
Abstract
Purpose:
To investigate the risk factors for hip displacement in patients with dyskinetic cerebral palsy (DCP).
Methods:
We evaluated 81 patients with DCP, 45 males and 36 females, aged 10–22 years, risk factors for hip displacement were evaluated using multivariate logistic regression analysis with primary brain lesions, Gross Motor Function Classification System (GMFCS) level, gestational age, birth weight, Cobb’s angle, and complication of epilepsy as independent factors. Hip displacement was defined as migration percentage >30%. Primary brain lesions were classified into globus pallidus (GP), thalamus and putamen (TP), and others using brain magnetic resonance imaging (MRI). Perinatal and clinical features were compared between patients with GP lesions and those with TP lesions.
Results:
Hip displacement was observed in 53 patients (67%). Higher GMFCS levels (p = 0.013, odds ratio [OR] 2.6) and the presence of GP lesions (p = 0.04, OR 16.5) were independent risk factors for hip displacement. Patients with GP lesions showed significantly higher GMFCS levels, more frequent hip displacement, and lower gestational age and birth weight than those with TP lesions.
Conclusion:
Primary brain lesion location may be an important factor in predicting hip displacement among patients with DCP. Appropriate risk assessment using brain MRI may contribute to the early detection and intervention of hip displacement because brain lesion location can be assessed during infancy before GMFCS level is decided.
Introduction
Cerebral palsy (CP) encompasses several permanent movement disorders caused by non-progressive disturbances in the developing fetal or infant brain 1 and is clinically characterized by abnormal posture and insufficient muscle tone regulation. There are four major types of CP: spastic (76–80% of cases), dyskinetic (2–14% of cases), ataxic (<2% of cases), and mixed type (<2% of cases). 2,3 The dyskinetic types are mostly caused by lesions in the bilateral deep grey matter, such as the thalamus and putamen (TP) and globus pallidus (GP). 4,5
The prevalence of hip dislocation was reported to be 15–35% in patients with CP of all types 6 –9 and 10–48% in those with dyskinetic cerebral palsy (DCP). 10,11 Hip displacement or dislocation often results in the destruction of the hip joint cartilage, causing pain in the hip and limitations in range of motion. 12 Subsequently, patients are unable to sit or receive sufficient care, 13 and the quality of life (QOL) of both patients and caregivers declines. 4,6 Hence, early diagnosis and treatment of hip displacement are important for the prevention of future QOL deterioration.
It is difficult to predict hip dislocation in patients with DCP as compared to those with spastic CP 14 because the posture and laterality of patients with DCP are not always fixed, and their muscle tone fluctuates with changes in mood and/or circumstances. There are many reports regarding the risk factors for hip dislocation in patients with spastic CP, but only a few reports exist on the risk factors for hip dislocation or displacement in patients with DCP. The purpose of this study was to investigate the risk factors for hip displacement among patients with DCP with reference to the location of their brain lesions.
Materials and methods
Patients
We recruited patients with DCP who visited the rehabilitation/orthopedic clinic of our institution between April 2006 and December 2019. All patients were diagnosed by a pediatric neurologist based on the Surveillance of Cerebral Palsy in Europe. 15 The inclusion criteria were as follows: over 2 years of follow-up, age ≥10 years at the latest follow-up, and complete clinical information including hip and spine radiographs and brain magnetic resonance imaging (MRI). All patients received physical therapy, and orthoses were prepared and adjusted to encourage hip abduction with use of orthoses in the patients. X-rays were assessed annually, and patients who received surgical treatment, including soft tissue release or osteotomies, were excluded from the study when the operation was performed.
Methods
Migration percentage (MP) for the hip joint and Cobb’s angle for scoliosis were measured using plain antero-posterior radiographs at the latest follow-up. Hips with an MP > 30% were considered as having a high risk of hip displacement. 16 The location of the primary brain lesion was evaluated by pediatric neurologists and classified into GP, TP, or others using brain MRI. The typical GP and TP lesions are shown in Figure 1. Gestational age, birth weight, and complication of epilepsy were recorded retrospectively from the patients’ medical charts.
