
Abstract
Purpose:
Given that pediatric traumatic hip dislocations are relatively rare, the purpose of the current study is twofold: first, to contribute a significant cohort to the existing corpus, and second, to provide evidence toward the role that computed tomography and magnetic resonance imaging could play in identification and management of this type of injury.
Methods:
A retrospective review was conducted of all patients with traumatic hip dislocation who presented from 2012 to 2022 at a tertiary-level pediatric trauma center. Data regarding demographics, mechanism of injury, imaging, and treatment were tabulated. Outcomes of interest included immobilization length, concomitant injuries, imaging performed and findings, and rates of avascular necrosis, pain, and stiffness. Concomitant injuries were identified using imaging, clinical, and operative notes. Differences between categorical variables were compared using chi-square analysis or Fischer-exact testing, while continuous variables were compared using Student t tests or Wilcoxon rank sum tests when appropriate.
Results:
Thirty-four patients were identified. Postreduction, 28 patients had a cumulative 17 magnetic resonance imaging, 19 computed tomographies, and 1 intraoperative arthrogram. Of these, 16 patients had 19 injuries identified on advanced imaging that were missed on initial radiographs. Eleven of these patients went on to operative treatment. In eight of these, postreduction advanced imaging helped guide the decision for surgery. In four patients, magnetic resonance imaging was necessary to fully characterize injury to the posterior acetabular rim after initial identification on computed tomography. Magnetic resonance imaging was also used to rule out one computed tomography-diagnosed acetabular fracture.
Conclusion:
Magnetic resonance imaging is valuable to fully define associated rim and intra-articular injuries following initial treatment of pediatric traumatic hip dislocations.
Level of evidence:
Level IV diagnostic study.
Introduction
Pediatric traumatic hip dislocations are uncommonly occurring orthopedic emergencies, and have been described in a variety of circumstances, most commonly as a result of sport or motor vehicle collisions (MVCs).1–11 Current evidence suggests that successful timely reduction plays a critical role in preventing deleterious sequelae such as avascular necrosis (AVN) from developing; however, associated osteochondral or acetabular injuries may hamper the stability or concentricity of any attempted reduction.1,3,6,8,10–12 While radiographs both pre- and postreduction are established as standard of care in the management of this sort of injury, the role of computed tomography (CT) and especially magnetic resonance imaging (MRI) in the acute phase of managing traumatic hip dislocations in the pediatric population remains more heterogeneous.6,13–15
As a function of the developing skeleton’s pattern of ossification, injuries in the skeletally immature may not be readily apparent on plain radiographs or even CT. Fabricant et al. 16 demonstrated that posterior acetabular wall ossification typically occurs around 12–13 years of age, just prior to the closure of the triradiate cartilage. Therefore, accurate imaging is critical to fully understand these injuries, especially given that the majority are managed through closed reduction, in which direct visualization of intra-articular structures is impossible. With ever-increasing access to MRIs in the United States, more recent literature has purported the value of this modality in appropriately characterizing these potentially complex injuries.17–21
Given that hip dislocations with a traumatic etiology are relatively rare injuries in the pediatric cohort, the purpose of the current study is twofold. First, to contribute a significant cohort to the existing corpus. Second, to provide evidence of the role that advanced imaging (CT and MRI) could play in the identification and management of this type of injury. We hypothesize that both CT and MRI are likely to be effective ways in characterizing the extent and character of injury; however, MRI is more likely to be the most representative imaging modality of injury, given that MRI can more readily identify soft-tissue and cartilaginous injuries.
Methods
Following approval from the institutional review board (IRB), a single-center retrospective review was conducted of all patients with traumatic hip dislocation who presented to the emergency department or pediatric orthopedic outpatient clinic from 2012 to 2022 at a tertiary-level pediatric trauma center. All patients who suffered from traumatic hip dislocation aged ≤18 years were considered for inclusion in the study. Patients who lacked sufficient clinical documentation suffered from complex polytrauma, or had a history of previous ipsilateral hip surgery excluded from the study.
