff muscle. 11
Despite encouraging clinical reports, the lack of visualization in the percutaneous technique may be a source of uncertainty that precludes its popularization. Since 2018, our center has routinely performed percutaneous humeral nailing via cannulated awl, however the characteristics of soft tissue damage associated with this technique are not well understood. In this study, we compared the damage caused by entry site preparation and nail insertion between the percutaneous and open techniques in order to substantiate and inform clinical practice. We hypothesized that the percutaneous approach would not result in a significantly different pattern of soft tissue damage as compared to the conventional open approach.
Methods
This study was performed according to the Quality Appraisal for Cadaveric Studies (QuACS) scale. 12 Thirty-one consecutively embalmed whole cadavers were obtained. All cadavers were embalmed with a mixture of 7.5% formalin with ethanol and glycerin. Protocols for cadaver preparation, entry site preparation, nail insertion and outcome assessment were developed in a consensus-building session by performing pilot procedures on two cadavers which were subsequently excluded. Entry site preparation, nail insertion and outcome assessment were performed by six orthopedic surgeons with surgical experience in IM nailing in the last 12 months. One anatomy department lecturer and two orthopaedic residents assisted in soft tissue preparation. Skin, subcutaneous fat, deltoid muscle, subdeltoid bursa and acromioclavicular ligament were removed from the shoulder region without disturbing the underlying rotator cuff muscle and tendon. The anterior compartment muscles of the arm, except for the biceps, were removed to reveal the humeral shaft in order to determine the shaft axis. Cadavers with pre-existing rotator cuff injuries or other shoulder pathologies identified at any point during the study were excluded.
Modern straight antegrade IM nails (MultiLoc humeral nail, DePuy Synthes, Paoli, PA, USA) with a 9.5 mm proximal diameter were used for both percutaneous and open nailing in all shoulders. Each cadaver served as its own control to eliminate confounding effects of anatomical variability. An alternating pseudo-random sequence was used to determine the technique that would be performed on the right and left shoulder. All entry site preparations, nail insertions and observations were performed with cadavers in supine position, shoulder in neutral rotation and 0° abduction. The nail entry site was identified without fluoroscopy by extrapolating the humeral axis by palpation and visualization.
In the conventional open technique, a 1–2 cm longitudinal split was made in the supraspinatus fibers using a scalpel, as per manufacturer recommendations. The cartilage surface was visualized and guide rod with a metal olive was inserted along the humeral shaft axis. A 10 mm hollow reamer was used to create a hole in the humeral head for nail insertion. In the percutaneous technique, a 2.5 mm guide rod was inserted along the humeral shaft axis. A cannulated awl (10 mm diameter) was used to perforate the rotator cuff muscle and simultaneously create a hole in the humeral head for nail insertion without visualizing the cartilage surface. The awl tip was aimed in a posterior position so as to avoid the biceps tendon, which was expected to be located anterior to the guidewire. The hollow reamer was selected for the open technique because it produces a more uniform hole than the awl. Because the hollow reamer cannot be used for the percutaneous technique, the awl was chosen as the next best option that would be used in a pragmatic real-world scenario. A sequential comparison of entry site preparation between the two techniques is displayed in Figure 1.
