
Abstract
When sizing the femoral component or determining its placement in total knee arthroplasty (TKA), if the anterior–posterior diameter of the femoral condyle is between component sizes, the selected size will differ depending on whether anterior referencing (AR) or posterior referencing (PR) is used. As a result, the amount of resected bone will also vary. In the present prospective study, we compared the two referencing methods to determine which is more suitable for individual patients. We recruited 58 patients (92 joints) who received TKA using the standard technique with intermediate-size components. AR was used in 26 joints, and PR in 23 joints. Seventeen of the patients underwent same-day bilateral TKA in which components of different sizes were used for the left and right joints. AR resulted in significantly smaller anterior and posterior offsets than PR. Preoperative clinical evaluation revealed no significant differences among cases in which intermediate-size components were indicated, or those in which components of different sizes were indicated. When an intermediate-sized component was indicated using the AR method, moving the sizer forward resulted in a larger posterior gap, but this technique was nevertheless considered acceptable. AR is likely to be more suitable than PR as it achieves more physiological anterior clearance.
Introduction
During total knee arthroplasty (TKA), a sizing guide (sizer) is used to determine the correct size and position of the femoral component. There are two methods for setting the reference position of the sizer: anterior referencing (AR) and posterior referencing (PR).
When the anteroposterior diameter of the femoral condyle matches the anteroposterior diameter of the component (i.e., the sizer indicates the optimum component size), the amount of bone resected will be the same whichever reference method is used. However, when the anteroposterior diameter of the femoral condyle is between component sizes, component size selection and the amount of bone resected will differ depending on the referencing method used. When the size of the component is smaller than the femoral condyle, if AR is selected more bone will be resected and the flexion gap will be wider. In contrast, if PR is selected the risk of causing anterior notch formation is greater. When the size of the component is larger than the femoral condyle, AR will result in a tighter flexion gap, whereas PR will result in a tighter anterior clearance (Figure 1). For this reason, when the sizer indicates an intermediate component size, the surgeon may feel uncertain about whether they should use AR or PR to select the most suitable component.

Issues associated with anterior reference and posterior reference.
This study aimed to examine how differences in the reference position of the sizer and component size affect clinical outcomes and whether AR or PR should be preferred. This prospective, single-blind study was approved by the ethics committee at our institution. Patients were randomly assigned to either AR or PR by the envelope method. Clinical evaluation, plain X-ray evaluation, amount of bone resected, and ligament balance were compared between the two groups. We hypothesized that AR would be more useful, as the amount of posterior bone resection would be greater, resulting in a better flexion angle.
Subjects and methods
Subjects
Subjects were 58 patients (92 joints) who were scheduled to undergo primary TKA using the LEGION CR TKA System between April 2014 and March 2016. Of these, 34 patients underwent bilateral TKA (31 same-day, 3 on different days [staged]) and 24 underwent unilateral TKA. Eight patients were men, 50 were women, all had osteoarthritis (OA) as an underlying disease, and the mean follow-up period was 4 years and 2 months (range: 3 years and 4 months–5 years and 3 months). Mean age at surgery was 76.1 ± 6.4 years, mean body mass index was 25.8 ± 3.9, 11 joints were classified as Kellgren–Lawrence (KL) III and 81 as KL-IV, and 6 joints had patellofemoral (PF) OA.
Operative procedures and postoperative treatment
`The LEGION® cruciate-retaining (CR) TKA system (Smith & Nephew, Memphis, TN, USA) was used in this study. This device is a rebranded version of Genesis II called the Genesis II Symmetric Posterior Condyle. Genesis II has a 5- to 11-year postoperative survivorship of 98.0–98.9%, and good long-term results have been reported. 1,2
All operative procedures were performed under the same conditions. Surgery was performed under general anesthesia via the midvastus approach using an air tourniquet. The distal femoral osteotomy angle was set perpendicular to the functional axis and was determined by individual preoperative planning. The rotational angle of the femoral component was 3° external rotation from the posterior condylar axis. Osteotomy was performed using the measured resection technique. The sizer of the LEGION CR TKA system allows for selection of the referencing method (AR or PR) using just one jig, making it possible to easily change the position of anterior and posterior placement. The femoral component reference was selected by preparing a bag containing envelopes with 47 tags each for AR and PR. Then, on the day before their operation, patients were asked to take an envelope containing a tag from the bag; thus, the selection method was single blinded. However, the femoral component reference was selected prospectively in a random manner between the AR and PR methods. In bilateral cases, AR was used on one side and PR on the other side, to avoid bias, except in one case. The allocation was not sequential.