Electronic medical records from the initial emergency department presentation to the most recent follow-up visit were queried and reviewed manually to identify eligible patients. After a thorough chart review, data regarding demographics, mechanism of injury, imaging, treatment, follow-up length, and outcomes were extracted from all relevant records including those from outside institutions. The treatment and outcome variables of interest were postreduction immobilization, pre- and postreduction imaging modalities, findings on imaging, concurrent fractures and injuries, operative management, reported pain, stiffness, AVN, and time to return to sports. Findings on imaging were extracted from the radiology reports and the treating surgeon’s documented interpretations of the imaging. Representative imaging was also collected at this time. Concomitant injuries were identified using imaging reports and intraoperative findings as documented in the operative notes. Skeletal maturity was defined as complete closure of the triradiate cartilage and closure of the proximal femoral physis. All operations were performed by fellowship-trained pediatric orthopedic surgeons working directly with a fellowship-trained adult orthopedic traumatologist. Study data were then collected and managed using REDCap electronic data capture tools hosted at the (blinded).22,23 Differences between categorical variables were compared using chi-square analysis or Fischer-exact testing, while continuous variables were compared using Student t tests or Wilcoxon rank sum tests when appropriate. All data were cleaned and analyzed using Microsoft Excel and IBM SPSS statistical analysis software.24,25
Results
After an exhaustive chart review, 34 patients (34 hips) were identified. Twenty-four were male, 10 were female, with an average age at time of injury of 11.2 ± 4.9 years. The cohort’s average body mass index (BMI) was 20.9 kg/m2. After removing patients with inadequate (< 3 months) or ongoing follow-up (n = 11) average length of follow-up was 0.94 (SD: 0.91 years, median 0.73 years, range 0.29–4.12 years). Lost to follow up was defined as patients who did not present for follow-up care following initial encounter and reduction of their hip. Length of follow-up was defined as the time from reduction to the time of most recent clinical visit. Fourteen of the dislocations were on the right and 20 were on the left. Eight patients were considered skeletally mature at time of injury; 26 were skeletally immature.
The etiologies of the traumatic hip dislocations were recorded in Table 1. Twenty-five of our 34 patients had “low-energy” injuries secondary to sports or a fall from standing. Of the 21 sporting injuries, 11 were related to football (52.38%). One hip was dislocated anteriorly, and the rest were posterior. Individual patients’ age, sex, follow-up length, mechanism of injury, laterality of injury, and prereduction CT/MRI are recorded in Table 2. Table 3 includes key postreduction CT and MRI findings for each patient, when available. Table 3 also includes any operative intervention. Figure 2 includes representative imaging of injuries identified on postreduction MRIs.
Demographics and descriptive data of patient cohort, including differences in diagnosis of MRI following CT.
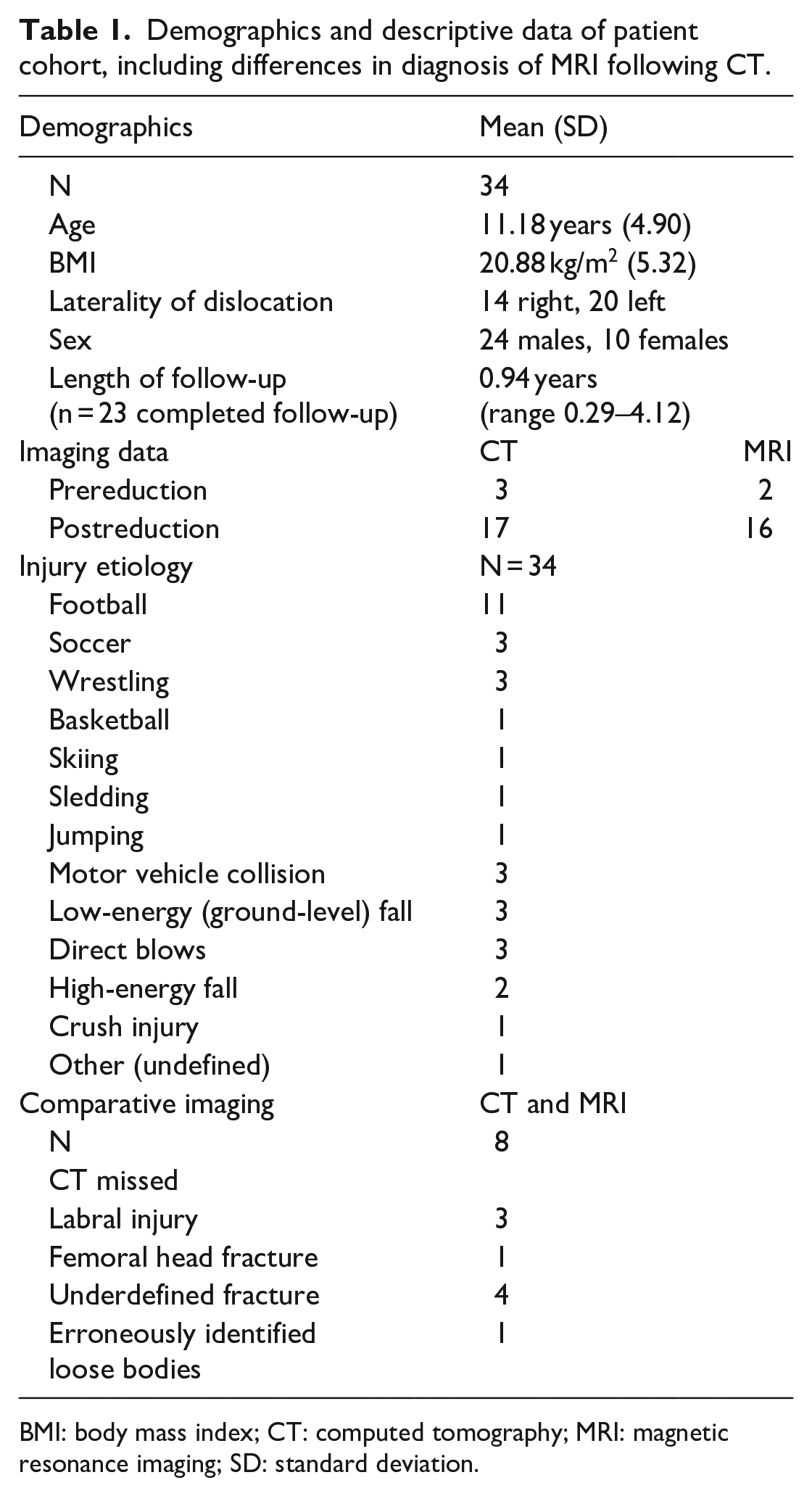
BMI: body mass index; CT: computed tomography; MRI: magnetic resonance imaging; SD: standard deviation.
