
Abstract
Purpose:
In this study we investigated on the personal protective equipment (PPE) usage, recycling, and disposal among spine surgeons in the Asia Pacific region.
Methods:
A cross-sectional survey was carried out among spine surgeons in Asia Pacific. The questionnaires were focused on the usage, recycling and disposal of PPE.
Results:
Two hundred and twenty-two surgeons from 19 countries participated in the survey. When we sub-analysed the differences between countries, the provision of adequate PPE by hospitals ranged from 37.5% to 100%. The usage of PPE was generally high. The most used PPE were surgical face masks (88.7%), followed by surgical caps (88.3%), gowns (85.6%), sterile gloves (83.3%) and face shields (82.0%). The least used PPE were powered air-purifying respirators (PAPR) (23.0%) and shoes/boots (45.0%). The commonly used PPE for surgeries involving COVID-19 positive patients were N95 masks (74.8%), sterile gloves (73.0%), gowns (72.1%), surgical caps (71.6%), face shields (64.4%), goggles (64.0%), shoe covers (58.6%), plastic aprons (45.9%), shoes/boots (45.9%), surgical face masks (36.5%) and PAPRs (21.2%). Most PPE were not recycled. Biohazard bins were the preferred method of disposal for all types of PPE items compared to general waste.
Conclusions:
The usage of PPE was generally high among most countries especially for surgeries involving COVID-19 positive patients except for Myanmar and Nepal. Overall, the most used PPE were surgical face masks. For surgeries involving COVID-19 positive patients, the most used PPE were N95 masks. Most PPE were not recycled. Biohazard bins were the preferred method of disposal for all types of PPE.
Keywords
Introduction
COVID-19 pandemic has significantly affected the world. 1 It is an infectious disease caused by the SARS-CoV-2 virus whereby the mode of transmission is by contact or respiratory droplets. 2 The virus can transmit by close contact through respiratory droplets, by direct contact with the infected person, or by contact with contaminated objects and surfaces. Therefore, there is a need for personal protective equipment (PPE) among the healthcare workers who are at a higher risk of contracting this virus. It had been reported that the transmission risks were higher if PPE were unavailable or if the healthcare workers were not trained to handle these PPE. 3,4
PPE can provide a barrier to prevent the spread of infection to healthcare workers. 5 –9 The World Health Organization had formed a guideline to optimize the usage of PPE in order to increase the efficiency of PPE usage and to prevent its shortages. 10 These strategies can be adopted by healthcare workers so that appropriate PPE will be used in different clinical situations. Despite this, shortages of PPE still occur due to the increase in demand that was not matched by the current supply. 11,12 Therefore, other ways to curb this shortage of PPE such as extending or recycling its use were explored. 11,13 In addition, proper disposal of PPE is important to minimize the risk of transmission of this disease especially when handling biohazard or biomedical waste.
In this study we investigated on the PPE usage, recycling, and disposal among spine surgeons in the Asia Pacific region. We hope that this study can provide useful information to guide future management, usage, recycling, and disposal of PPE.
Methodology
This cross-sectional survey was carried out among spine surgeons in the Asia Pacific region from 4 May 2020 to 4 June 2020. The questionnaire was administered using REDCap (Vanderbilt, Nashville, TN, USA). The questionnaire was distributed by email and the respondents’ participation was voluntary.
Questionnaire
The first part of the online questionnaire were questions on the surgeon’s demographics and background. The second part of the online questionnaire were questions on PPE which explored whether these PPE were provided by the hospital or were purchased by the surgeons themselves. Common PPE listed were surgical face masks, N95 respirator masks, powered air-purifying respirators (PAPR), goggles, face shields, surgical caps, non-sterile gloves, sterile gloves, plastic aprons, gowns, shoe covers, and shoes/boots. We also asked whether these PPE were used in the clinics, wards, or surgery. If PPE were used, we asked what types of PPE were used. For surgery, we further subdivided the usage on whether the patient was COVID-19 positive (+ve) or negative (−ve). If the surgeon were not treating COVID-19 positive patients, we asked respondents what PPE they would be using if they were to treat COVID-19 positive patients. In addition, we also asked whether they would recycle these PPE and how would they recycle them. Recycling methods listed were sun exposure, washing with water, wash with spirit, wash with Clorox and sending it to factory or commercial recycling. Finally, we asked regarding the disposal of PPE, whether it was disposed into general waste or biohazard bins.
Statistical analysis
The data generated from the study was analysed using IBM SPSS ver. 26.0 (IBM Corp, Armonk, NY, USA). The distribution of categorical data was reported in numbers and percentages. Comparison between categorical data was performed using chi-square test. Fisher’s exact test was used when the value within the parameter was less than 5. Statistical significance was set at p value < 0.05.