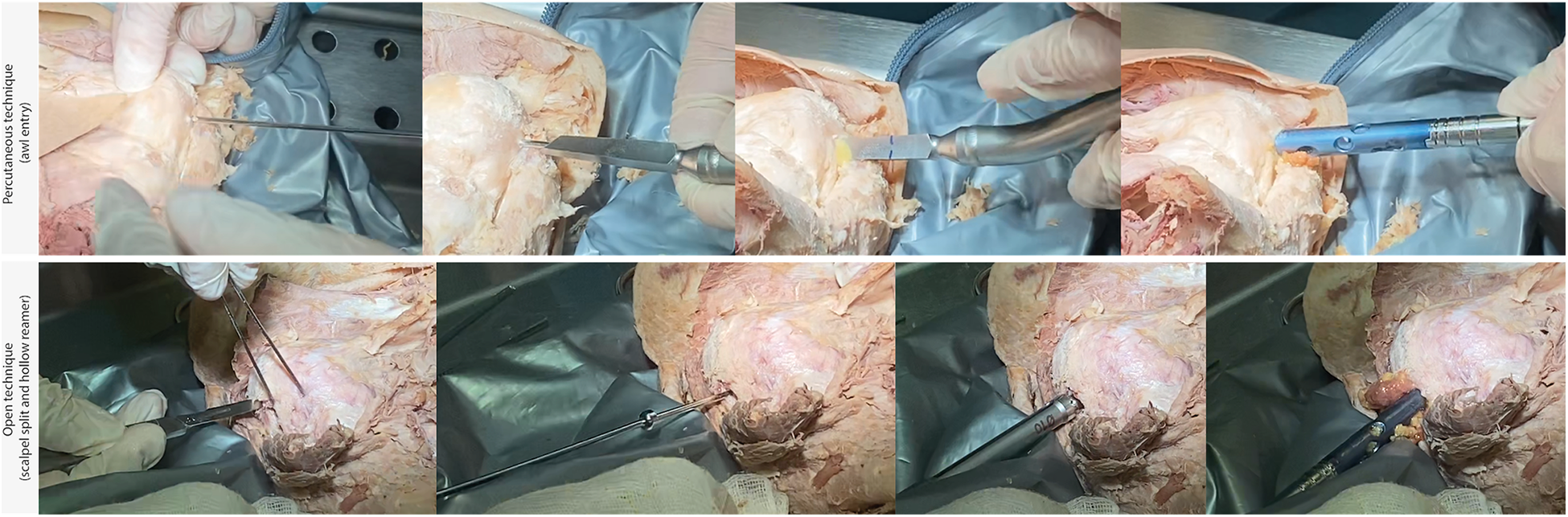
Sequential comparison of entry site preparation in the percutaneous (above) and open (below) techniques.
Outcome parameters
All qualitative and quantitative observations were by consensus between two surgeons who were not told which technique had been performed. With regard to the rotator cuff muscle, longitudinal (along fibers) and latitudinal (across fibers) diameters of the hole produced in the supraspinatus were measured (Figure 2). Assuming an oval configuration, the hole area was calculated as the product of the major radius, minor radius, and π. 13 Qualitative morphology of the hole was recorded (Figure 3). After documentation of rotator cuff status, the supraspinatus was excised to assess the bone entry site characteristics. The shortest distance from the humeral head entry hole to the biceps tendon, and from the bone entry hole to the lateral border of the articular cartilage (Figure 4) were recorded. These measurements were taken because the eccentric nature of the awl was thought to potentially produce slight differences in hole position as compared to the reamer with its centrally placed axis. Qualitative morphology of the humeral head entry hole was also assessed (Figure 5). Using a caliper, the greatest distance from the anterolateral edge of the greater tuberosity to the medial border of the humeral articular cartilage was measured; the mean anatomical neck diameter was measured as the greatest distance between the medial and lateral borders of the articular cartilage (Figure 6).