Individual patient characteristics.
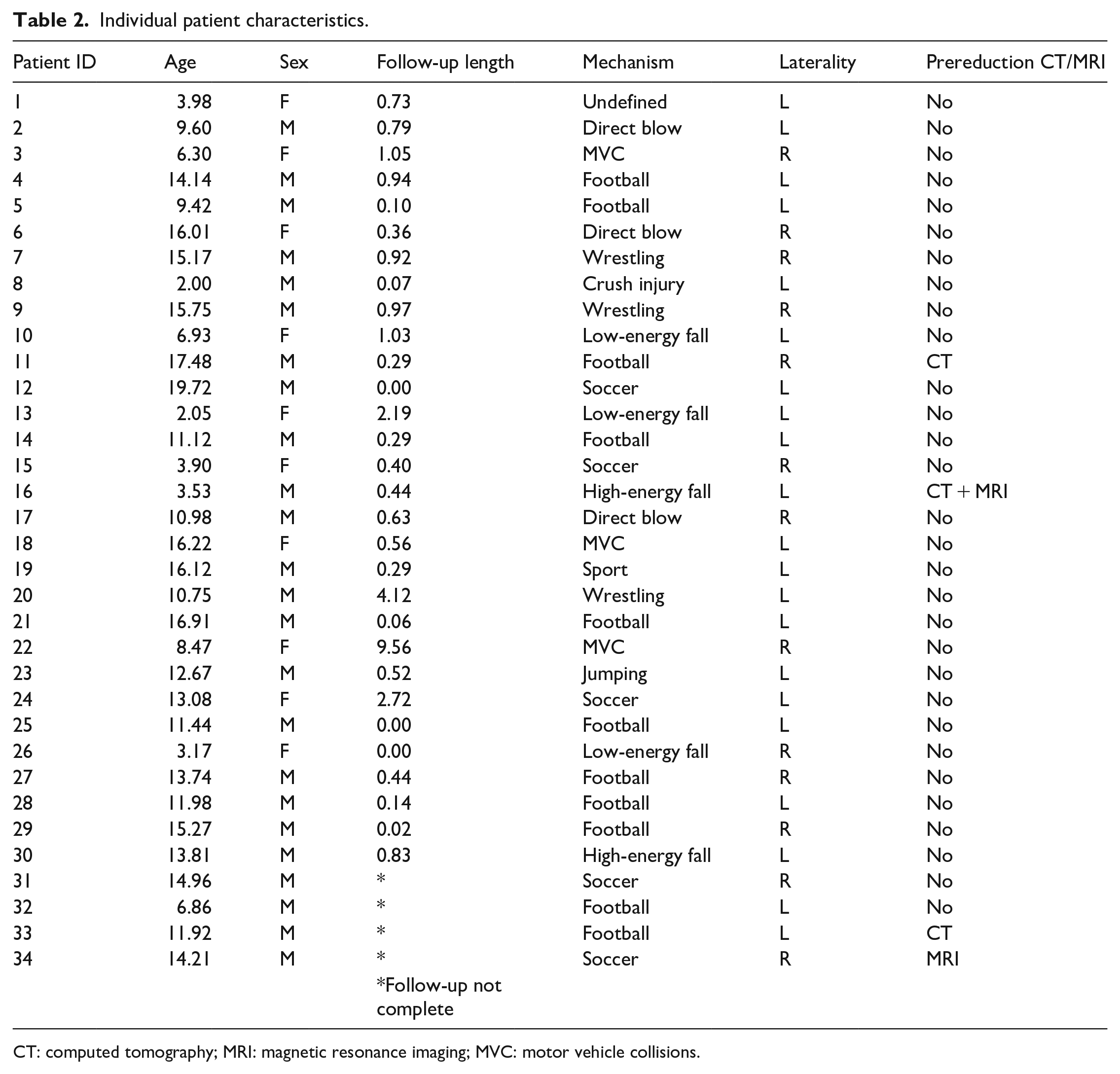
CT: computed tomography; MRI: magnetic resonance imaging; MVC: motor vehicle collisions.