Results
Survey respondents
The survey was sent to all members of the Asia Pacific Spine Society and selected non-members. A total of 719 survey email links were sent to 490 Asia Pacific Spine Society members and 229 selected non-members (Table 1). The selected non-members were surgeons who had participated in previous APSS activities (such as conferences, courses and fellowships) and were still enrolled in the APSS email subscription. A total of 222 surgeons from 19 countries participated in the survey. The total participation rate was 30.9%. The mean age (years old) of the respondents was 45.1 ± 9.0. There were 215 (96.8%) male and 7 (3.2%) female surgeons. The mean spine surgery experience (years) was 13.1 ± 14.7. There were 95 (42.8%) respondents that performed spine surgeries only, 119 (53.6%) respondents that performed orthopaedic and spine surgeries and 8 (3.6%) respondents that performed neurosurgery and spine surgery. There were 86 (38.9%) respondents from university only, 53 (24.0%) from government only, 63 (28.5%) from private practice only, 3 (1.4%) from both university and government, 5 (2.3%) from both government and private, 4 (1.8%) from university and private and 7 (3.2%) from university, government and private. There were 78 (35.3%) from individual practice, 140 (63.3%) from group practice and 3 (1.4%) from both individual and group practice. The distributions of the number of surgeons according to their countries are illustrated in Table 1. The highest number of respondents were from Japan (46, 20.7%). This was followed by Malaysia (38, 17.1%), India (27, 12.2%), Philippines (25, 11.3%) and South Korea (17, 7.7%).
Number and percentage of respondents by countries.
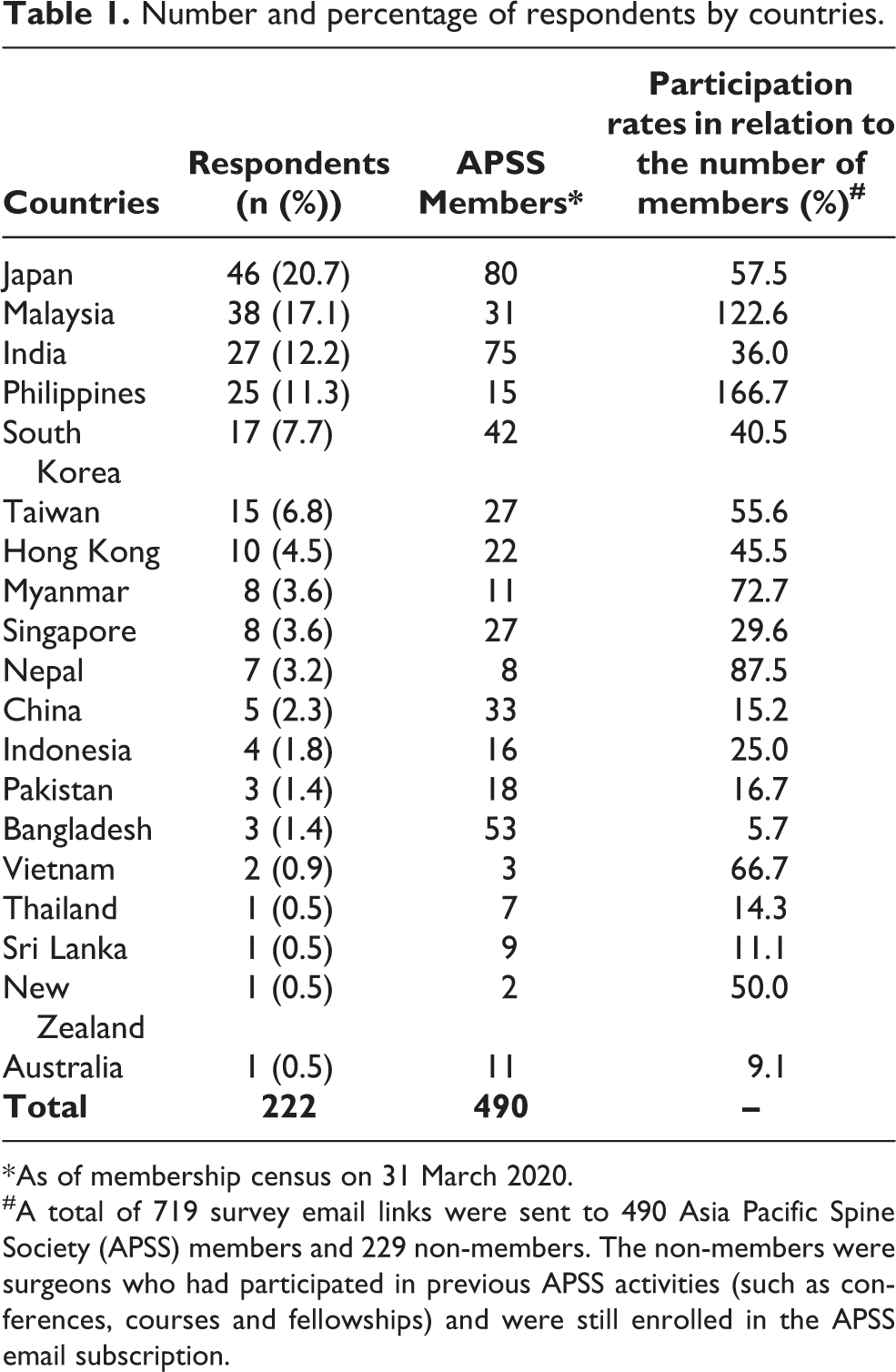
* As of membership census on 31 March 2020.