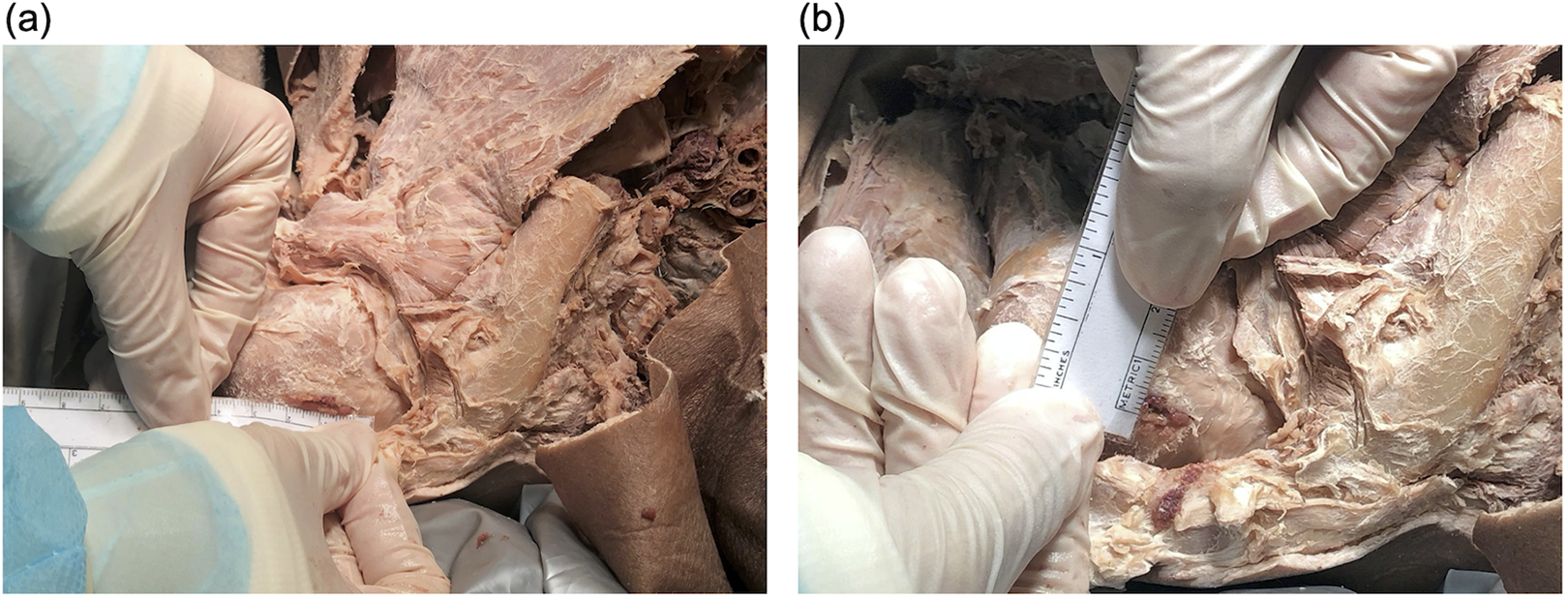
Method for measuring (a) longitudinal and (b) latitudinal diameter of hole in rotator cuff fibers.
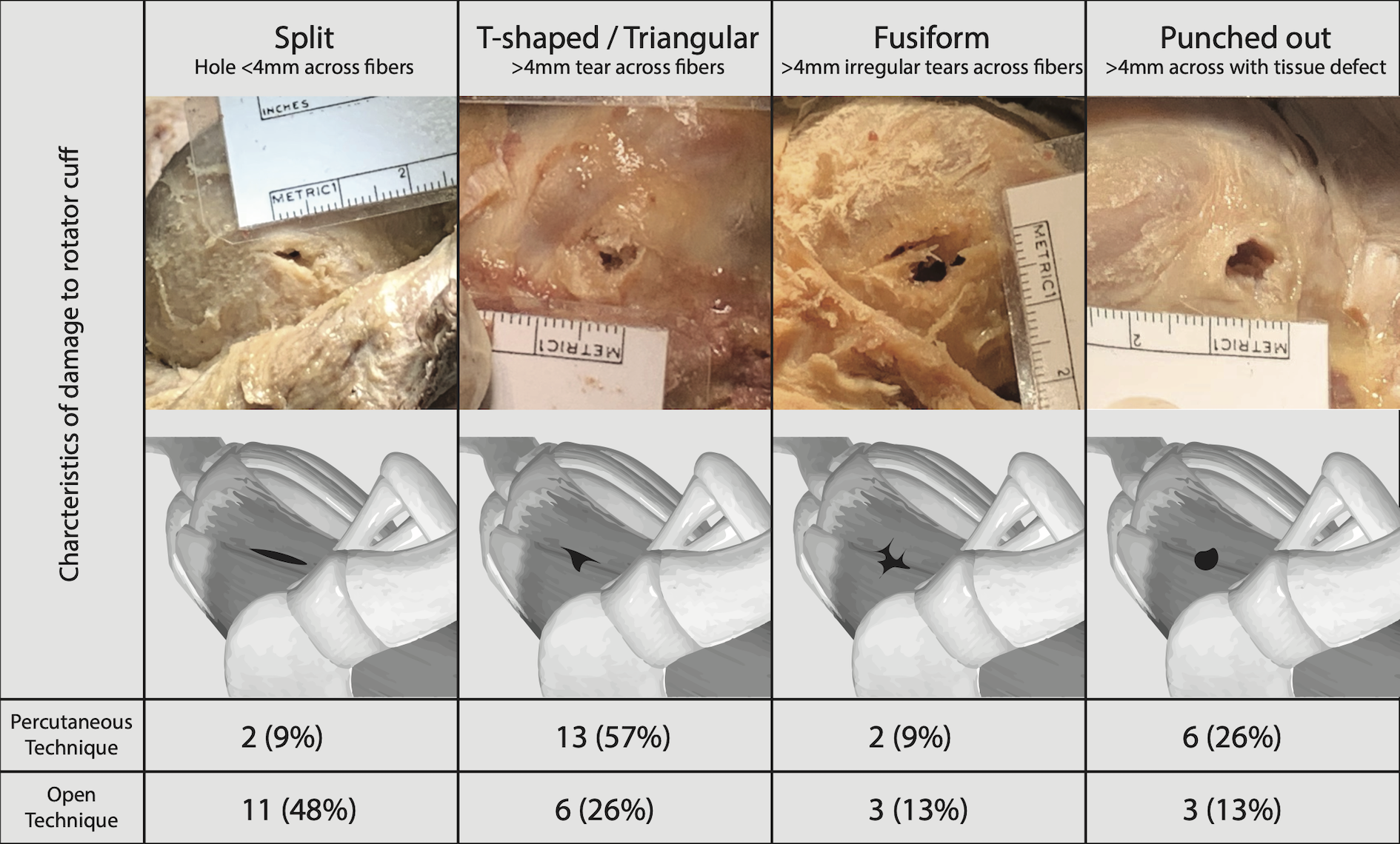
Morphology of damage to rotator cuff fibers by technique. Percutaneous entry was associated with a significantly higher number of triangular, fusiform or punched-out patterns with >4 mm longitudinal tearing (χ2 test, p = 0.018).

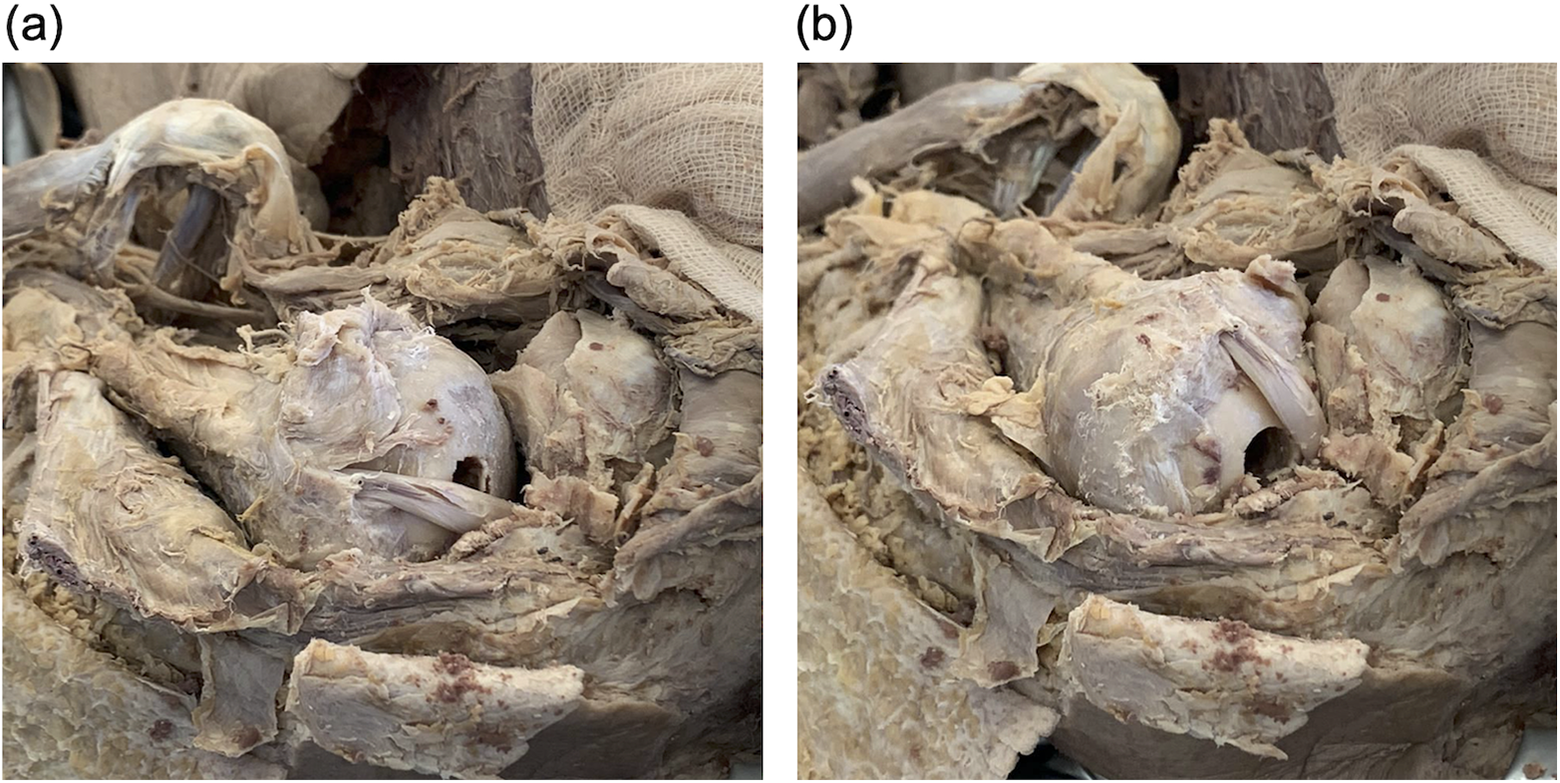
