
Abstract
Purpose:
To compare the sagittal alignment of different surgical approaches in patients with multiple levels cervical spondylotic myelopathy and explore the relationship between the cervical sagittal alignment and patient’s health relative quality of life.
Method:
A total of 97 multiple levels cervical spondylotic myelopathy patients who underwent surgery from January 2013 to January 2019 were collected in this study. Patients were divided into three groups: anterior cervical discectomy with fusion, anterior cervical corpectomy with fusion and laminectomy with fusion groups. Clinical outcomes and sagittal alignment parameters were compared preoperative and postoperative.
Results:
There were no significant differences in the average age and sex ratio among the groups. Sagittal parameters correlated to health relative quality of life were C7 slope, occipito-C2 angle, external auditory meatus tilt and cervical sagittal vertical axis. Both anterior cervical discectomy with fusion and anterior cervical corpectomy with fusion groups exhibited better sagittal alignment and clinical outcomes improvement postoperatively. Anterior cervical discectomy with fusion provided better clinical outcomes and the better improvement of cervical lordosis, C7 slope, occipito-C2 angle and cervical sagittal vertical axis compared with patients with Laminectomy with fusion.
Conclusion:
C7 slope, occipito-C2 angle, external auditory meatus tilt and cervical sagittal vertical axis are the most important cervical sagittal parameters correlated to clinical outcomes in patients with multilevels cervical spondylotic myelopathy; anterior cervical discectomy with fusion and anterior cervical corpectomy with fusion provides more efficient to restoration of cervical sagittal alignment.
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) represents one of the most common causes of progressive spinal cord dysfunction in the adult population. 1,2 The degeneration of the intervertebral disc, uncovertebral joint, facet joint, posterior longitudinal ligament, and ligamentum flavum causes spinal cord compression and cervical myelopathy. 3,4 Multilevel CSM (mCSM) refers to CSM which involving two or more segments, and surgical treatment is the only effective strategy for mCSM because of the spinal cord and nerve root compression. 5
Radiographic evidence indicated that CSM often accompanied with abnormal sagittal alignment, disappearance of intervertebral space, reducing curvature, and alteration of the neck pillow position. 6 Human sagittal balance mainly consists of three parts: the sagittal plane alignment of the spine, the sagittal plane alignment of the pelvis and the sagittal plane alignment of lower limbs. 7,8 Recently, cervical sagittal alignment has also been considered to be a diverse and important part for the global sagittal alignment. 7 The cervical spine compensatory mechanism plays a critical role in achieving horizontal gaze and keeping head-trunk accordance. 9,10 In addition, lot of literatures demonstrated that cervical sagittal alignment is associated with Health relative quality of life (HRQOL) and clinical outcomes of CSM patients. 11 –14 Therefore, it is important to evaluate and correct the cervical sagittal alignment in the process of surgical treatment.
Surgical approaches of mCSM are mainly divided into anterior, posterior and combined approach. Anterior approaches include anterior cervical discectomy with fusion (ACDF) and anterior cervical corpectomy with fusion (ACCF); posterior approaches include laminectomy (LT), LT with fusion (LTF) and laminoplasty (LP). 15 In the past, it is generally believed that both anterior and posterior approaches have their advantage and disadvantage. 5 However, the effect of the surgical approaches on the cervical saigttal balance and clinical outcomes is still unclear.
The purpose of this study was to compare the sagittal alignment of different surgical approaches and explore the relationship between the cervical sagittal alignment and clinical outcomes. The results may provide information for approach selection for mCSM in the aspect of achievement of better postoperative sagittal alignment.
Material and method
Patient population
This is a retrospective clinical study. From January 2013 to January 2019, clinical data from a total of 97 patients with mCSM who underwent surgery were collected at the First Affiliated Hospital of Sun Yat-sen University. mCSM inclusion criteria were as follows: Patients with CSM and radiographic evidence indicated that at least two or more levels with stenosis and localized instability.