The procedures for selecting the femoral component size and determining its position were as follows. If the optimum size was indicated by the sizer, that size was selected at the same position with both methods. If an intermediate size was indicated using AR, a smaller component was selected by moving the sizer forward a few millimeters to a position where the smaller size was indicated. Conversely, when using PR, a larger component was selected at the original position (Figure 2). TKA was performed with patellar retention, with no lateral retinacular release. The amount of bone resection was measured using calipers, and the thickness of the resected bone fragment was measured during surgery. To achieve medial and lateral soft tissue balance, the flexion gap was measured using a Monogram Knee Balancer (Stryker-Howmedica, Kalamazoo, MI, USA), which determines the gap and the adduction and abduction angles when distraction force is applied to the mid-joint region. Alternatively, an Ortho Plus knee balancer (Smith & Nephew) was used, which measures the flexion gap on the medial and lateral sides when distraction force is separately applied to the medial and lateral paddles of the device. All cases received the same postoperative treatment, which was initiated on the following day. Patients left their beds and started training to improve the range of motion (ROM) in the knee, and walking training was started 1 week after surgery.
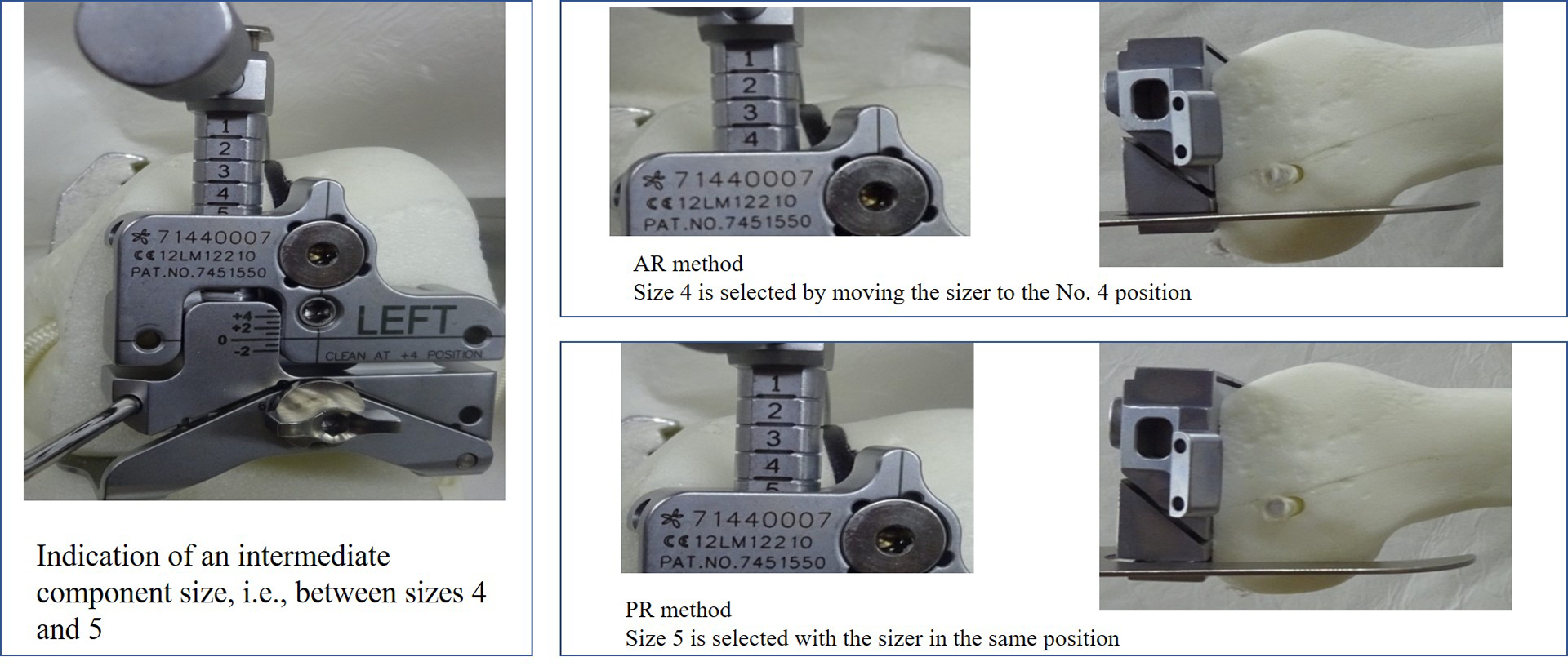
Basic procedures for selecting the size of the femoral component and determining its position with a sizer.