Method for measuring distance (a) from bone entry hole to lateral articular margin and (b) from bone entry hole to long head biceps tendon.

Morphology of humeral head entry hole by technique. Percutaneous entry was associated with significantly more holes with irregular edges (χ2 test p = 0.001).
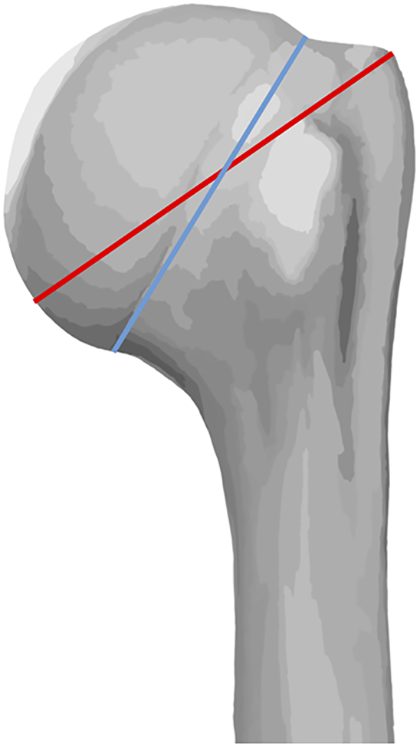
Greatest distance from the anterolateral edge of the greater tuberosity to the medial border of the humeral articular cartilage (red) and anatomical neck diameter (blue).
Statistical analysis
Statistical Package for Social Sciences (SPSS) 26.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Categorical variables were analyzed using χ2 tests. Continuous variables were presented as means with standard deviations and were compared using two-tailed paired t-tests. The type-1 error probability level was set as p < 0.05 throughout.
