
Abstract
Purpose:
Shorter length of stay (LOS) after total knee arthroplasty (TKA) is cost-effective. Straight leg raise (SLR) is a common exercise prescribed after TKA, but the significance of early postoperative SLR is unknown. The primary aim of this study is to evaluate the association between early postoperative SLR and LOS. Secondary aims are to explore associations among early postoperative SLR, time to ambulation, and time to stairs climbing and identify factors related to postoperative SLR.
Methods:
888 TKAs (888 knees, 865 patients) performed at a tertiary hospital in 2016 were included for this retrospective study. All TKAs were performed with medial parapatellar approach and tourniquet. Time to events (SLR, ambulation, stair climbing), LOS and factors influencing these events were analysed using a multivariate Poisson regression model and logistic regression.
Results:
Patients who performed SLR on postoperative day 1 (POD1) had shorter LOS than those who did not (adjusted Mean Ratio (aMR) = 0.846, p < 0.001), with estimated mean LOS being 3.5 days and 4.1 days, respectively. Performing SLR on POD1 was also associated with shorter time to ambulation (aMR = 0.789; p < 0.001) and stair climbing (aMR = 0.811, p < 0.001). Female gender and higher rest pain on POD1 were associated with delayed postoperative SLR.
Conclusion:
Performing SLR on POD1 after TKA is associated with shorter LOS, time to ambulation, and time to stair climbing. Early postoperative SLR can prognosticate early recovery and discharge. Optimization of preoperative muscle strength and postoperative pain may be important in early recovery after TKA.
Introduction
Total Knee Arthroplasty (TKA) is a successful procedure for severe osteoarthritis. 3.48 million TKAs per annum are projected by the year 2030 in the United States alone. 1 TKAs are associated with high cost, and a significant amount of the cost is from the hospital stay. 2 Shorter length of stay (LOS) after TKA has been shown to reduce cost without increasing readmission rates. 3,4 This has led to surgeons adopting strategies to reduce LOS after TKA and a trend towards enhanced recovery after surgery (ERAS), day surgery, and outpatient surgery. LOS is a multifactorial parameter influenced by patient, surgical, social, and rehabilitation factors. Several factors associated with LOS after TKA are age, race, discharge to other facilities, medical complications, 5 premorbid functional status, 6 and day of operation. 7 Postoperative physiotherapy is another important determinant of LOS and functional outcomes. Postoperative physiotherapy consists of ambulation, range of motion (ROM), and muscle strengthening. Early ambulation with physiotherapy has been studied to reduce LOS, and postoperative assessment of ROM and muscle strength are crucial for functional outcome. 8,9
Higher postoperative ROM is associated with better patient-reported outcomes 10,11 and patient satisfaction after TKA. 12 Quadriceps muscle strength after TKA is correlated with functional outcomes, including performance in Timed Up and Go and Stair Climbing Test. 13 Patients who undergo TKA have significant loss of quadriceps muscle strength 14 and deficient voluntary activations of the muscle. 15,16 Postoperative muscle strength after TKA, however, is not routinely measured during an inpatient stay. Straight leg raise (SLR) and leg extension are surrogates for quadriceps muscle strength since quadriceps muscle activation, especially rectus femoris, is involved in both actions. 17 SLR is commonly prescribed by physiotherapists and surgeons after TKA, but little is known about the significance of early postoperative SLR. Early postoperative SLR likely indicates good preoperative quadriceps strength, satisfactory arthrotomy repair technique and optimal postoperative pain control.