Exclude criteria were as follows: patients with single level CSM, idiopathic scoliosis, spinal tumor, spinal fracture, spinal surgical history, serious osteoporosis, infection and mixed ossification of posterior longitudinal ligament (OPLL). A complete radiographical series consisting of preoperative and postoperative posteroanterior and lateral view radiographs were recorded. Approval of the institutional review board at the First Affiliated Hospital of Sun Yat-sen University was obtained prior to study.
Surgical procedures
All surgical procedures (ACDF, ACCF, LTF) were performed by one of two senior spine surgeons. All patients were performed standard decompression, internal fixation and fusion. 16 –18 For anterior approach surgery, patients were placed in the supine position, and surgery was carried out under general anesthesia with endotracheal intubation. Briefly, of the ACDF procedures, the posterior longitudinal ligament was removed in all cases at the discectomy sites. Allogeneic bone graft was used to fit the discectomy sites. The grafts and PEEK interbody cage were inserted between the vertebral bodies to restore the intervertebral disc space and cervical lordosis. Anterior cervical plating was done. For the ACCF procedures, the posterior wall of the vertebral body and posterior longitudinal ligament were removed. Then, titanium mesh filled with local autograft bone was used to span the defect generated by corpectomy/corpectomies. For posterior approach surgery, patients were placed in the prone position, and surgery was carried out under general anesthesia with endotracheal intubation. Briefly, of the LTF, the amount of facet joint resection varied per level and side, removing as much as necessary to adequately decompress the cord and nerve roots. Facet joints were decorticated with a drill or curette and then packed with bone graft. Lateral mass plates were applied to decompressed segments and lateral mass screws placed bilaterally at each level. Lateral mass screws were placed in a unicortical fashion in most cases. Bicortical screw purchase was only used in cases with osteoporotic bone when unicortical screw purchase was not satisfactory. Fusion spanned all decompressed levels but did not extend to adjacent vertebra with intact lamina. Additional bone graft was placed over the lateral masses.
Radiographical assessment
The films were digitized and stored using PACS (Picture Archiving and Communication Systems; Shenzhen Annet Information System, China). The following sagittal parameters were measured as described in previous studies (Figure 1). 14,19 –22 Briefly, cervical lordosis (CL) was measured as the cobb angle between C2 and C7; C1-C2 cervical lordosis (proximal CL, PCL) was measured as the cobb angle between C1 and inferior endplate of C2; C7 slope was measured as the angle subtended by the horizontal line and the inferior endplate of C7; occipito-C2 (OC) angle was measured as the angle between the McGregor line and the inferior endplate of C2; external auditory meatus (EAM) tilt was measured as the angle between vertical and the line joining the center of C7 and EAM; cervical sagittal vertical axis (CSVA) was measured as the distance between C2 and C7 plumb line.

Schematic drawings of the sagittal alignment parameters. Cervical lordosis (CL) was measured as the cobb angle between C2 and C7; C1-C2 cervical lordosis (proximal CL, PCL) was measured as the cobb angle between C1 and inferior endplate of C2; C7 slope was measured as the angle subtended by the horizontal line and the inferior endplate of C7; Occipito-C2 (OC) angle was measured as the angle between the McGregor line and the inferior endplate of C2; external auditory meatus (EAM) tilt was measured as the angle between vertical and the line joining the center of C7 and EAM; Cervical sagittal vertical axis (CSVA) was measured as the distance between C2 and C7 plumb line.
Outcome assessment
Three self-assessment health relative quality of life (HRQOL) measures were obtained from each patient: neck disability index (NDI), visual analog pain scale (VAS), and Japanese orthopedic association (JOA) scale. Outcomes measured were obtained preoperatively and postoperatively.