Examined items
In cases in which the sizer indicated an intermediate-sized component and in which surgery was performed using the standard technique, we compared clinical evaluations, plain X-ray evaluations, amount of bone resected, and ligament balance (measured intraoperatively) between the AR and PR methods. In addition, among 30 cases in which surgery was performed using the standard technique for same-day bilateral TKA, we compared those in which components of different sizes were inserted (i.e., a small component according to AR and a large component according to PR) in the left and right joints in a similar fashion according to the AR and PR methods (Figure 3).

Joints included in the study (cases in which intermediate-size components or components of different sizes were used are underlined).
The following items were examined for clinical findings at 4 years and 2 months of mean follow-up: knee ROM, angle improvement (angle at the time of follow-up minus preoperative angle), Knee Society Score (KSS), Knee Society Score–Function (KSSF), and patient’s sense of discomfort due to anterior pain. The following items were examined for postoperative plain X-ray findings at 4 years and 2 months of mean follow-up: component placement angle, standing femorotibial angle (FTA), PF joint gap narrowing, and posterior condylar offset (PCO). PCO was measured in accordance with the method descried by Bellemans et al. 3 using postoperative plain X-ray lateral images. 3 First, a tangential line was drawn at the apex of the posterior condyle of the femur so that it is parallel to a line extended from the posterior cortex of the femur. Next, a vertical line was drawn from the apex of the posterior condyle to a point on the line extended from the posterior part of the femur, and its length was measured. For surgical findings, the amount of bone actually removed and intraoperative soft tissue balance were measured. The