Individual patient descriptions of postreduction CT and MRI, including key findings and operative status.
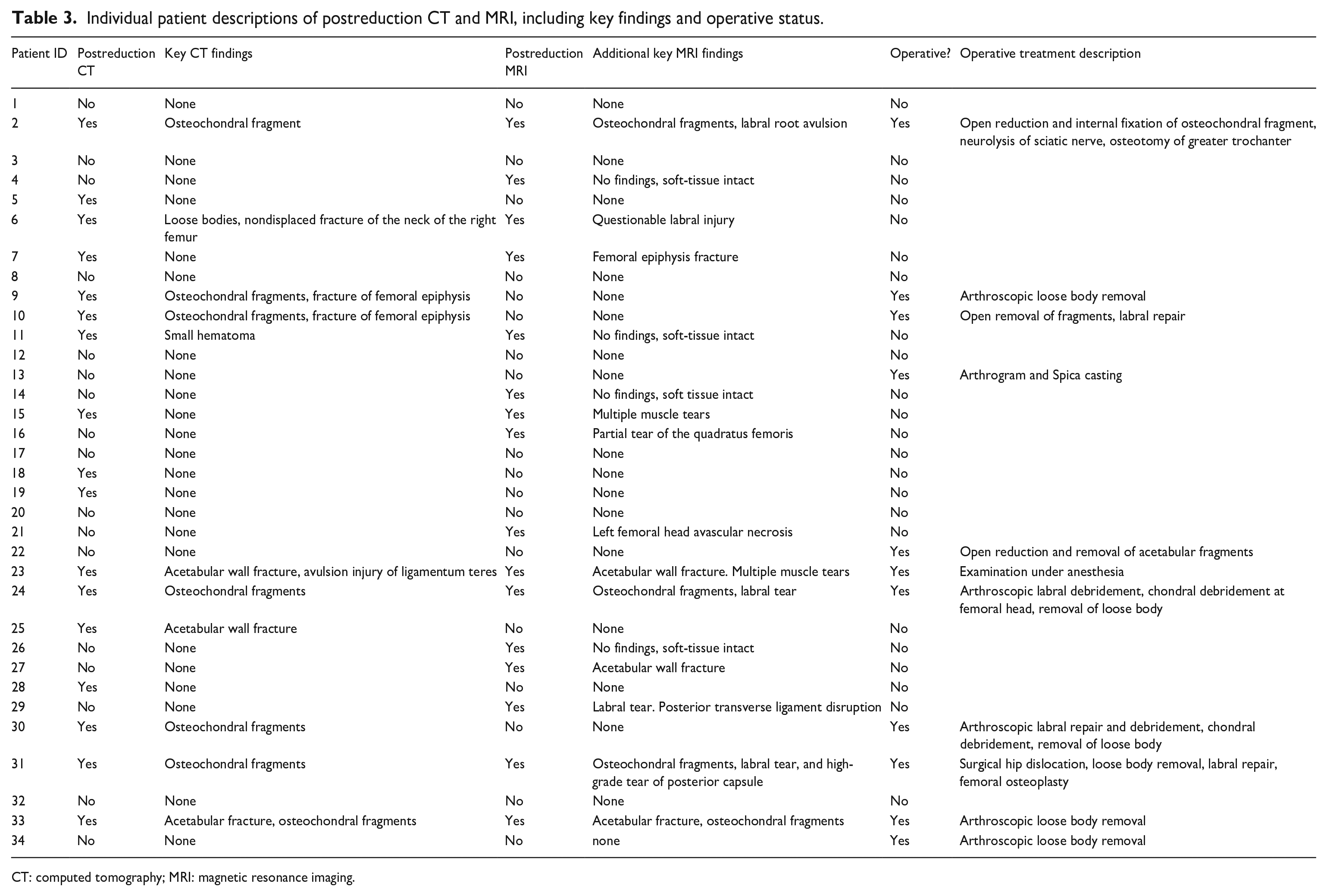
CT: computed tomography; MRI: magnetic resonance imaging.