#A total of 719 survey email links were sent to 490 Asia Pacific Spine Society (APSS) members and 229 non-members. The non-members were surgeons who had participated in previous APSS activities (such as conferences, courses and fellowships) and were still enrolled in the APSS email subscription.
The provision of adequate PPE by hospital between countries
The provision of PPE by hospitals ranged between 37.5% and 100%, when we sub-analysed the differences between countries with more than five respondents. Singapore and Nepal (100%) had the highest provision, followed by Malaysia (97.4%) and Taiwan (93.3%). Myanmar (37.5%) had the lowest provision, followed by Japan (45.3%) and India (59.3%) (Figure 1).
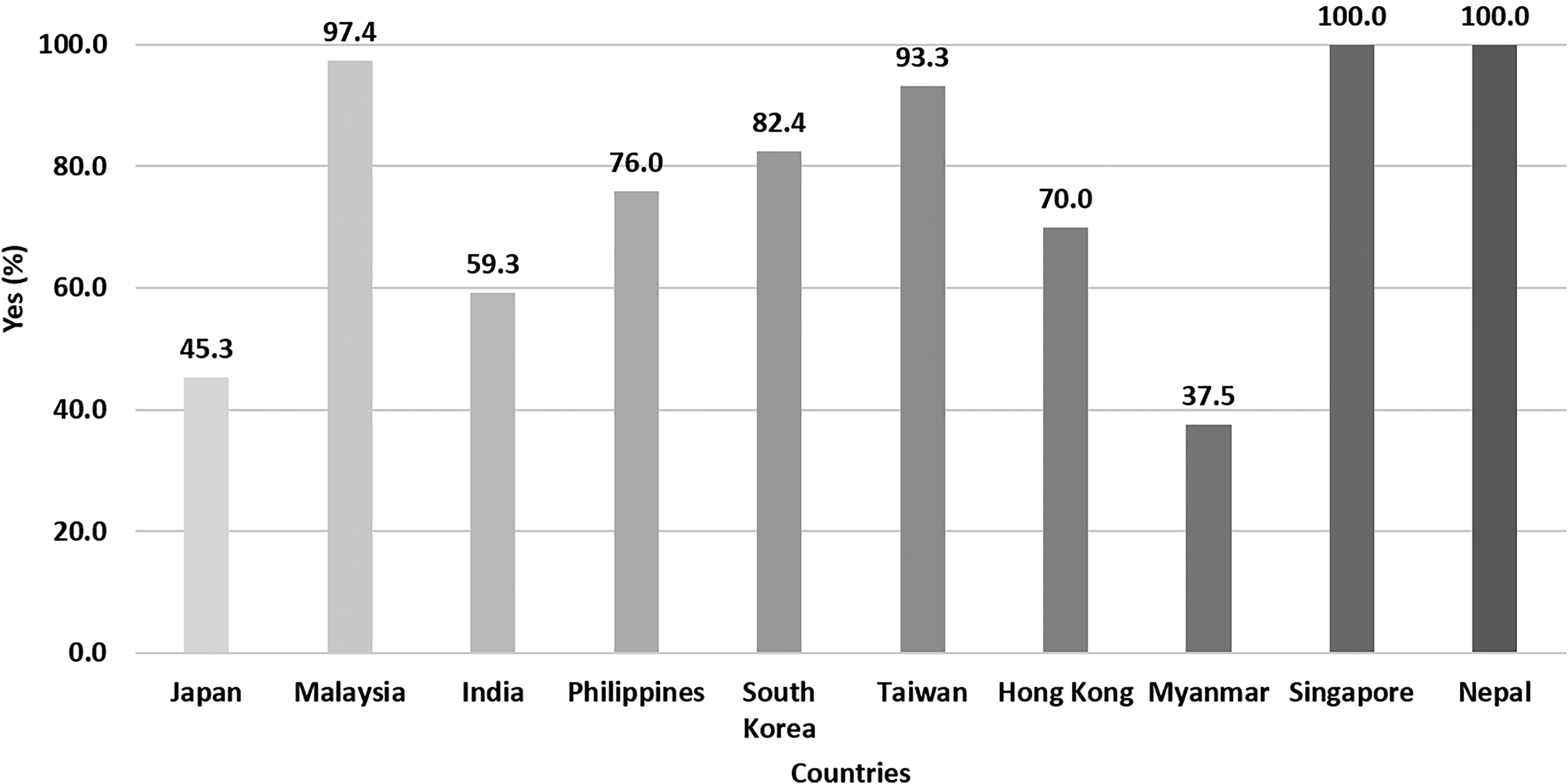
Provision of adequate personal protective equipment (PPE) by hospital during COVID-19 outbreak stratified by countries (only countries with more than five responses were analysed).