Statistical analysis
Data were analyzed using SPSS 16.0 (SPSS, Inc., Chicago, IL). Categorical variables were compared between the two groups using the χ2 test. Comparative studies were conducted with paired t test, one-way ANOVA, and the Bonferroni post hoc test. A correlation study was conducted with the Pearson correlations analysis. Data were presented as mean value ± standard deviation and statistical significance was indicated at p < 0.05.
Result
Comparative study of HRQOL in different surgical groups
A total of 97 mCSM patients (34 in ACDF group, 27 in ACCF group and 36 in LTF group) were included in this part of study. The average age was 52.97 ± 12.00 in ACDF, 59.33 ± 9.32 in ACCF and 55.64 ± 10.10 in LTF patients. There were no significant differences in the average age, sex radio (Table 1).
Demographic and clinical data of MCSM patients in different groups.

ACDF, anterior cervical discectomy with fusion; ACCF, anterior cervical corpectomy with fusion; LTF, laminectomy with fusion.
Table 2 summarized the comparative analyses of HRQOL among ACDF, ACCF and LTF groups. No significant differences were shown in the preoperative HROQL among ACDF, ACCF and LTF groups. Compared with ACDF and ACCF groups, LTF group showed significantly higher NDI scores (10.21 ± 3.49 vs 13.75 ± 4.07, p < 0.05) (10.99 ± 2.83 vs 13.75 ± 4.07, p < 0.05); ACDF and ACCF group also showed greater variance in △NDI (−3.82 ± 3.57 vs −2.06 ± 2.66, p < 0.05) (−3.05 ± 2.63 vs −2.06 ± 2.66, p < 0.05) and △VAS (−1.47 ± 1.28 vs −0.78 ± 1.10, p < 0.05) (−1.81 ± 1.04 vs −0.78 ± 1.10, p < 0.05).
Comparative study of HRQOL in different surgical groups.
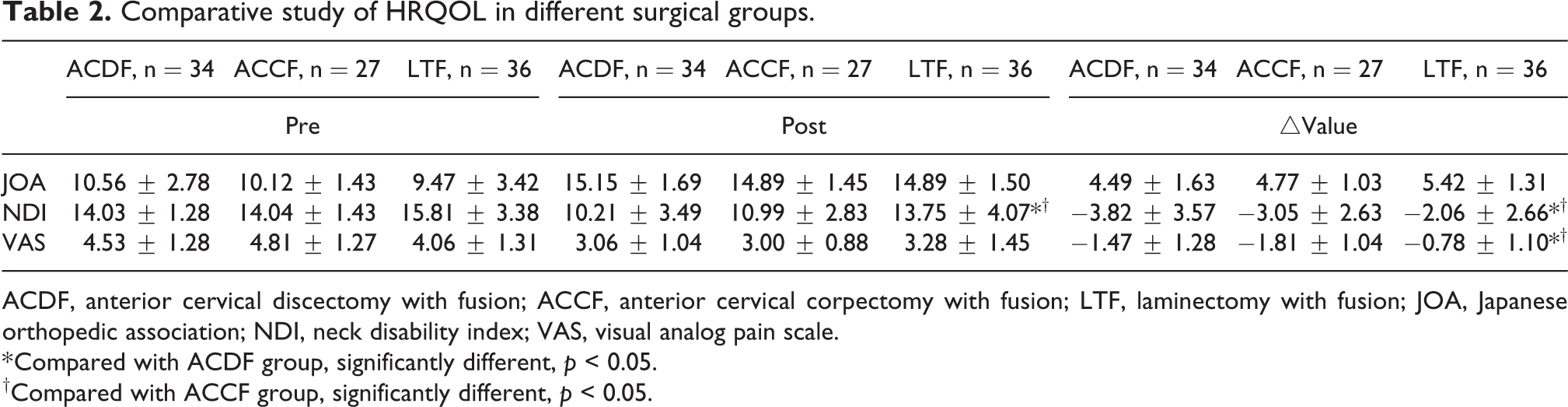
ACDF, anterior cervical discectomy with fusion; ACCF, anterior cervical corpectomy with fusion; LTF, laminectomy with fusion; JOA, Japanese orthopedic association; NDI, neck disability index; VAS, visual analog pain scale.