The primary aim of this study is to evaluate the association between early postoperative SLR and LOS. Secondary aims are to explore associations among early postoperative SLR, time to ambulation, and time to stairs climbing and identify factors affecting postoperative SLR. Understanding the relationship between early postoperative SLR and inpatient outcomes may guide future pre and postoperative management. Our hypothesis is that early postoperative SLR after TKA is associated with shorter LOS, time to ambulation, and time to stair climbing. We hypothesize premorbid function based on questionnaires are associated with early postoperative SLR.
Materials and methods
Subjects
The study was approved by our Institution’s Centralized Institutional Review Board (CIRB 2018/3027). This retrospective study examined 888 primary, unilateral TKAs (865 patients) performed at a Singapore tertiary hospital in 2016. All TKAs were performed through medial parapatellar approach with tourniquet, and patients did not receive femoral nerve block or epidural infusion. Only patients who achieved SLR, ambulation, and stair climbing with known dates were included in the study. Patients with planned or actual discharge to community hospital and severe medical complications, namely myocardial infarction, cerebrovascular accidents, or asystole were excluded. Patients were given similar multi-modular postoperative pain control with periarticular injection (morphine, Marcaine, ketorolac) and oral analgesia (paracetamol, etoricoxib/tramadol, gabapentin).
Study design
Daily inpatient physiotherapy was offered to TKA patients from postoperative day 1 (POD1). Physiotherapy sessions included pain assessment (verbal numerical scale from 0 to 10), passive ROM assessment, SLR, trial of ambulation, and trial of stair climbing. To assess SLR, patients were asked to lift the operated leg off the bed without bending the knee and hold the position for 10 seconds. SLR attempts were recorded in electronic medical record system as 1) whether the patient was able to raise the operated leg 2) the number of seconds the patient was able to hold in air 3) the number of repetitions performed. For the purpose of this study and to minimize any variability in assessment by physiotherapists, SLR was considered successful if the patient was able to independently lift the operated leg off the bed, regardless of height raised, presence of knee flexion, or hold time. Early postoperative SLR was defined as ability to perform SLR on POD 1 (POD1 SLR). The number of days from operation to first SLR was recorded as time to SLR.
Ambulation was defined as taking any forward step with any ambulation aid and type of assistance from physiotherapists. The use of appropriate aid and assistance was selected by physiotherapists based on the patient’s gait and safety profile. Possible ambulation aid included no aid, walking stick, crutches, narrow-based quad stick, broad-based quad stick, walking frame, and rollator frame. Sit to stand, transfer, and marching on spot were not considered as ambulation. As a routine practice in the tertiary hospital, stair climbing was attempted from POD2, with the exception of a few patients who climbed stairs on POD1. Time to first ambulation and time to first stair climbing were recorded as number of days. All patients were required to ambulate and climb stairs prior to discharge. LOS, the primary outcome, was defined as the number of days from the operation day to discharge.