Only 4 of the 34 patients had prereduction advanced imaging, of which 3 were CTs and 2 were MRIs (one patient had both). Two of the four patients who received advanced imaging prior to reduction went on to receive operative treatment. There were 17 concomitant fractures across our 34 patients. Two were of the pelvic ring, eight of the posterior acetabular wall, two of the acetabular columns, and five of the femoral head. Eight of these resulted in intra-articular bodies that required surgical removal. One was identified with postreduction MRI only, four with CT only, and three with both CT and MRI. Fischer’s exact test demonstrated no significant relationship between prereduction advanced imaging and the presence of a concurrent fracture (p = 0.611) nor of operative management (p = 0.602).
Postreduction, 27 patients had a cumulative 16 MRIs, 17 CTs, and 1 intraoperative arthrogram. Of these, 16 patients (59%) had 19 injuries identified on advanced imaging that were not characterized by initial radiographs. Of our eight skeletally mature patients, half (n = 4) had missed injuries between their initial imaging and follow-up advanced imaging. There were 13 osteochondral fragments, 3 labral injuries, and 3 femoral head fractures (Figure 1). Nine of these patients received both CT and MRI (Table 1). MRI was able to rule out an acetabular fracture that was previously diagnosed by CT in one instance. MRI also identified a subtle fracture of the right femoral epiphysis and three labral injuries missed by CT. Outside of the preceding cases, CT was able to identify all bony injuries, though in four patients, MRI was necessary to fully characterize injury to the posterior acetabular rim after initial identification on CT. Patients who had concomitant acetabular fractures were more likely to have operative treatment than those who did not (p < 0.001).
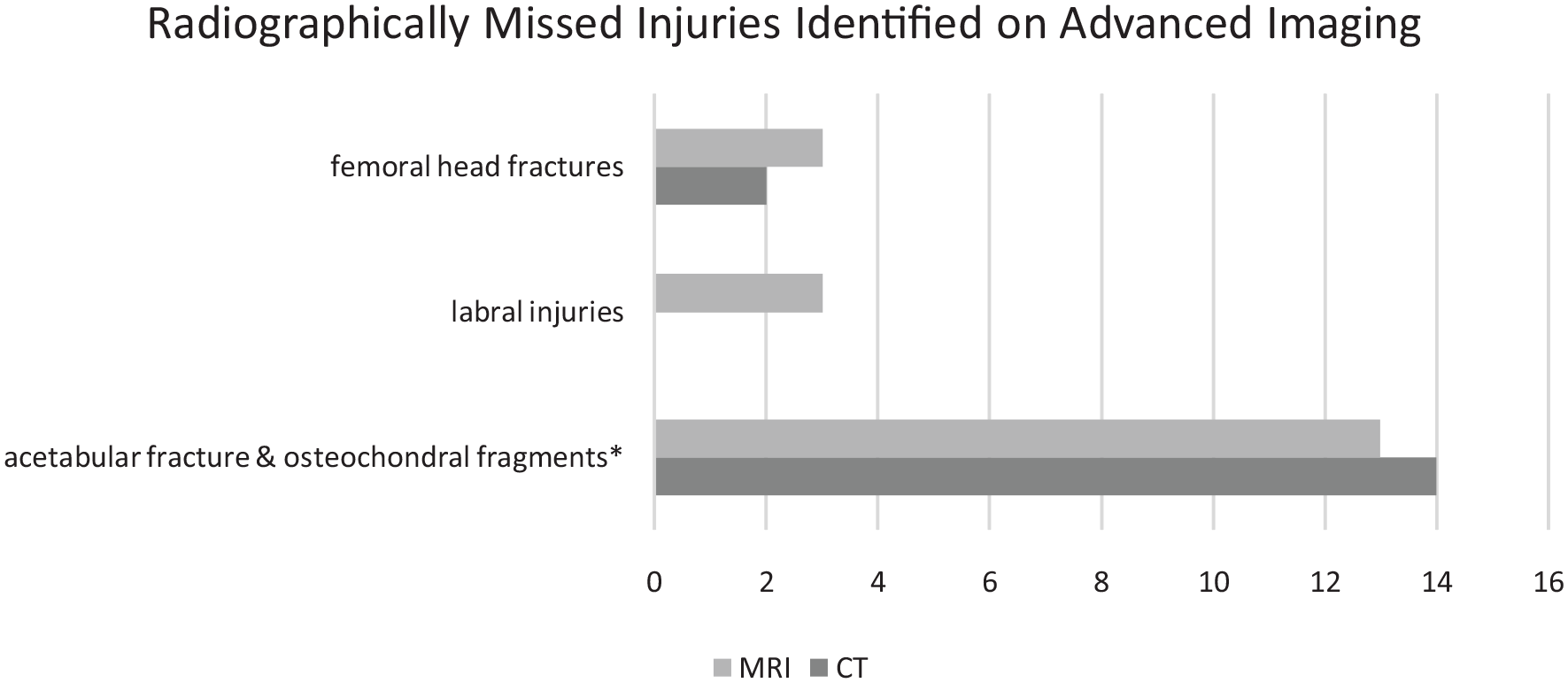
Injuries captured on MRI or CT after being missed on initial radiograph.