* Compared with ACDF group, significantly different, p < 0.05.
†Compared with ACCF group, significantly different, p < 0.05.
Comparative study of sagittal parameters between preoperative and postoperative measurements in different surgical groups
Table 3 summarized the comparative analyses of sagittal parameters between preoperative and postoperative in different surgical groups. In ACDF group, significantly increased CL (16.80 ± 9.47 vs 19.19 ± 8.67, p < 0.05), C7 slope (23.62 ± 8.12 vs 27.63 ± 7.44, p < 0.05) and CSVA (1.44 ± 1.10 vs 2.07 ± 1.39, p < 0.05); significantly decreased PCL (31.52 ± 6.48 vs 29.41 ± 5.49, p < 0.05), OC (26.06 ± 11.13 vs 17.21 ± 9.00, p < 0.01) were shown postoperatively. In ACCF group, significantly increased CL (19.99 ± 12.71 vs 22.97 ± 11.36, p < 0.05) and C7 slope (24.59 ± 5.70 vs 30.62 ± 7.17, p < 0.05). In LTF group, significantly decreased PCL (35.37 ± 6.37 vs 32.00 ± 6.22, p < 0.01) and OC (30.71 ± 12.03 vs 23.12 ± 8.67, p < 0.01) were shown postoperatively.
Comparative study of sagittal parameters between preoperative and postoperative in different surgical groups.

ACDF, anterior cervical discectomy with fusion; ACCF, anterior cervical corpectomy with fusion; LTF, laminectomy with fusion; CL, cervical lordosis; PCL, C1-C2 cervical lordosis, proximal cervical lordosis; OC, occipito-C2 angle; EAM tilt, external auditory meatus tilt; CSVA, cervical sagittal vertical axis.
* Compare with preoperative values of the same group, significantly different, p < 0.05.
** Compare with preoperative values of the same group, significantly different, p < 0.01.
Comparative study of sagittal parameters in different surgical groups
Tables 4 and 5 summarized the comparative analyses of sagittal parameters in different surgical groups. No significant differences were shown in the preoperative measurements between ACDF and ACCF groups. Compared with ACDF group, LTF group showed significantly lower CL (16.80 ± 9.47 vs 13.90 ± 9.60, p < 0.05) and PCL (31.52 ± 6.48 vs 24.66 ± 6.92, p < 0.05); significantly higher CSVA (1.51 ± 1.13 vs 2.15 ± 1.29, p < 0.05) in the preoperative measurements. Compared with ACCF group, LTF group showed significantly lower CL (19.99 ± 12.71 vs 13.90 ± 9.60, p < 0.05) and PCL (30.80 ± 6.73 vs 24.66 ± 6.92, p < 0.05) in the preoperative measurements.
Comparative study of sagittal parameters in different surgical groups.