Other factors collected that may influence LOS were age, gender, BMI, premorbid ambulation aid, presence of home care, operation day, inpatient complications, rest pain on POD1, and ASA score. For premorbid ambulation aid, patients were stratified based on the support provided by ambulation devices and categorized into three groups: no aid, walking stick, crutches/quad sticks/frames. Pain was measured before each physiotherapy session using verbal numerical score ranging from 0 to 10. Preoperative ROM and questionnaires (Oxford Knee Score, Knee Society Score, and 36-Item Short Form Survey) were identified as potential factors associated with early postoperative SLR performance along with patient demographics. All data were collected through one centralized electronic medical records system.
Statistical analysis
Data were analysed using SPSS version 22. A multivariable Poisson model was applied to examine each of the three continuous outcomes: LOS, time to ambulation, and time to stair climbing. These outcome variables had skewed distributions. Nonparametric univariate analysis for the outcomes, treated as continuous variables, was conducted for each independent variable using Mann-Whitney U test (2 categories), Kruskal-Wallis test (>2 categories), and Spearman’s correlation coefficient (continuous variable). Independent variables with p < .20 in univariate analyses were included in the multivariable Poisson analysis. Independent variables were adjusted for in the Poisson models. The level of significance was determined as p < .05 for Poisson models.
A binary logistic regression was used to explore factors associated with early postoperative SLR. Univariate analysis was conducted for categorical variables (chi-squared test) and continuous variables (independent T tests). Independent variables with p < .20 in univariate analyses were included in the logistic regression. For binary logistic regression, the level of significance was determined as p < .05. There was a total of 15 missing data (<2%) in pain score and BMI. These values were imputed with mean imputation to avoid case-wise deletion of records with missing covariates.
Results
Majority of the study population (67.1%) was able to perform SLR on POD1 (Table 1). Spinal regional anaesthesia was more common choice of anaesthesia compared to general anaesthesia (64.2% vs 35.8%). More males (206/267 = 77.2%) were able to perform SLR on POD1 than females (389/612 = 63.6%). The average rest pain on POD1 for patients who performed SLR on POD1 was 1.0 lower than those who did not (1.2 vs 2.2). Gender and rest pain on POD1 were significantly associated with POD1 SLR. Gender had an odds ratio (OR) of 1.922 (95% CI 1.337, 2.763), with females 1.9 times the odds of inability to perform SLR on POD1 relative to males (Table 2). Higher levels of pain on POD1 were associated with greater odds of inability to perform SLR on POD1 (OR: 1.35, 95% CI 1.24, 1.46).
Demographics and univariate analyses for straight leg raise.
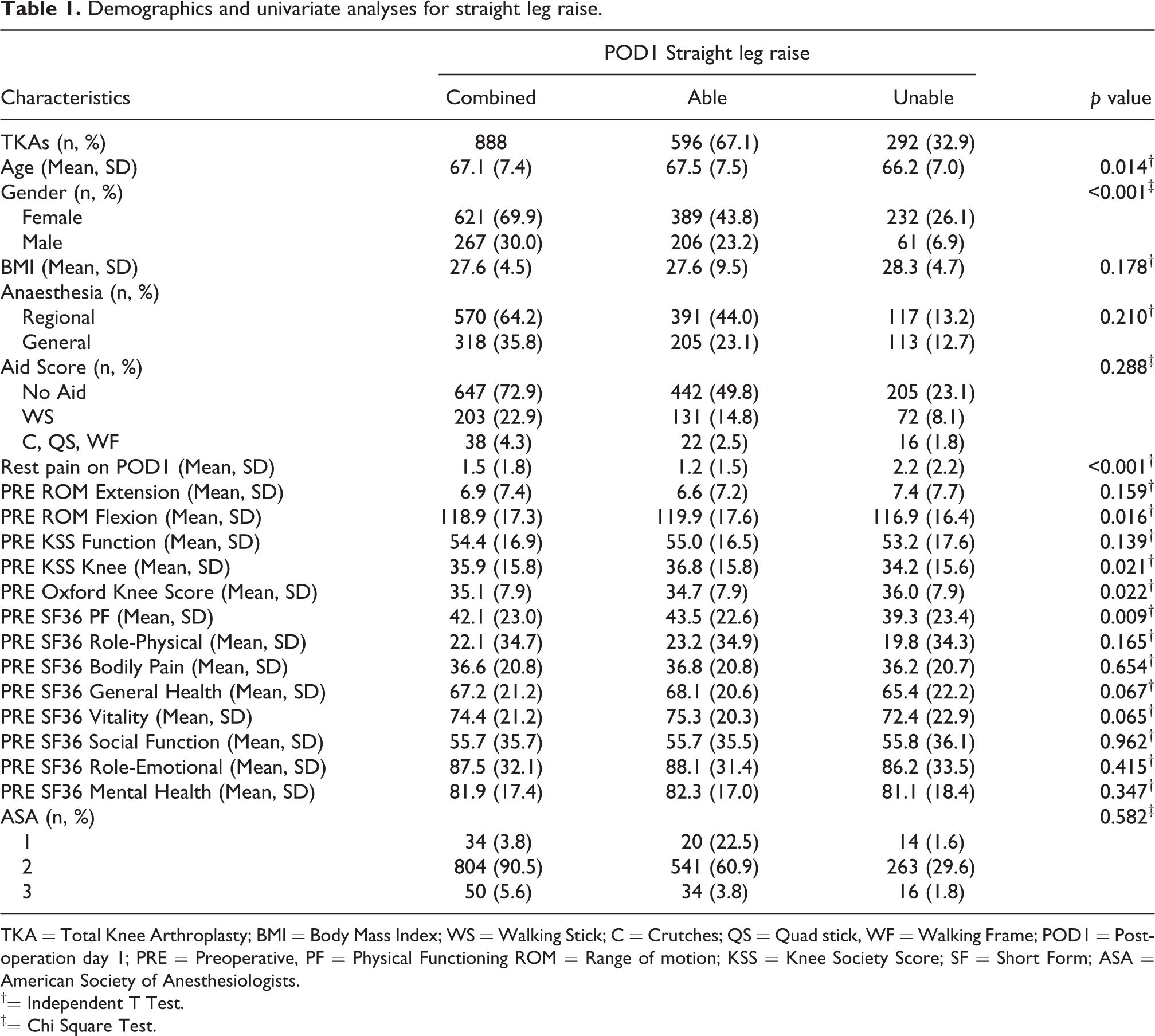
TKA = Total Knee Arthroplasty; BMI = Body Mass Index; WS = Walking Stick; C = Crutches; QS = Quad stick, WF = Walking Frame; POD1 = Post-operation day 1; PRE = Preoperative, PF = Physical Functioning ROM = Range of motion; KSS = Knee Society Score; SF = Short Form; ASA = American Society of Anesthesiologists.
†= Independent T Test.
‡= Chi Square Test.
Logistic regression for straight leg raise.