Results
Subject characteristics
Six cadavers with rotator cuff pathologies in one or both shoulders were excluded. Two cadavers used for pilot procedures to develop study protocols were also excluded. The remaining 23 cadavers (46 shoulders) were included in the study. The sample consisted of 6 female and 17 male cadavers with a mean age of 69.7 (range: 50–87) years at time of death. The mean distance from the anterolateral edge of the greater tuberosity to the medial border of the humeral articular cartilage was 50.7 mm (range: 42–56 mm). The mean anatomical neck diameter was 50.7 mm (range: 42–56 mm) and 45.5 mm (range: 37–61 mm), respectively. The percutaneous technique was performed on 11 right shoulders and 12 left shoulders, with the conventional open technique performed on the corresponding 11 left shoulders and 12 right shoulders.
Soft tissue observations
Quantitative analysis of rotator cuff damage is summarized in Table 1 and compared graphically in Figure 7. The percutaneous technique produced a larger latitudinal hole diameter (5.7 ± 1.8 mm vs 3.4 ± 1.8 mm, p = 0.002) but a smaller longitudinal hole diameter in the supraspinatus muscle fibers (7.5 ± 1.5 mm vs 11.3 ± 2.4 mm, p < 0.001) compared to the open technique. There was no difference in the overall area of the hole (35.0 ± 14.0mm2 vs 33.7 ± 14.7 mm2; percutaneous vs open, respectively; p = 0.748).
Results comparing the soft tissue dimensions of the damage to the rotator cuff and the distances from the bone hole to the biceps tendon and lateral articular edge.
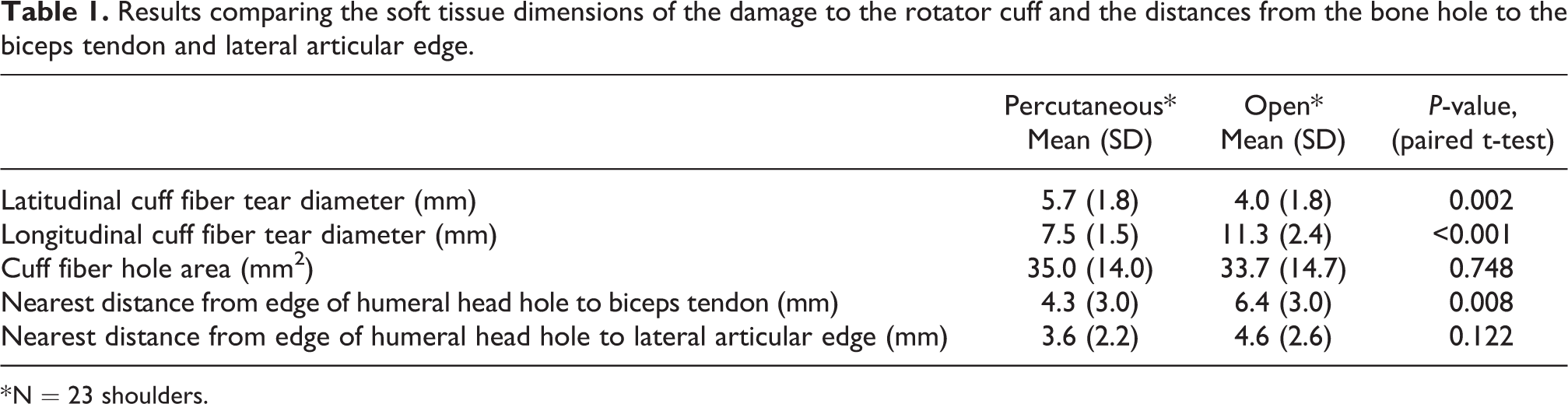
* N = 23 shoulders.

Boxplots showing differences between the percutaneous and open groups. Percutaneous entry resulted in smaller longitudinal tears (a) and larger latitudinal tears (b) in the supraspinatus fibers, with no significant difference in the overall hole area (c).