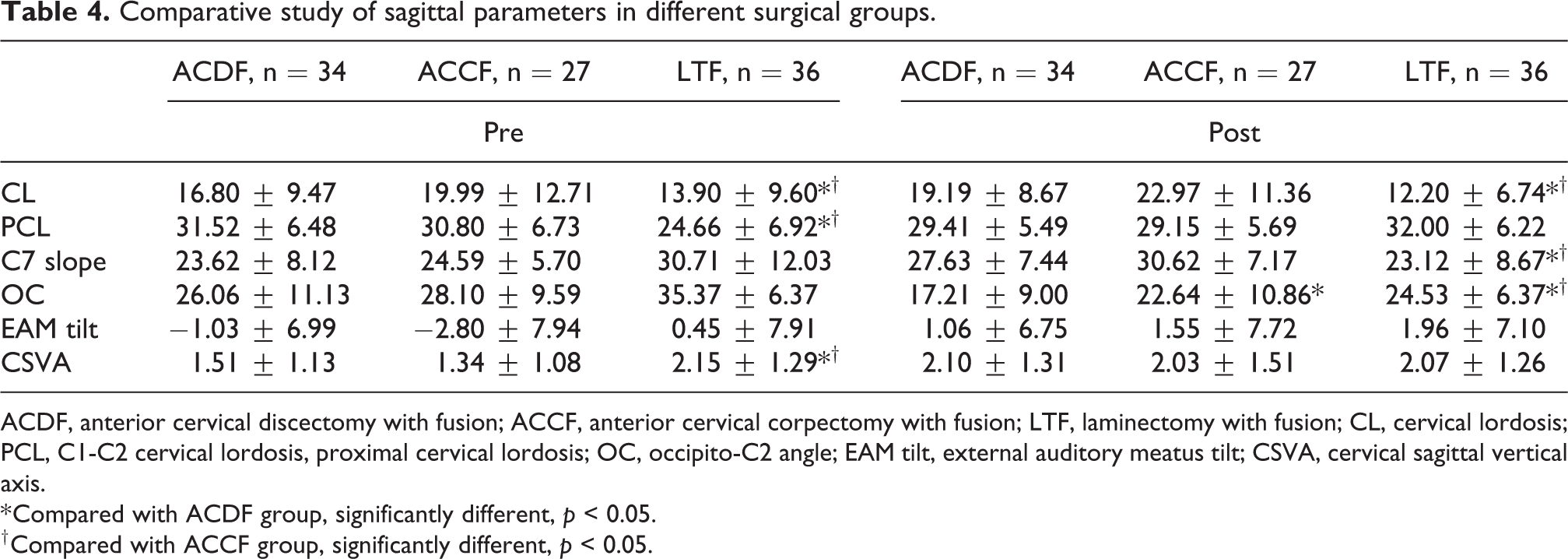
ACDF, anterior cervical discectomy with fusion; ACCF, anterior cervical corpectomy with fusion; LTF, laminectomy with fusion; CL, cervical lordosis; PCL, C1-C2 cervical lordosis, proximal cervical lordosis; OC, occipito-C2 angle; EAM tilt, external auditory meatus tilt; CSVA, cervical sagittal vertical axis.
* Compared with ACDF group, significantly different, p < 0.05.
† Compared with ACCF group, significantly different, p < 0.05.
Comparative study of sagittal parameters improvement in different surgical groups.

ACDF, anterior cervical discectomy with fusion; ACCF, anterior cervical corpectomy with fusion; LTF, laminectomy with fusion; CL, cervical lordosis; PCL, C1-C2 cervical lordosis, proximal cervical lordosis; OC, occipito-C2 angle; EAM tilt, external auditory meatus tilt; CSVA, cervical sagittal vertical axis.
* Compared with ACDF group, significantly different, p < 0.05.
† Compared with ACCF group, significantly different, p < 0.05.
Compared with ACDF group, ACCF group showed significantly higher OC (17.21 ± 9.00 vs 22.64 ± 10.86, p < 0.05) in the postoperative measurement. LTF group showed significantly lower CL (19.19 ± 8.67 vs 12.20 ± 6.74, p < 0.05) and C7 slope (27.63 ± 7.44 vs 23.12 ± 8.67, p < 0.05); significantly higher OC (17.21 ± 9.00 vs 24.53 ± 6.37, p < 0.05) in the postoperative measurement. Compared with ACCF group, LTF group showed significantly lower CL (22.97 ± 11.36 vs 12.20 ± 6.74, p < 0.05) and C7 slope (30.62 ± 7.17 vs 23.12 ± 8.67, p < 0.05); significantly higher OC (22.64 ± 10.86 vs 24.53 ± 6.37, p < 0.05) in the postoperative measurement.