TKA = Total Knee Arthroplasty; BMI = Body Mass Index; POD1 = Post-operation day 1; PRE = Preoperative ROM = Range of motion; SF = Short Form; PF = Physical Functioning; CI = Confidence interval.
*p < 0.05.
The mean LOS for the study population was 3.7 ± 1.5 days (Table 3). The presence of inpatient complications (adjusted Mean Ratio [aMR]: 1.373, p < .001) and rest pain on POD1 (aMR 1.032, p = .001) were significantly associated with prolonged LOS (Table 4). POD1 SLR was associated with a shorter LOS (aMR 0.846, p < .001). The estimated mean LOS from the Poisson model for patients who performed SLR on POD1 and patients who could not were 3.5 days (95% CI 3.2, 3.8) and 4.1 days (95% CI 3.8, 4.5), respectively (Figure 1). The difference in mean LOS between the two groups was 0.6 days.

This figure shows the estimated mean length of stay (LOS) for postoperative day 1 (POD1) straight leg raise (SLR) from the Poisson model, after accounting for other factors. 95% Confidence Interval for POD1 Able (3.3, 3.8) and POD1 Unable (3.8, 4.4).
Demographics and univariate analyses for length of stay.

TKA = Total Knee Arthroplasty; LOS = Length of Stay; BMI = Body Mass Index; WS = Walking Stick; C = Crutches; QS = Quad stick, WF = Walking Frame; POD1 = Post-operation day 1; SLR = Straight Leg Raise; ASA = American Society of Anesthesiologists.
†Spearman’s Correlation Coefficient.
‡Mann-Whitney U Test.
§Kruskal-Wallis Test.
Multivariable Poisson regression analysis for length of stay.

REF = Reference, WS = Walking Stick; C = Crutches; QS = Quad stick, WF = Walking Frame; BMI = Body Mass Index; POD1 = Post-operation day 1; SLR = Straight Leg Raise; aMR = adjusted Mean Ratio.
*p < 0.05.
The mean time to ambulation was 1.2 ± 0.5 days with 82.3% of the study population ambulating on POD1 (Table 5). Complications and POD1 SLR were significant factors associated with time to ambulation (Table 6). The aMRs for complication and POD1 SLR were 1.217 (p = .021) and 0.789 (p < .001), respectively. There was a decrease in estimated mean time to ambulation from 1.5 days (95% CI 1.3, 1.7) to 1.2 days (95% CI 1.0, 1.3) for those who perform SLR on POD1 (Figure 2). An increasing trend of time to ambulation was seen after time to SLR was associated with the time that first SLR was performed (POD1, POD2, POD3, POD4, POD5 and above) (Figure 3).