thickness of the anterior portion of the LEGION CR femoral component differs by size, whereas the thickness of its posterior portion is fixed at 9.5 mm up to size 6. Anterior offset was calculated by subtracting the amount of anterior bone resection from the anterior thickness of the femoral component, and posterior offset was calculated by subtracting the amount of posterior bone resection from the posterior thickness of the component (Figure 4). A positive offset value indicates a small amount of bone resection, and the presence of anterior or posterior protrusion relative to the original position; a negative offset value indicates a large amount of bone resection, with reduced anterior–posterior overhang relative to the original position.
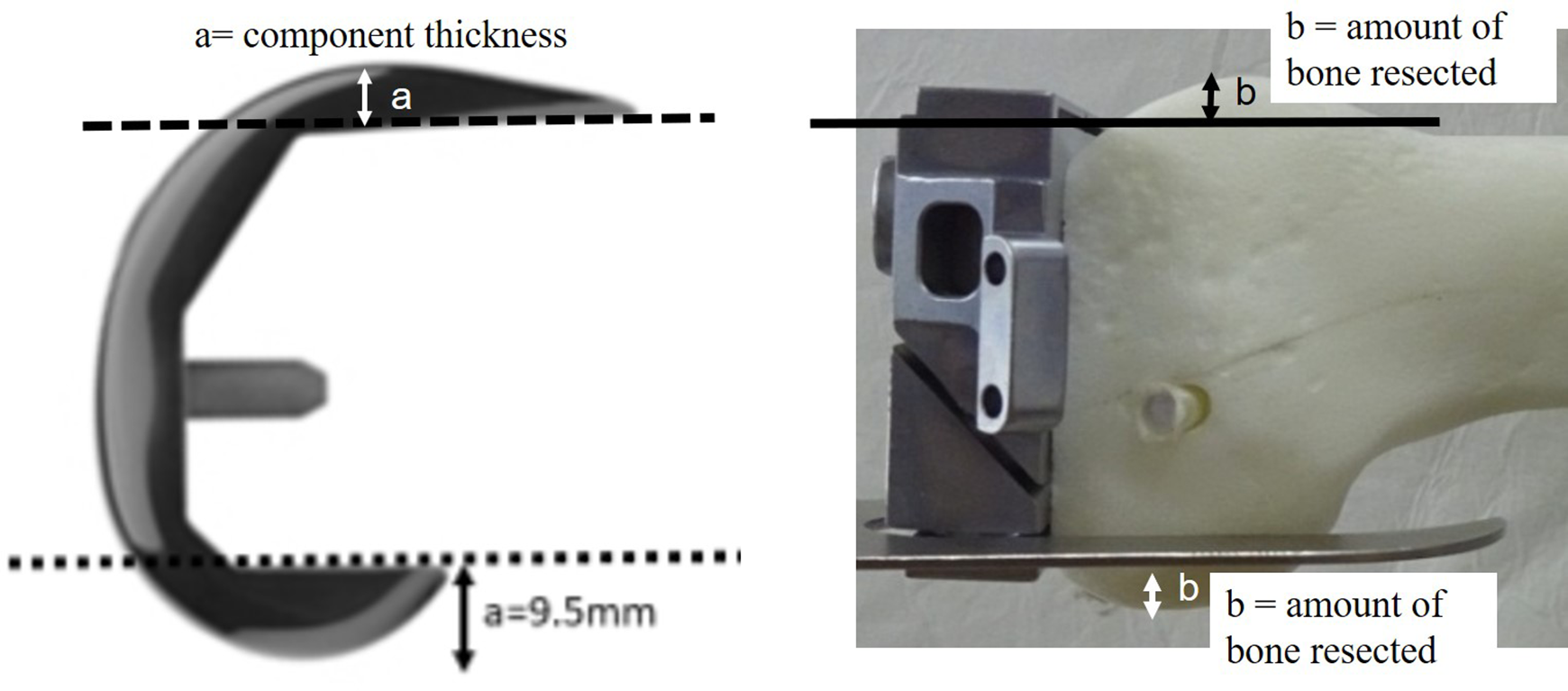
Offset (anterior, posterior) = a-b.
Statistical analysis
SPSS Statistics 26 (IBM Japan, Tokyo, Japan) was used. Differences in measured values between the AR and PR methods were compared using the Mann–Whitney U test. Differences in the number of joints between the AR and PR methods were compared using Fisher’s exact test. P < 0.05 was considered statistically significant. Data are presented as mean ± standard deviation.
Results
Intraoperative findings among the 92 joints included patellar osteophytes in 84 joints, anterior cruciate ligament loss or remnant in 34 joints, a mean insert thickness of 9.7 ± 1.0 mm, and a mean operative time of 86.6 ± 17.8 minutes. AR was used in 47 joints, and PR in 45 joints. Patient characteristics were compared between the two groups, and no significant differences were observed in clinical evaluation, plain X-ray evaluation, or intraoperative findings (Table 1).
Patient characteristics (92 joints).

AR, anterior referencing; PR, posterior referencing; BMI, body mass index; ROM, range of motion; PF, patellofemoral; OA, osteoarthritis; KL, Kellgren–Lawrence; FTA, femorotibial angle.