Ultimately, 11 cases were managed operatively: five arthroscopically, four by open techniques, one with a spica cast, and one as an examination under anesthesia (Figure 2). In eight of these, postreduction advanced imaging helped guide the decision to operate. There were no cases that returned to the operating room nor complications such as infections, fracture nonunions, or fracture malunions. Three cases had postreduction stiffness documented—all of which were initially treated with arthroscopy. There were two AVN cases reported. Both presented with complaints of pain at follow-up visits. One was diagnosed at 5.5 months after the initial injury, while the other was diagnosed 34.3 months after injury, both through MRI. Only one had advanced imaging at the time of hip dislocation, which revealed a concurrent fracture, but no other findings. Neither was treated operatively for their hip dislocation, though both underwent core decompression for the AVN that followed. One AVN patient returned to sports with no restrictions, while the other was lost to follow up following her core decompression.
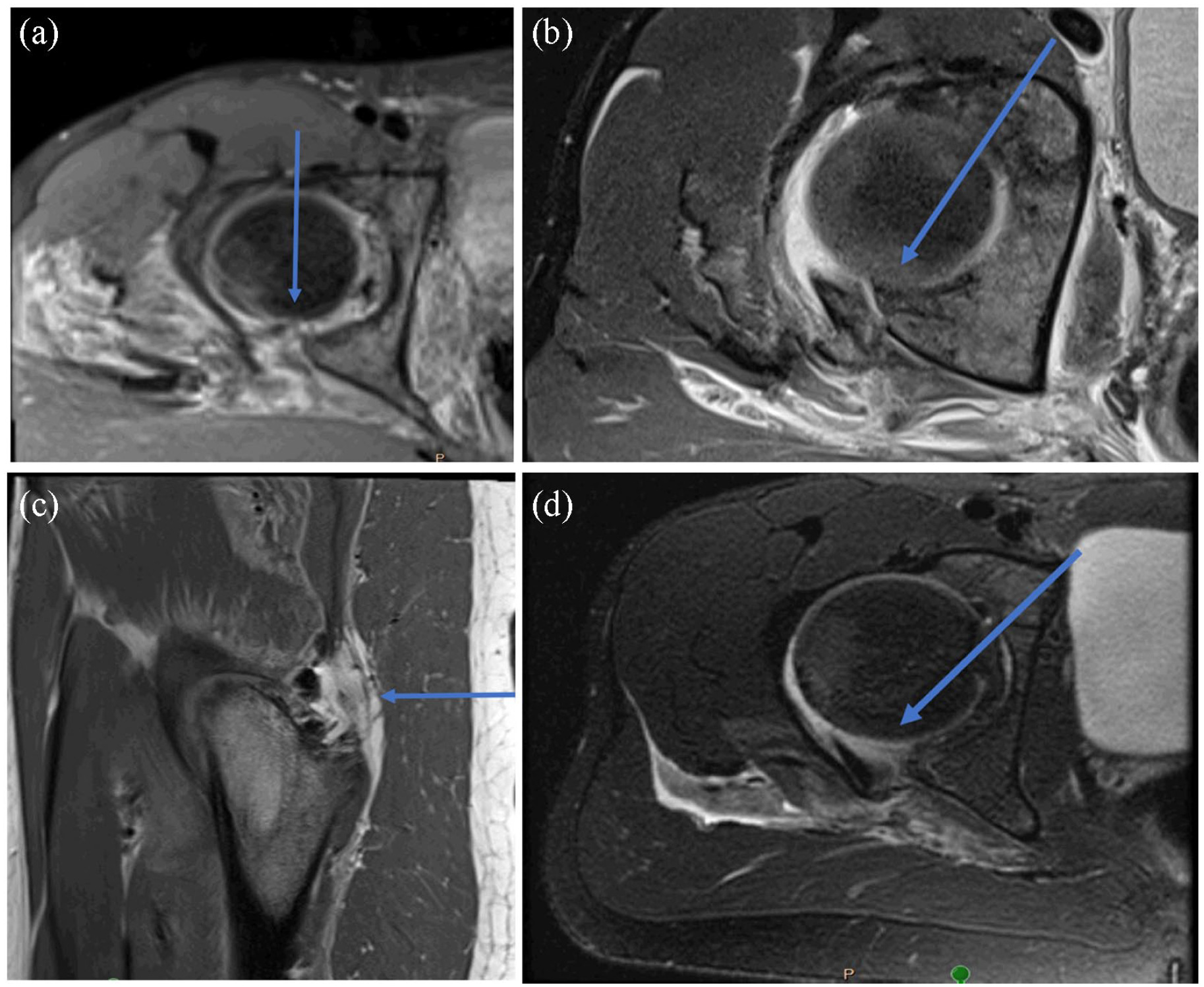
Representative slices from postreduction-MRI (injury labeled with blue arrow). (a) Labral tear. (b) Osteochondral fragments. (c) Gluteus medius tear. (d) Labral tear.