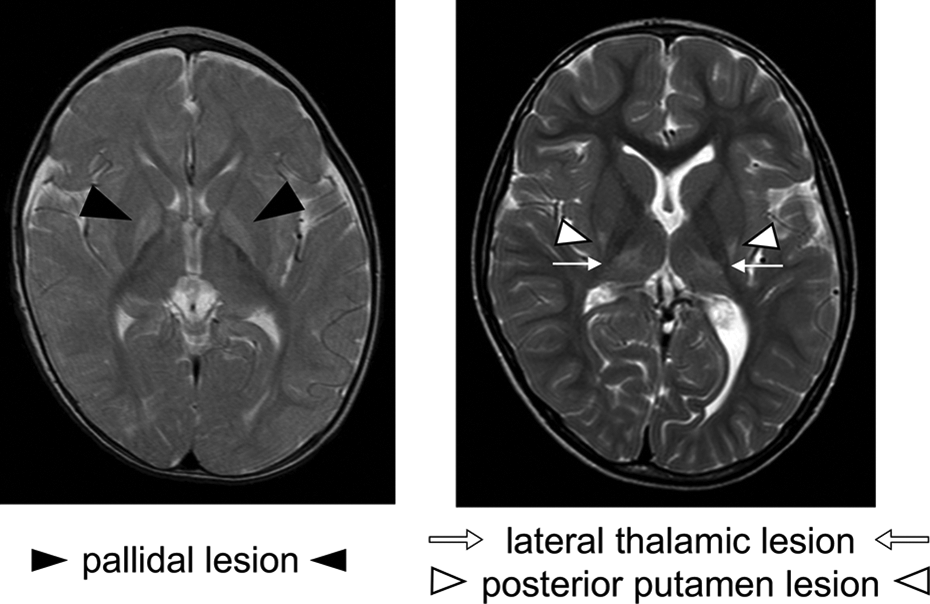
Exemplary images of primary brain lesion.
In the primary analysis, the presence of a GP lesion, Gross Motor Function Classification System (GMFCS) level, gestational age, birth weight, Cobb’s angle, and complication of epilepsy were used as independent variables in multiple logistic regression analysis. As a secondary analysis, GMFCS level, gestational age, birth weight, and onset age of hip displacement were compared between 32 patients with GP lesions and 42 patients with TP lesions. The age of onset of hip displacement was also compared between the GP (64 hips) and TP (84 hips) groups.
Statistical analyses
In the primary analysis, multivariate logistic regression analysis was performed to elucidate the independent risk factors for hip displacement. In the secondary analysis, the Mann-Whitney-U test was used to compare the continuous data, and the chi-square test was used to compare the categorical data between the two groups. Data analyses were performed using SPSS version 19 software (IBM Corp., Armonk, NY, USA). A p-value of <0.05 was considered statistically significant.
Results
A total of 81 patients (male: 45; female: 36) with DCP met the inclusion criteria. Demographic characteristics of the participants are summarized in Table 1. The average age at the last follow-up was 14.3 years (range: 10–22 years), and the average follow-up period was 9.4 years (range: 2–19 years). Brain MRI, conducted earlier than the age of 18 months, revealed that the primary brain lesions were located in the GP in 32 patients, TP in 42 patients, and other locations in seven patients. Sixty-eight patients (84%) were classified as GMFCS level IV or V. Fifty-three patients had hip displacements.
Clinical information of patients with dyskinetic cerebral palsy.