An intermediate-size component was indicated in 49 cases. AR was used in 26 of these cases (55.3%) and PR in 23 (51.1%) (P = 0.686). Comparisons between the two groups are summarized in Table 2. We compared patient backgrounds, preoperative clinical findings, plain X-ray evaluation findings, and surgical findings between the groups but did not find any significant differences (Table 2). The amount of bone resection was significantly larger on the anterior lateral side (AR: 8.4 ± 2.7 mm, PR: 6.9 ± 1.7 mm) and posterior medial (AR: 13.4 ± 1.0 mm, PR: 11.1 ± 0.7 mm) and lateral (AR: 10.9 ± 1.1 mm, PR: 9.3 ± 0.9 mm) sides of the femur with AR than with PR. No significant difference was observed in ligament balance in extension. Flexion balance showed a significantly wider gap with AR (26.6 ± 2.6 mm) than with PR (24.7 ± 2.7 mm), but only when the Stryker device was used (P = 0.018). No significant differences were observed in the ROM, KSS, or KSSF at the time of follow-up. AR resulted in improved extension angle, and the decrease in flexion angle also tended to be small. Compared with AR, PR tended to result in more discomfort in the anterior part of the knee, with patients experiencing discomfort in four joints after PR compared with one joint after AR. The tibial component placement angle β was 90.7° for AR and 88.9° for PR (P = 0.002), whereas the femoral component angle α (AR: 95.2 ± 1.7°, PR: 94.7 ± 1.6°) and FTA (AR: 174.4 ± 3.8°, PR: 175.4 ± 4.0°) were not significantly different. There was no significant difference in postoperative PF joint gap narrowing. PCO was significantly larger for the PR method (31.2 mm) than the AR method (28.7 mm; P = 0.008). Anterior and posterior offset values were significantly lower on the medial and lateral sides when the AR method was used.
Cases in which total knee arthroplasty was performed using the standard technique when intermediate-size components were indicated.
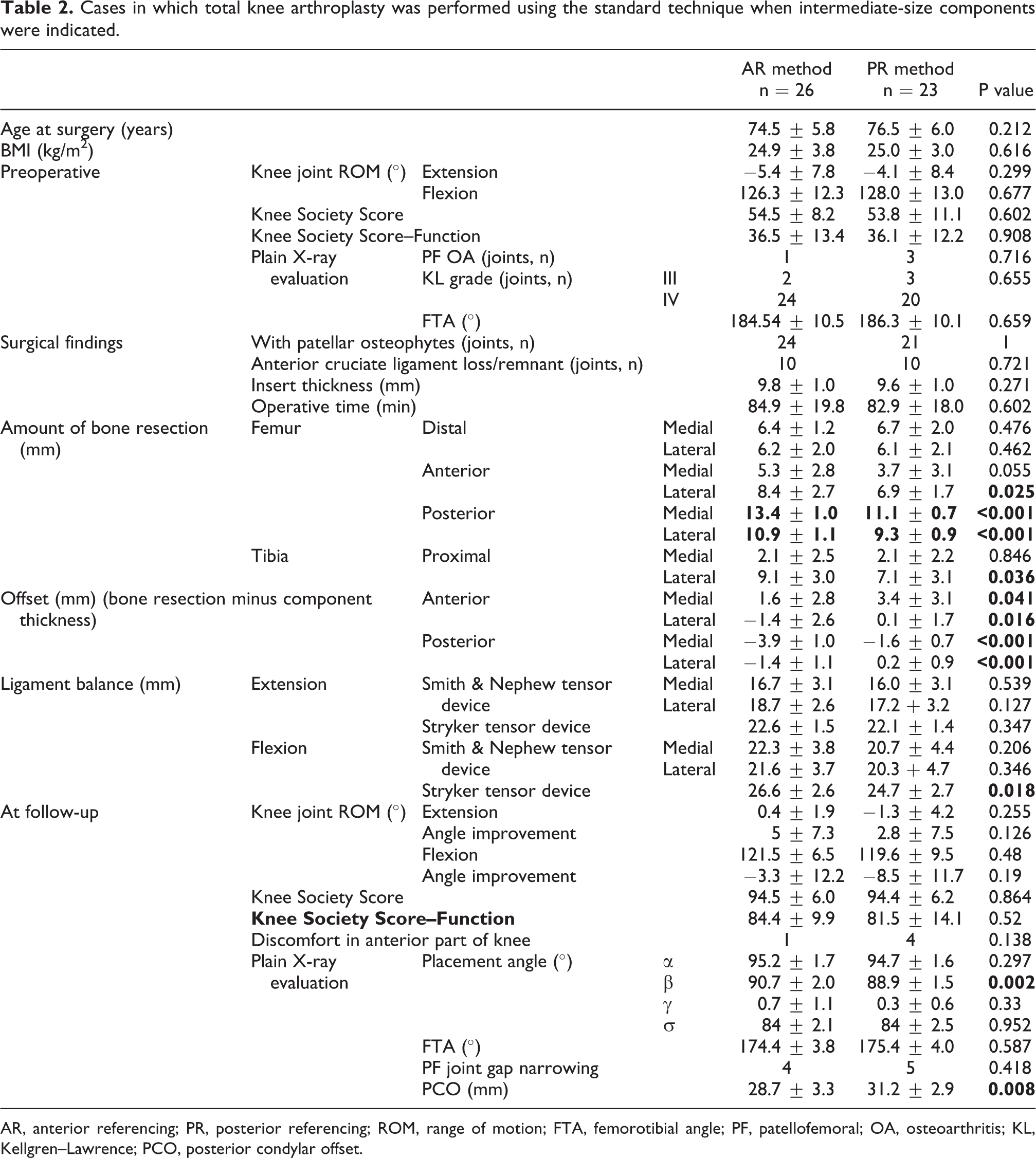
AR, anterior referencing; PR, posterior referencing; ROM, range of motion; FTA, femorotibial angle; PF, patellofemoral; OA, osteoarthritis; KL, Kellgren–Lawrence; PCO, posterior condylar offset.