Qualitative morphology of rotator cuff holes is summarized in Figure 3. Percutaneous entry was associated with <4 mm latitudinal tearing of cuff fibers in only 2 shoulders (9%). The remaining 44 shoulders (91%) were associated with irregular tear patterns (triangular/T-shaped, fusiform, or punched-out) with 4–8 mm of fiber transection. In the open group, 11 shoulders (48%) had a <4 mm latitudinal fiber tearing, with the remaining 12 shoulders (52%) exhibiting irregular tear patterns. The difference in number of shoulders showing split versus irregular tear patterns between the two groups was not statistically significant (χ2 test, p = 0.018). Including all tear morphologies among both groups, no shoulders demonstrated proximal retraction of transected cuff tissue fibers.
Humeral head observations
The shortest distance from the edge of the humeral head entry hole to the biceps tendon was shorter for the percutaneous technique (4.3 ± 3.0 mm vs 6.4 ± 3.0 mm, p = 0.008). Combining both groups, the biceps tendon was within 3 mm of the bone hole in 13 (28%) cadavers and within 6 mm in 27 (59%) cadavers. One shoulder in the open group had a complete biceps tendon laceration caused by entry site preparation. The cadaver was noted to have an anatomical variation with an excessively lateralized bicipital groove and a more posteriorly located long head biceps tendon. The contralateral shoulder displayed the same variation and had a 0 mm distance from the hole to the tendon.
There was no difference between the two techniques with regard to the distance between the edge of the bone hole and the lateral border of the articular cartilage (3.6 ± 2.2 mm vs 4.6 ± 2.6 mm; percutaneous vs open, respectively; p = 0.122). The edge of the hole coincided (0 mm distance) with the lateral border of the articular cartilage in two cadavers (one percutaneous and one open, separate cadavers). No bone entry holes overlapped with the rotator cuff insertion. One humerus in the percutaneous group had iatrogenic shaft fracture related to eccentric (posterior) entry during nail insertion.
Bone hole morphologies of both groups are summarized in Figure 5. Bone hole morphology was related to the entry instrument used; the cannulated awl produced a greater number of irregular hole shapes than the hollow reamer (χ2 test p = 0.001). The hollow reamer produced a near-perfect circle-shaped hole in 20 (87%) shoulders. When using an awl, 14 shoulders (61%) had grossly observable irregularities at the bone hole edge. One shoulder in each group showed osteochondral collapse of the bone hole rim.
Discussion
Antegrade third-generation IM nailing is an accepted alternative to locking plate fixation for two-part proximal humerus fractures. The proposed advantages for nailing, compared to plating, include minimal invasiveness, 6,11 a stiffer mechanical construct 14 and lower complication rates, especially in relation to Intraarticular screw penetration. 15,16 Clinical studies of third generation nails have demonstrated satisfactory outcomes with low rates of cuff-related symptoms. 4,8,11 The success of third-generation nails lends itself to a more medial entry site through the supraspinatus muscle fibers, which are more vascularized and play a less critical mechanical role compared to the avascular tendon insertion. 4 It is traditionally recommended that the rotator cuff be visualized through an open incision, carefully split along its fibers, and repaired by suture. This technique, used with third generation implants, has produced clinical and sonographic evidence of a very low incidence of cuff tears and good healing of the soft tissue portal beyond one year postop. 17 Despite the improvement in entry site location, surgical exposure remains similar between second- and third-generation nailing. The more recent percutaneous technique is an attractive option due to its simplicity, minimal invasiveness, and shortened surgical duration. The primary concern for this technique is the risk of damage to the rotator cuff due to the lack of cuff visualization and repair. Despite this, satisfactory results have been demonstrated in several studies. 6,11,18 This study evaluated the differences in damage to shoulder structures with direct visualization in the open technique versus no visualization in the percutaneous technique.