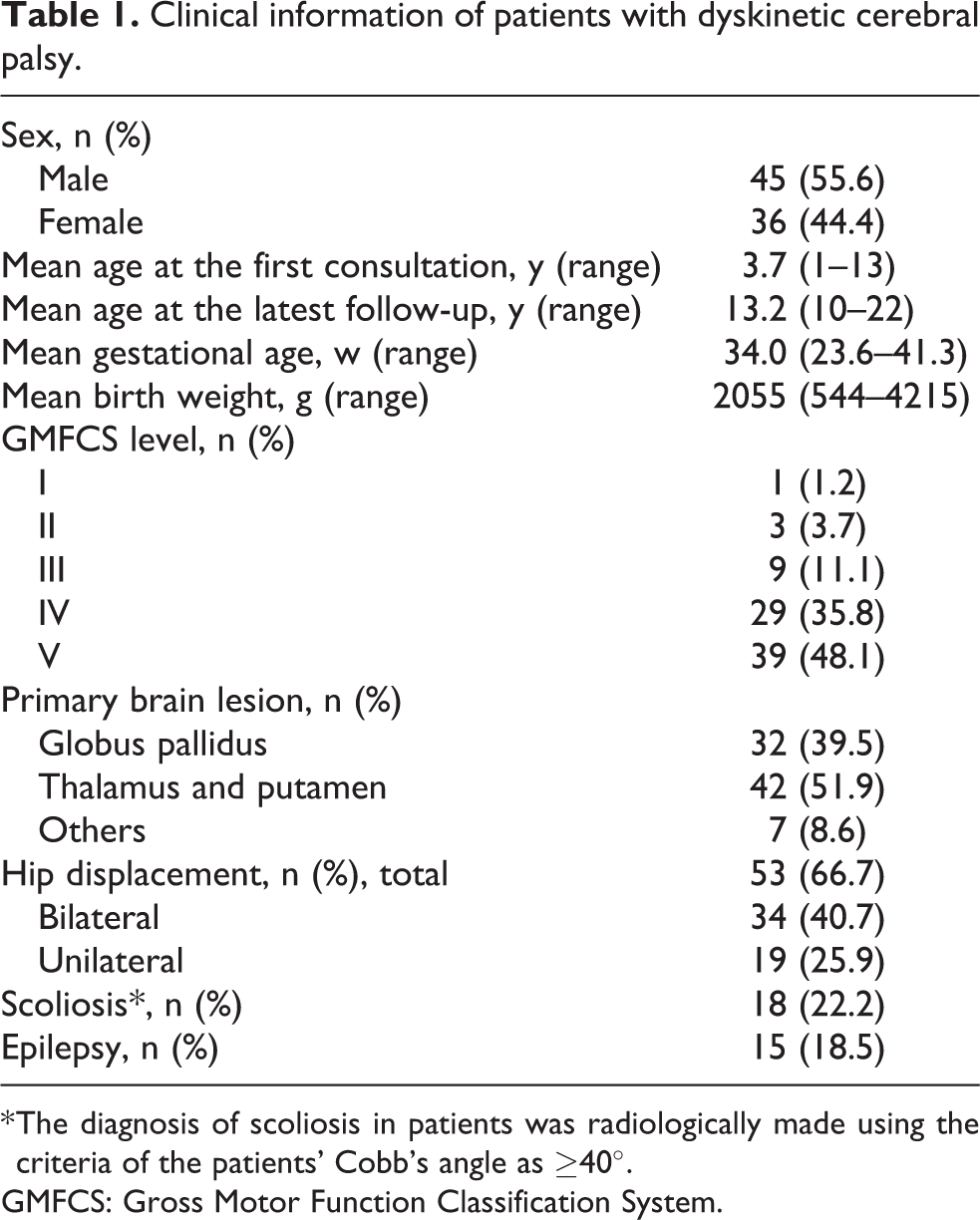
* The diagnosis of scoliosis in patients was radiologically made using the criteria of the patients’ Cobb’s angle as ≥40°.
GMFCS: Gross Motor Function Classification System.
Multiple logistic regression analysis revealed that the presence of GP lesion (odds ratio [OR] 16.5, p = 0.04) and higher GMFCS level (OR 2.6, p = 0.01) were independent risk factors for hip displacement (Table 2). The distribution of GMFCS levels in the GP group was significantly poorer than that in the TP group (p < 0.001), and the prevalence of hip displacement was significantly higher in the GP group (67.2%) than in the TP group (46.4%) (p = 0.013). However, the age of onset of hip displacement was not significantly different between the two groups (p = 0.17). Gestational age and birth weight were significantly lower (p < 0.001) in the GP group than in the TP group (Table 3).
Multivariate risk analysis for hip displacement among patients with dyskinetic cerebral palsy (case analysis).