Comparisons between the AR method with small components and the PR method with large components in the 17 patients who underwent bilateral TKA with femoral components of different sizes are summarized in Table 3. No significant differences were observed in the clinical evaluation. In the plain X-ray evaluation, placement angle β was significantly greater with AR than with PR, but no significant difference was observed in angle α or FTA. The amount of bone resection was significantly larger on the anterior lateral side of the femur as well as the posterior medial and lateral sides of the femur when the AR method was used than when the PR method was used. Anterior and posterior offset values were significantly smaller on the medial and lateral sides with the AR method than the PR method. For ligament balance, the AR method tended to result in a wider gap than the PR method.
Same-day bilateral total knee arthroplasty cases with femoral components of different sizes.

AR, anterior referencing; PR, posterior referencing; FTA, femorotibial angle; PF, patellofemoral; PCO, posterior condylar offset.
Discussion
In TKA, a component that matches the size of the femur must be selected before bone resection to achieve appropriate kinematics. Determining the placement position as well as the size is important. Koninckx et al. reported that with PR, the anterior–posterior width of the femur increased by a mean of 2.3 mm with 3° of external rotation, and by a mean of 3.8 mm with 5° of external rotation, suggesting that an increase in external rotation results in an increase in component size. 4 Furthermore, Minoda et al. reported that the rotation center influences the size of the femur, and when performing CR TKA using PR, referencing centrally or latero-centrally is suitable. 5 In our cases, placement of the CR femoral component was performed with the measured resection method, and sizing was performed at 3° of external rotation from the posterior condyle using a lateral referencing strategy. In general, a small component is selected when the AR method used, so that the flexion gap can be secured by fitting it anteriorly. As this reduces PCO, an excessive flexion gap might result. Conversely, when the PR method is used, the amount of posterior condyle bone resected is small, so PCO is maintained and flexion instability is reduced. However, a large component is selected to avoid anterior notch formation, so the tightness of the anterior clearance becomes a concern.
Regarding anterior clearance, the sizer was moved forward when using the AR method in the present study; this led to reduced anterior notch formation, which was advantageous. While this approach could help reduce the incidence of femoral condyle fractures after TKA in elderly people, there is a concern that PF pressure may increase. Furthermore, excessive resection of the posterior condyle bone 3,6,7 may reduce the posterior offset, risking flexion instability due to an increase in the flexion gap. 3,6 –8 With regard to the relationship between flexion and the femoral component position, Walker and Garg 9 reported that when the CR was replaced anteriorly using computer simulation, the tension of the PCL decreased, causing flexion. Conversely, Mihalko et al. 8 showed that PF tightness might lead to restricted flexion. Examination of our intermediate-size cases revealed a significantly lower anterior offset with AR than with PR, and the anterior movement was not to the extent that PF narrowing could be confirmed in plain X-ray images. These results indicated that selecting a small component using the AR method would likely lead to lower PF pressure than using the PR method. Since the PR method tended to result in more discomfort in the anterior part of the knee, the overhang of the component in the anterior direction when the PR method is used was considered a cause of discomfort.