No significant differences were shown in the sagittal alignment improvement between ACDF and ACCF groups. Compared with ACDF group, LTF group showed poor variance in △CL (2.32 ± 7.35 vs −1.70 ± 7.95, p < 0.05), △C7 slope (3.89 ± 7.93 vs −0.13 ± 6.70, p < 0.05) and △CSVA (0.57 ± 1.23 vs −0.08 ± 1.12, p < 0.05). Compared with ACCF group, LTF group showed poor variance in △CL (2.99 ± 9.29 vs −1.70 ± 7.95, p < 0.05), △C7 slope (6.03 ± 6.02 vs −0.13 ± 6.70, p < 0.05) and △CSVA (0.69 ± 1.42 vs −0.08 ± 1.12, p < 0.05).
Correlative studies between variance in HRQOL and sagittal parameters in different surgical groups
Tables 6 to 8 summarized the correlative analyses between variance in HRQOL and sagittal parameters in different surgical groups. In ACDF group, close correlations were obtained between △JOA and △C7 slope (r = −0.430, p < 0.05); △JOA and △CSVA (r = −0.567, p < 0.01); △NDI and △C7 slope (r = 0.410, p < 0.05); △NDI and △EAM tilt (r = 0.507, p < 0.01); △NDI and △CSVA (r = 0.675, p < 0.01); △VAS and △C7 slope (r = 0.374, p < 0.05); △VAS and △EAM tilt (r = 0.458, p < 0.01); △VAS and △CSVA (r = 0.584, p < 0.01).
Correlative studies between variance in HRQOL and sagittal parameters in ACDF group.

CL, cervical lordosis; PCL, C1-C2 cervical lordosis, proximal cervical lordosis; OC, occipito-C2 angle; EAM tilt, external auditory meatus tilt; CSVA, cervical sagittal vertical axis; JOA, Japanese orthopedic association; NDI, neck disability index; VAS, visual analog pain scale.
* Statistically significant, p < 0.05.
** Statistically significant, p < 0.01.
Correlative studies between variance in HRQOL and sagittal parameters in ACCF group.

CL, cervical lordosis; PCL, C1-C2 cervical lordosis, proximal cervical lordosis; OC, occipito-C2 angle; EAM tilt, external auditory meatus tilt; CSVA, cervical sagittal vertical axis; JOA, Japanese orthopedic association; NDI, neck disability index; VAS, visual analog pain scale.
Correlative studies between variance in HRQOL and sagittal parameters in LTF group.

CL, cervical lordosis; PCL, C1-C2 cervical lordosis, proximal cervical lordosis; OC, occipito-C2 angle; EAM tilt, external auditory meatus tilt; CSVA, cervical sagittal vertical axis; JOA, Japanese orthopedic association; NDI, neck disability index; VAS, visual analog pain scale.
* Statistically significant, p < 0.05.
** Statistically significant, p < 0.01.
In ACCF group, there is no correlation between HRQOL and sagittal parameters.
In LTF group, close correlations were obtained between △NDI and △CL (r = −0.291, p < 0.05); △NDI and △EAM tilt (r = 0.487, p < 0.01); △NDI and △CSVA (r = 0.394, p < 0.01); △VAS and △CL (r = −0.343, p < 0.05); △VAS and △EAM tilt (r = 0.443, p < 0.01); △VAS and △CSVA (r = 0.480, p < 0.01).
Discussion
Sagittal balance is one of the most important factors that affect the quality of life in patients with spinal diseases. 9,23 Previous studies are mainly focus on the effect of thoracolumber segments and pelvis alignments on HRQOL. Recently, cervical alignment has also been considered to play an important role to HRQOL in human. Several sagittal parameters have been used to evaluate the cervical sagittal alignment. When local segment alignment of cervical spine is changed, such as reduction of CL, increasing of CSVA and EAM tilt. At this time, the cervical spine will produce a series of compensatory mechanism, and a series of CSM related symptoms. Obeid et al. demonstrated that CL is the most important parameters to evaluate sagittal alignment of cervical alignment. 22 Lower CL was found in CSM patients and was the major cause of the symptoms of the CSM. Other studies reported that CSVA not exceeding 20 mm normally and increasing CSVA was considered as an important reason to poor HRQOL in CSM patients. 14 Thus, beside neurological decompression, correction of sagittal alignment is also considered an important goal of surgery. However, which surgical approach for CSM provides better postoperative cervical alignment is so far unclear.