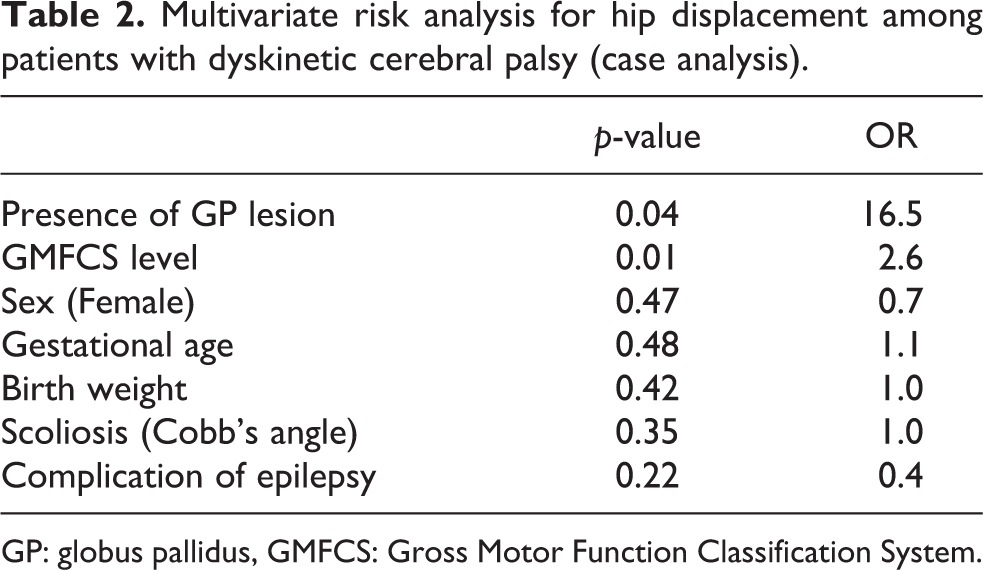
GP: globus pallidus, GMFCS: Gross Motor Function Classification System.
Comparison between the GP and TP groups.
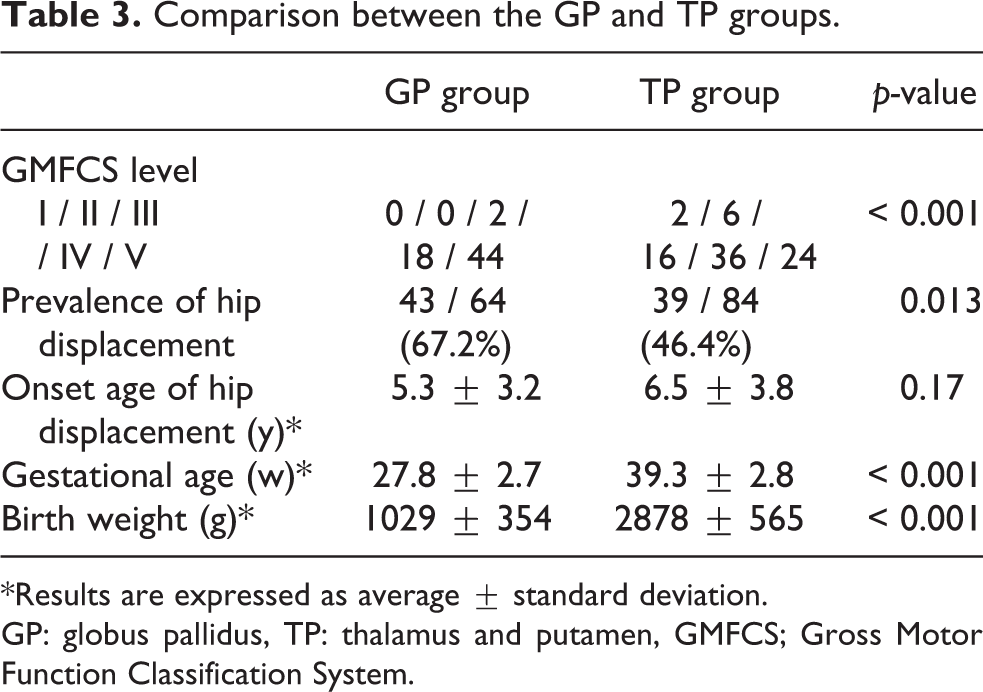
*Results are expressed as average ± standard deviation.
GP: globus pallidus, TP: thalamus and putamen, GMFCS; Gross Motor Function Classification System.
Discussion
CP is an umbrella term that covers various types of movement disorders with different etiologies and outcomes. Because it is necessary to restrict the CP type and etiology to predict outcomes more accurately, we included only patients with DCP and expanded the risk factor candidates to include perinatal factors and primary brain lesions. To the best of our knowledge, this is the first study to investigate the prevalence and risk factors of hip displacement, specifically in patients with DCP. Low gross motor function (high GMFCS level) is considered the risk factor for hip dislocation among patients with CP of all types, 6,16 Similar results were found in this study confined to patients with DCP, and patients with GP lesion were more likely to experience hip displacement than those with other lesions.