Though some patients (n = 11) did not have explicit return to sport time documented, we found that of the patients that did, the average time to return to sport in patients who did not have an operation (n = 15) was 3.78 months (SD: 2.09). Operative patients with available return to sport time (n = 8) did so in an average of 7.41 months (SD: 4.24). When examining the entire cohort, return to sport was 5.04 months (SD: 3.41).
Discussion
This study builds on existing literature about traumatic hip dislocations in pediatric patients. While previous literature has shown that timely reduction (<6 h from index injury) lowers the risk of devastating long-term sequelae, few other studies report on the role of imaging in the accurate characterization of the extent of the injury.1,7 Due to ligamentous laxity, children have been reported to have more hip dislocations as a result of lower energy mechanisms compared to adults.26,27 This is in line with our findings, as 25 of our 34 patients in our sample had a sports-related injury or a ground-level fall. Furthermore, of the 21 sport-related injuries, 11 were related to football (52.38%). Our study also described a significant difference in rates of concomitant injury and fracture in patients who required operative management; however, of our high-energy etiology patients, only three MVC etiology patients advanced to surgery, and one of our direct blow-etiology patients advanced to surgery (patient 2).
The use of MRI in the diagnosis and severity stratification of traumatic hip dislocations has been described increasingly in the last two decades. In 2002, Rubel et al. 20 presented two cases where posterior acetabular injuries were missed or under-reported on all imaging modalities except MRI. This study concluded that MRI could disclose the true size of the lesion, thus guiding management decisions in a way that CT and X-ray could not. This finding was expanded upon in 2015 when Mayer et al. 17 described a cohort of nine patients who had MRIs after a posterior dislocation. This imaging modality was able to identify all intraoperatively confirmed lesions preoperatively, while CT imaging underestimated posterior wall injuries given the later ossification of this structure during normal development.16,17 In 2018, Strüwind et al. 14 demonstrated the utility of MRI in identifying labral interposition following closed reduction of these dislocations, especially given that two of their patients who had a free body identified on CT had missed labral interpositions when subsequently managed operatively. Similar findings were reported by Thanacharoenpanich et al. 28 in 2020, who found that not only did MRI capture all bony injuries also identified by CT, but MRI also identified one posterior acetabular injury and three labral entrapments that CT could not. Furthermore, the authors describe a case of a persistently unstable hip that was due to an incompletely ossified acetabular fragment missed on all imaging except MRI. These findings are supported by our own, as MRI identified three labral injuries and a single femoral head fracture not captured by CT.
While pathognomonic indicators for traumatic hip dislocation present on advanced imaging (CT and MRI) have been proposed, the most notable is the CT “fleck sign” for labral injury by Blanchard et al. 13 In 2005, Vialle et al. 6 noted that CT identified all acetabular wall fractures through the usage of the aforementioned “fleck sign” but could not identify avulsion of ligament teres or acetabular lip interposition. As Thanacharoenpanich et al. 28 describe in their study, it is difficult to resolutely identify causes of incongruous reduction through indirect measures such as joint space widening; thus, they advocate for more routine MRI evaluation to evaluate soft-tissue structures in conjunction with more ossified structures. Future work should center on codifying MRI findings to better support time-efficient and accurate clinical decision-making.
It has also been noted by Shaath et al. 29 that in the skeletally immature, CT imaging provides a significant advantage in the diagnosis of acetabular fractures; they conclude that radiographs alone may lead to missed acetabular fractures. In our series, we identified 19 injuries that were missed on initial radiographs, of which four patients were skeletally mature (n = 8). As 50% of our skeletally mature patients had an injury that was initially missed, it is difficult to justify reserving advanced imaging only for the immature; however, our findings do support the efficacy of CT and MRI for identifying fractures in the skeletally immature as well. Furthermore, in our cohort, 40 advanced imaging studies either CT or MRI) helped in the clinical decision-making that led to nine actual surgeries (a rate of 22.5%). Thus, the benefit of advanced imaging is twofold including better diagnosis of potential intra-articular injuries and fractures as well as for surgical planning should operative management be necessary. As such, we perform CT or MRI routinely for all traumatic dislocations, especially if we have a high clinical suspicion for missed injuries or incongruent reduction based on plain radiographs. However, advocating for the routine use of such imaging modalities would be incomplete without weighing the cost and potential risks of widespread implementation. When compared to conventional radiographs, CT and MRI are significantly more expensive and may require additional healthcare resources such as anesthetists to provide sedation for noncompliant patients. Previous work has attempted to study the cost-effectiveness of different imaging modalities in children; however, it is difficult to draw any definitive conclusions given the dearth of data surrounding traumatic hip dislocations in this arena. 30 The authors of this study hope that our findings and implications regarding the utility of advanced imaging can serve as a foundation for future work in this space.