This figure shows the estimated mean time to ambulation for postoperative day 1 (POD1) straight leg raise (SLR) from the Poisson model, after accounting for other factors. 95% Confidence interval for POD1 Able (1.0, 1.3) and POD1 Unable (1.3, 1.7).

This figure shows the estimated time to ambulation for time to straight leg raise (SLR) variable (categorized into postoperative day 1, 2, 3, 4, 5 and above) from the Poisson model, after accounting for other factors.
Demographics and univariate analyses for time to ambulation.

TKA = Total Knee Arthroplasty; BMI = Body Mass Index; WS = Walking Stick; C = Crutches; QS = Quad stick, WF = Walking Frame; POD = 1 Post-operation day 1; SLR = Straight Leg Raise; ASA = American Society of Anesthesiologists.
†Spearman’s Correlation Coefficient.
‡Mann-Whitney U Test.
§Kruskal-Wallis Test.
Multivariable Poisson regression analysis for time to ambulation.

REF = Reference, WS = Walking Stick; C = Crutches; QS = Quad stick, WF = Walking Frame; BMI = Body Mass Index; POD1 = Post-operation day 1; SLR = Straight Leg Raise; aMR = adjusted Mean Ratio.
*p < 0.05.
The mean time to stair climbing was 2.5 ± 1.0 days (Table 7). Inpatient complications (aMR = 1.380, p < .001) and POD1 SLR (aMR = 0.811, p < .001) were associated with time to stair climbing (Table 8). The estimated mean time to stairs climbing for patients who can perform SLR on POD1 and who cannot perform SLR on POD1 were 2.3 days (95% CI 2.2, 2.6) and 2.9 days (95% CI 2.6, 3.2) (Figure 4). An increasing trend of time to stairs climbing was associated with the time that first SLR was performed (POD1, POD2, POD3, POD4, POD5 and above) (Figure 5).

This figure shows the estimated mean time to stair climbing for postoperative day 1 (POD1) straight leg raise (SLR) from the Poisson model, after accounting for other factors. 95% Confidence interval for POD1 Able (2.2, 2.6) and POD1 Unable (2.6, 3.2).

This figure shows the estimated time to stair climbing for time to straight leg raise (SLR) variable (categorized into postoperative day 1, 2, 3, 4, 5 and above) from the Poisson model, after accounting for other factors.
Demographics and univariate analyses for time to stair climbing.

TKA = Total Knee Arthroplasty; BMI = Body Mass Index; WS = Walking Stick; C = Crutches; QS = Quad stick, WF = Walking Frame; POD1 = Post-operation day 1; SLR = Straight Leg Raise; ASA = American Society of Anesthesiologists.
†Spearman’s Correlation Coefficient.
‡Mann-Whitney U Test.
§Kruskal-Wallis Test.
Multivariable Poisson regression analysis for time to stair climbing.