Previous studies on primary brain lesions in DCP have reported that the TP lesion was the most common. 14 It is caused by perinatal asphyxia among term-born neonates and manifests as mixed neurological signs of choreoathetosis, dystonia, ataxia, and spasticity. The second most common lesion has been reported to be the GP lesion caused by neonatal bilirubin encephalopathy. 14 Patients with DCP with GP lesions have characteristic excessive muscle tone and asymmetric dystonic posture resulting in severe motor dysfunction. 17 Severe dystonia is suspected to be caused by the disruption of direct and indirect pathways from the putamen, which coordinates volitional movement. 18 These findings emphasize the importance of understanding the pathological background of CP for the precise prediction of outcomes in the affected patients.
The prevalence of hip displacement in this study (67%) was higher than that reported in previous studies on CP. 6 –11 This may have been because the ratio of patients with GMFCS levels IV and V was higher in this study than in previous studies. 6,16 When limited to DCP, three studies reported that 10–48% of patients experienced hip displacement, which is a drastically lower proportion than that reported in this study. However, none of these three previous reports mentioned GMFCS levels of the patients with DCP. Two of the studies had an insufficient number of participants (n = 25 and n = 34), and two included much younger participants (mean age = 5.5 years and 7.88 years). 7,10,11
Another possible reason for the high prevalence of hip displacement in the present study is the greater proportion of patients with GP lesions (39.5%) than that reported in a previous study on DCP etiology (26%). 14 Multivariate logistic regression analysis revealed that not only GMFCS level but also the presence of GP lesion were independent risk factors for hip displacement in patients with DCP. Secondary analysis showed that the GP group had significantly higher GMFCS levels and prevalence of hip displacement than the TP group. Recently, bilirubin encephalopathy in very premature infants has received increasing recognition as an etiological determinant of DCP. 17,19,20 Indeed, most patients in the GP group in this study were very premature and of very low birth weight. Recent advances in perinatal medicine might help improve the survival ratio of very premature infants, which resulted in the increased number of patients with DCP who had GP lesions.
The primary brain lesion is determined using MRI before 18 months of age, 17 whereas the GMFCS level is usually ascertained after 2 years of age. Risk evaluation via brain MRI can facilitate earlier prediction of the future development of hip displacement among patients with DCP. It suggests that for patients in the GP group, shortening follow-up periods from a young age and providing early surgical treatment to prevent hip displacement improve the QOL of patients and caregivers.
In this study, the prevalence rate of bilateral hip displacement was 40.7% and that of unilateral hip displacement was 25.9% (Table 1), which is similar to that of the spastic type. 21 This may be caused by the fact that the muscle tone of the whole body in DCP is stronger than in the spastic type, although there is an asymmetric posture in both types.
Scoliosis was not related to hip displacement. The mean age of 13.2 years at the latest follow-up in this study was considered to be too young to develop scoliosis. A longer follow-up period may be necessary to examine the relationship between hip displacement and scoliosis in patients with DCP. Furthermore, a history of epilepsy was also not related to hip displacement. While epilepsy may affect activity and participation, it appears to have no relationship with the fixed posture that leads to contracture.
A major limitation of this study was selection bias. We recruited participants from our rehabilitation and orthopedic clinic, and our hospital is a central hospital for CP in West Japan. Therefore, participants tended to have relatively severe motor impairment and a high need for hip surgery. Indeed, there was only one patient with GMFCS level III and no patients with levels I or II in the GP group. Another limitation was that although all patients received physical therapy and used orthoses, the frequency, treatment methods, and orthoses usage time varied among them. This non-uniformity between the two groups may have influenced hip displacement.
Conclusion
Our results revealed that GP lesion was specific to very premature infants and was a significant risk factor for hip displacement among patients with DCP. Not only the GMFCS level but also a thorough assessment of primary brain lesion location and perinatal history should be considered for the early detection of hip displacement.
Footnotes
Acknowledgement
We would like to thank all the medical staff at Bobath Memorial Hospital.
Author contributions
KO: data acquisition, analysis and interpretation of data, drafting and critical revision, and final approval of the article.
YK, TS, HA: design, data acquisition, analysis and interpretation of data, drafting and critical revision, and final approval of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and informed consent
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the ethics committee of Omichikai Medical Corporation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.