Our rates of AVN are similar to that which is published in the literature (n = 2/34, or 5.88% compared to 6% by Hougaard and Thomsen, 5 12% by Mehlman et al., 8 and 13.6% by Hung et al. 9 ). Our cohort had an average follow up of 0.94 years (SD: 0.91). Given this follow-up, it is possible that certain cases may have been missed if osteonecrosis were to develop after the most recent appointment. That said, it is our experience that the vast majority of AVN following traumatic injuries such as hip dislocations, femoral neck fractures, and unstable slipped epiphyses occur within the first 9 months of injury. Also similar to existing literature, the majority (33 of 34, 97.05%) of injuries in our series were posterior dislocations. A large literature review reported posterior dislocations at a rate of 95.8%. 11 In terms of general outcomes, we found that our cohort returned to sports on average 5.04 months following reduction; however, there are scant data regarding this timing in the literature with which to compare our data. Authors such as Mehlman et al. 8 have instead reported that 33 of their 42 patients returned to “high-demand activities,” which included several sports following traumatic hip dislocation.9,31
Our study had several limitations. First, this study was retrospective. Not all patients had complete data, but given the nature and rarity of this injury, the authors felt it appropriate to include patients with available data in analysis and disclose where some patients were excluded given the lack of data. This is most marked with patients who were transferred to our institution. As a large referral center, many patients were initially seen in an outside emergency department and transferred to our institution or were first managed elsewhere before referral. This variation in presentation also explains differences in initial management. For example, in our cohort, only one patient with a fracture received an examination under anesthesia which is routinely performed at certain centers. At our hospital, this is primarily reserved for larger posterior wall fractures where gross stability may be compromised. Most of our patients in this series had small posterior rim injuries or isolated dislocations and as such did not undergo further workup with examination under anesthesia. Next, data are not uniformly available from these patients, though the data were extracted as best as possible. Patients with missing data points were excluded from analysis where appropriate. In addition, imaging protocols were not described nor easily captured through chart review, and so the authors cannot guarantee a standard protocol was applied; despite this, images were all reviewed by radiologists and attending surgeons at a single large institution. Similarly, clinical interpretation of available imaging was completed by the radiologist on staff at the time of imaging, and so there was no possibility of standardizing quality of the interpretation. Time to CT or MRI were not data points that could be standardized, and so some findings that may have been present at different time points, especially soft-tissue injury, may be missing from the radiologist’s interpretation. In addition, patients were selected based on their injury and analysis conducted on their treatment post hoc; therefore, verification bias could not be completely eliminated from this study. Existing literature has also discussed the additional value of MRI during the follow-up period in identifying AVN; however, as this study only had two cases of AVN recorded, no conclusions were drawn. Advanced imaging (CT or MRI) helped guide the decision to operate in eight patients. Because of the retrospective nature of this study, however, we are unable to determine how often advanced imaging helped the treating surgeon decide not to operate, which is equally important. Finally, we acknowledge that skeletal maturity may play a role in the presentation and behavior of these injuries and the utility of MRI and CT. We have included a small number of skeletally mature patients within this “pediatric” cohort as this is the series that presented to our institution, and limited numbers make it difficult to perform meaningful subanalyses of these two groups.
In conclusion, this study sought to contribute to the existing literature for a rare injury, as well as provide data on the value of advanced imaging, as recommendations remain relatively scant. While CT and MRI are both valuable in characterizing the injury and reduction, this study found that MRI was capable of detecting both bony and soft-tissue injuries that may otherwise be missed, thereby providing important and potentially operatively relevant data to the surgeon. The current study substantiates our recommendation of more liberal usage of MRI after initial reduction of traumatic hip dislocations in children.
Footnotes
Author contributions
D.Y., J.L., K.O., A.S., and W.S. conceived and designed the analysis. D.Y., J.L., K.O., and M.B. collected the data and contributed analysis tools. D.Y., J.L., and K.O. completed the analysis. All authors contributed to drafting and critical revisions, as well as final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.