Our study showed minor differences in hole dimensions and injury pattern to rotator cuff muscle fibers between the two techniques. Awl entry was associated with greater latitudinal transection, but less longitudinal transection. While the difference was small, it may indicate greater muscle damage since more fibers are transected. Impalement by the awl was more likely to result in a punched-out lesion with tissue loss, however conventional scalpel splitting still carried a 52% chance of inadvertent latitudinal tearing of >4 mm due to retraction or subsequent steps. The clinical significance of these differences is uncertain; however, we suspect that any adverse clinical effects would be minimal. Regardless of technique, the muscle tissue surrounding the hole remained intact in all shoulders and appears able to bear the tension caused by entry site preparation and prevent cuff retraction, theoretically facilitating healing of the cuff defect. Additionally, it is possible that the injury pattern caused by the awl could be lessened by optimization of future awl designs; the awl included in our implant kit has a square profile with one spike offset from the center. Our findings confirm that third-generation nails avoid injury to the rotator cuff insertion when the correct entry site is selected 19,20 ; in our study, the edge of the bone hole coincided with the edge of the articular cartilage in only two shoulders.
The relationship between the long head biceps tendon and the nail entry site is of concern due to the risk of injury when a medialized entry site is used. Such is preferred in certain instances of anatomical variation of the neck shaft angle and the proximal humerus offset, 21 or in varus displaced fractures where a medialized entry point could facilitate fracture reduction. We observed the biceps tendon was located within 3 mm of the bone entry hole in 28% of our cadavers and within 6 mm in 59%. Anatomical variations resulting in a lateralized bicipital groove can further predispose the biceps tendon to iatrogenic injury, based on one shoulder in which this occurred. Furthermore, it was noted that during external rotation of the shoulder, the biceps tendon translates posteriorly across the humeral head from the supraglenoid fossa to the bicipital groove, resulting in the biceps tendon overlapping the nail entry site at full external rotation (Figure 8) (Supplementary Material 1). Except for one cadaver with an excessively lateralized bicipital groove, we were able to avoid iatrogenic injury during nail insertion by carrying out the procedure with the shoulder in neutral rotation and forearm resting on the hip. It is therefore important that guide pin and entry point preparation be performed with the proximal bone fragment internally rotated to avoid biceps tendon injury.
(a) The biceps tendon overlaps the nail entry hole when the humeral head is in maximal external rotation, placing it at risk of injury during entry site preparation. (b) When the humeral head is internally rotated, the biceps tendon lies medial and anterior to the nail entry hole.
Our study had several limitations. Firstly, there may have been technical inconsistencies regarding entry site preparation and nail insertion as these were not performed under fluoroscopic guidance. Secondly, the use of embalmed cadavers may have affected the elasticity of soft tissue and hence led to an increased propensity for soft tissue tearing during the procedure. Thirdly, we did not quantitatively record the exact angles of external rotation during which the biceps tendon would override the entry hole in each specimen as this observation was only noted during the end of our dissections and not pre-contemplated in our study protocol. Fourth, while damage to supraspinatus tendon fibers has been identified as a cause of postoperative morbidity, 4 this could not be reliably assessed due to difficulty in visually distinguishing muscular from tendinous fibers.
In conclusion, percutaneous insertion of intramedullary nails appears to produce similar soft tissue and bone entry site morphology as compared to the conventional open technique. The percutaneous method was associated with slightly greater latitudinal tearing, however the effects of this remain to be clarified through clinical studies. When performing the percutaneous technique, the surgeon should be careful to place the proximal bone fragment in neutral or internal rotation to avoid potential injury to the biceps tendon during entry site preparation.
Footnotes
Acknowledgements
The authors wish to acknowledge Patrick Wong, SP Ho, Sally Li and Jeffrey Lau for technical assistance, as well as Grace Ho and Kathine Ching for assistance with data collection.
Author contributions
Study concept: C.F., Fr.L., D.Y., T.M.W.; Manuscript writing: C.F., D.Y., E.F., C.C.C., J.W.; Study protocol development: C.F., T.M.W., T.W.L., G.L.T.; Data analysis: D.Y., C.F., E.F.; Cadaver Procurement: R.L., C.C.C., G.L.T.; Cadaver dissection and implementation: T.P., C.F., Fr.L., T.W.L., R.L., D.Y., T.M.W., J.W., Fe.L.; Data verification: T.M.W., E.F., J.W., Fe.L.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethics approval for this study was waived by the Hong Kong University/Hospital Authority Hong Kong West Cluster Institutional Review Board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.