Recently, many studies focus on the effect of surgical approaches on cervical sagittal alignment. Uchida et al. made analysis of a series of cases to compare with neurological functions and clinical efficacy obtained from the 3 years follow-up of anterior and posterior surgery. The results showed that the cervical curvature was significantly improved postoperatively in mCSM patients who undergone anterior surgery, in contrast, the cervical curvature was still poor in mCSM patients who undergone posterior surgery. 24 Shamji et al. analyzed the clinical outcomes in 124 CSM patients base on the cervical sagittal cobb angle and found that patients with kyphotic alignment exhibited greater improvement when approached by anterior approach. 25 More recently, CSVA has also been considered an important role in clinical. Tang et al. analyzed MCSM patients that underwent posterior cervical fusion for cervical stenosis, kyphosis or myelopathy and found 40 mm was the threshold of disability correlated the strongest with CSVA. 13
In this current study, we retrospectively analyzed the cervical alignment of mCSM patients and found that C7 slope, OC, EAM tilt and CSVA are the most important sagittal parameters correlated to the clinical outcomes. Cervical lordosis was improved in mCSM patients who undergone ACDF or ACCF. However, the cervical lordosis was still lower in mCSM patients who undergone LTF. Guo et al. also reported cervical curvature were significantly improved in patients with ACCF and ACDF compared with patients with LT. 26
Cervical Lordosis reduction produced a serious of compensatory mechanism in cervical alignment. To maintain the horizontal gaze under the lower CL situation, PCL and OC were found to increase and C7 slope were decreased, which kept a hyperextended posture to support the head. This compensatory mechanism would increase the load of the cervical spine muscles and resulted in a serious of symptoms. Previous studies suggested that surgeon should focus on restoring OC angle during occiptiocervical arthrodesis to maintain the horizontal gaze. 22 Our results also indicated that OC and PC was increased in mCSM patients due to the decreasing of cervical curvature and to maintain the horizontal gaze. Both PC and OC angle were improved postoperatively in MCSM patients with ACDF, ACCF and LTF. It is worth noting that PC and OC angle were improved in mCSM patients with ACDF, ACCF and LTF, C7 slope was still lower to maintain horizontal gaze due to the lower CL in mCSM patients with LTF. Hirai et al. demonstrated that C7 slope was decreased to maintain the sagittal balance and horizontal gaze when OC angle was increased postoperatively in spinal deformity patients. 27 Patients with ACDF has better clinical outcomes compare with patients with LTF due to the better improvement of CL, C7 slope, OC and CSVA. Thus, it is suggested that ACDF and ACCF provided better restoring of sagittal alignment than LTF.
There are some limitations in our study. First of all, it was a retrospective non-randomized case-control study and the number of patients in this study was relatively small. In addition, the follow-up data was lacking in this study to further evaluate the efficacy of surgery for treatment of mCSM. Further large-scale prospective trials with long-term follow-up periods are needed.
Conclusion
In mCSM patients, C7 slope, OC, EAM tilt and CSVA are the most important cervical sagittal parameters correlated to clinical outcomes; ACDF and ACCF provides more efficiency for restoration of cervical sagittal alignment.
Footnotes
Author contributions
Hui Liu and Zhaomin Zheng: Conceptualization, methodology, software. Jianru Wang, Zemin Li and Hua Wang: Data curation, writing—original draft preparation. Zihao Li: Visualization, investigation. Hui Liu: Supervision. Siwen Chen: Software, validation. Hui Liu and Xiang Li: Writing—reviewing and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.