REF = Reference, WS = Walking Stick; C = Crutches; QS = Quad stick, WF = Walking Frame; BMI = Body Mass Index; POD1 = Post-operation day 1; SLR = Straight Leg Raise; aMR = adjusted Mean Ratio.
*p < 0.05.
Discussion
The most important finding from this study is that POD1 SLR is associated with LOS, time to ambulation, and time to stair climbing. Patients who perform SLR on POD1 have 15% shorter estimated mean LOS, which is equivalent to 0.6 days as estimated mean difference. POD1 SLR is associated with faster time to ambulation and time to stair climbing. To our knowledge, no other study has looked at association between early postoperative SLR and LOS after TKA. Our study’s findings, however, differ from a cross-sectional study by Ishii et al. which found no significant correlation between time to SLR and time to ambulation. 18 This could be due to population differences in terms of ethnicity and body mass index. Early mobilization after TKA has been established to influence LOS and it could indicate better functional recovery, as patients with early mobilization were more likely to be discharged to home compared to sub-acute rehabilitation facility. 19,20 The association between early postoperative SLR and LOS may therefore be secondary to the patient’s ability to ambulate early. Patients who are unable to perform SLR on POD1 may benefit from additional physiotherapy and optimization of postoperative pain to facilitate earlier recovery. On the other hand, patients who perform SLR on POD1 may be selected for ERAS and early discharge.
The ability to perform postoperative SLR is determined by muscle strength, pain, and motivation. Patients who achieved SLR on POD1 were likely to possess better postoperative muscle strength. Postoperative quadriceps strength is known to be influenced by preoperative strength and type of surgical procedure. For example, subvastus approach is associated with shorter time to SLR than the conventional medial parapatellar approach. 21,22 Quadriceps strength and volume have been known to decrease after the use of tourniquet during TKA. 23,24 Higher postoperative knee swelling after TKA is correlated with decreased quadriceps strength. 25 Given that all TKA procedures are performed in a homogenous fashion at our institution, preoperative quadriceps strength may have predicted early postoperative SLR. Future studies can consider studying preoperative quadriceps strength as a predictor of early postoperative SLR and selection criteria for ERAS.
Postoperative pain is an integral part of management after TKA. Pain is a subjective measure, but it can affect recovery and postoperative mobilization, particularly during the first postoperative day. 26 In our study, higher rest pain on POD1 was associated with increased LOS and delayed SLR. SLR performance and other physiotherapy exercises can be influenced by significant pain. Severe postoperative pain has been studied to cause delayed discharge after hip and knee arthroplasty. 27 The mechanism may be due to delayed recovery leading to prolonged LOS. In addition to pain, gender is identified to be associated with SLR performance on POD1. The significance of gender in TKA has been controversial. There is no reported difference in outcomes between males and females after TKA in Asian population. 28 However, males report less pain compared to females in both pre and post-operation. 29,30 In our study, males report lower pain on POD1 compared to females and are more likely to perform SLR on POD1. The difference in pain between the genders may be linked to SLR performance.
Inpatient complications are associated with longer LOS. El Bitar et al. demonstrated all types of inpatient complications were associated with longer LOS. 5 Even with good functional recovery of the operated knee, some patients extend their inpatient stay for medication titration and treatment for surgical and medical complications. Complications are also associated with a longer time to ambulation and stair climbing. Some complications prevent certain activities or even entire physiotherapy sessions due to patients’ symptoms or impending investigations. For example, patients who require blood transfusions miss physiotherapy sessions for that day. Inpatient complications are not categorized in our study for simplicity.
The limitation of this study is its retrospective data collection and interpretation. Social and personal factors, which can have a significant impact on LOS, are not fully accounted for in this study. Presence of carer at home is included to account for social factors that may affect hospital LOS. However, LOS is also affected by other social factors and personal factors that cannot be easily accounted for. This may include inadequate home environment, transportation for discharge, and personal choice. These factors are not easily quantifiable, especially in a retrospective study. Another limitation is regarding ambulation. Our study defines ambulation as any forward steps taken with any ambulation aid and assistance. The number of steps, ambulation aid, and ambulation assistance from physiotherapist are not considered in this study. The average time to ambulation for the study population is 1.2 days and most patients ambulate on POD1. This classification based on our definition of ambulation may not represent the variability of physical functions in the study population. With a validated ordinal scale stratifying patient based on ambulation aid and assistance, we may be able to better understand the relationship between SLR and ambulation.
Conclusion
Performing SLR on POD1 after TKA is associated with shorter LOS, time to ambulation, and time to stair climbing. Postoperative pain is closely related to postoperative SLR performance and LOS after TKA, highlighting the importance of postoperative pain control. Early postoperative SLR can be used to prognosticate patient’s inpatient recovery after unilateral TKA. Measuring and optimizing preoperative quadriceps strength and postoperative pain may be useful to identify suitable ERAS patients and could aid in achieving early postoperative SLR and reduction in LOS.
Footnotes
Acknowledgements
We would like to acknowledge Singapore General Hospital Orthopaedic Diagnostic Centre for safe data storage and transfer.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by SingHealth Duke-National University of Singapore Nurturing Clinician Scientist Scheme [13/FY2017/P1/16-A30].