With respect to posterior clearance, PCO and PCO ratio (PCOR) are important outcome measures of knee joint function 3,10,11 and these values have been reported to increase postoperatively. 12,13 Almeida et al. 13 reported that postoperative PCOR did not differ between the AR and PR methods, showing a significant increase in both cases. For PCO, opinions are divided as to whether it influences ROM 3,6,7,11,14 or not. 10,12,15 –19 Excessive PCO may cause flexion contractures of the knee due to relative shortening of the posterior soft tissue, 14 and the PR method in CR TKA is not an independent risk factor of flexion gap tightness. 20 Since the thickness of the posterior portion of the CR component is fixed, PCO affects the amount of bone resection. In our intermediate-size cases, significantly less posterior bone was resected when the PR method was used, with latero-posterior offset being 0.2 mm greater than when using the AR method. Moreover, when the Stryker device was used, ligament balance in flexion was significantly tighter with PR than with AR, by 1.9 mm. Although the ROM was poorer with AR than with PR before surgery, it tended to be poorer with PR at the time of follow-up. We suspect that the amount of posterior clearance affects the ROM.
To date, only a few reports have compared AR and PR to determine which method is preferable. Fokin et al. 21 compared the two methods in 100 cases of posterior-stabilized (PS) TKA. They found no differences in ROM or clinical results and concluded that both are feasible for minimally invasive TKA. Similarly, Han et al. 12 reported that knee scores and ROM did not differ between AR and PR in 20 cases of bilateral PS TKA, and ROM was not correlated with changes in PCO and postoperative flexion angle. In our cases, flexion angles at the time of follow-up tended to be favorable when the AR method was used, so we conclude that PCO does not affect increases in ROM, and that the technique of moving the sizer forward in the AR method is acceptable.
In the present study, an intermediate-size component was indicated in 17 (56.7%) of 30 cases for one or both knees, even in the same patient or for same-day surgeries, revealing that different referencing methods could lead to the selection of different-sized components for the left and right knees. As a result, anterior and posterior clearances were maintained with the AR method, in which small components are used, in contrast to the PR method. In addition, ROM with AR tended to be better than that with PR. From these results, we conclude that it is better to select the AR method when using the LEGION CR TKA system, and if the sizer indicates an intermediate-size component, it is advisable to select a small component by adopting a method in which the reference position is moved a few millimeters anterior to the position where an intermediate size is indicated.
There are some limitations to this study. First, the sample size was small. Among the 92 joints, the sizer indicated the optimum size in 44.7% of cases in which the AR method was used, and 48.9% of cases in which the PR method was used. Examining only those cases in which an intermediate-size component was indicated resulted in fewer cases, but nevertheless gave us a good indication of the situation. Second, there was a high number of cases in which same-day bilateral TKA was performed. For this reason, no differences in clinical outcomes were observed. Moreover, components of the same size were used for the left and right knees in 14 (45.2%) patients undergoing same-day bilateral TKA, which resulted in fewer cases by extracting those in which components of different sizes were used for the left and right knees. Nonetheless, it was valuable to perform comparisons under the same conditions. Among the 49 joints in which an intermediate-size component was indicated, power analysis was performed using G*Power 3, with an effect size of 0.5 and a significance level α of 0.05; the calculated power was 0.53. A power of 0.41 was calculated for the 34 joints in which components of different sizes were used for the left and right knees. The duration of the follow-up period was also considered a limitation of this study because differences between the two groups might change if patients were followed up for a longer time.
Conclusion
We examined 92 joints in which primary TKA was performed for OA using the LEGION CR system. The AR method was used in 47 joints, and the PR method in 45 joints. The two methods were compared in 26 and 23 joints in which the AR and PR method was used, respectively, and in which an intermediate-size component was indicated, as well as in 17 patients undergoing same-day bilateral TKA with components of different sizes for the left and right knees.
In intermediate-size cases, anterior and posterior offset values and PCO were significantly lower when the AR method was used, and the components were also smaller, although no significant differences were observed in terms of clinical outcomes. Patients tended to report less discomfort with the AR method than with the PR method, and ROM tended to be better with AR than with PR.
We consider the AR method to be the better option as it achieves more physiological anterior clearance.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Clinical Research (Public Notice of the Ministry of Health, Labour and Welfare No. 415 of 2008), and was approved by the ethics committee of our hospital.