The usage of PPE between countries
The usage of PPE was generally high when we sub-analysed the differences between countries with more than five respondents. Singapore had 100% usage for clinics, wards, and surgeries for COVID-19 positive patients and 88% for surgeries for COVID-19 negative patients. Myanmar had low PPE usage in clinics (13%), wards (25%), and surgeries for COVID-19 negative patients (13%) whereas Nepal had low PPE usage in wards (14%), and surgeries for COVID-19 negative patients (29%). All countries had very high usage of PPE for COVID-19 positive surgeries (71–100%) except for Nepal (57%) (Figure 2).

The usage of personal protective equipment (PPE) in clinics, wards and operation theatres for surgeries involving COVID-19 negative patients and COVID-19 positive patients stratified by countries.
The usage of PPE among spine surgeons
The most used PPE were surgical face masks (88.7%), followed by surgical caps (88.3%), gowns (85.6%), sterile gloves (83.3%) and face shields (82.0%). The least used PPE were PAPRs (23.0%) and shoes/boots (45.0%). About 3.6–23.4% of surgeons needed to purchase these PPE for personal use with N95 being the most common item purchased (23.4%).
The commonly used PPE in clinics were surgical face masks (55.4%), non-sterile gloves (26.1%) and face shields (22.1%). The commonly used PPE in wards were surgical face masks (57.2%), N95 masks (21.6%), and non-sterile gloves (21.6%). The commonly used PPE for surgeries involving COVID-19 negative patients were surgical face masks (37.8%), sterile gloves (34.2%), gowns (33.8%), surgical caps (32.0%), face shields (24.8%), goggles (23.9%) and N95 masks (23.4%). The commonly used PPE for surgeries involving COVID-19 positive patients were N95 masks (74.8%), sterile gloves (73.0%), gowns (72.1%), surgical caps (71.6%), face shields (64.4%), goggles (64.0%), shoe covers (58.6%), plastic aprons (45.9%), shoes/boots (45.9%), surgical face masks (36.5%) and PAPRs (21.2%). Surgeons who performed or would perform surgeries on COVID-19 positive patients used significantly higher (p < 0.05) number of PPE except for surgical face masks and non-sterile gloves. Overall, the surgical face mask was the most common PPE used in clinics, wards and for surgeries involving non-COVID-19 patients. N95 mask was the most common PPE for surgeries involving COVID-19 patients. Certain items may be mutually exclusive (for example face mask, N95 mask, PAPR and face shield or non-sterile and sterile gloves) whereby the usage of one PPE will replace the usage of the other PPE (Table 2).
Personal protective equipment (PPE) usage in clinics, wards and operation theatres for surgeries involving COVID-19 negative patients and COVID-19 positive patients.

PPE: Personal Protective Equipment; PAPR: Powered air-purifying respirator; NA: Not applicable.
* Significant.
The recycling practices of PPE among spine surgeons
Most PPE were generally not recycled. Majority of PPE used in various locations in clinics, wards and operation theatres had only less than 20% PPE recycled with more than half had less than 5% PPE recycled. About 35% of goggles were recycled to be used after surgery for COVID-19 positive patients, 26% of non-sterile gloves were recycled in clinics, 22% of face shields were recycled in clinics and 21% of shoes/boots were recycled after surgery for COVID-19 positive patients (Figure 3).

The percentage of various types of personal protective equipment (PPE) recycled for future usage in clinics, wards and operation theatres for surgeries involving COVID-19 negative patients and COVID-19 positive patients.
N95 masks were recycled by sun exposure after usage in clinics (35%) and wards (33%). Shoes/boots were recycled by sun exposure after usage in clinics (33%) and by washing with Clorox after usage in clinics (33%) and after surgery for COVID-19 positive patients (25%). Goggles were recycled by washing with spirit after usage in clinic (22%) and by washing with Clorox after usage in ward (21%). Face shields were recycled by washing with Clorox (22%) and washing with spirit (20%) after usage in clinics (Figure 4 and Figure 5).

Various methods of personal protective equipment (PPE) recycling used in the clinics and wards.

Various methods of personal protective equipment (PPE) recycling used in the operation theatres for surgeries involving COVID-19 negative and COVID-19 positive patients.
The disposal of PPE among spine surgeons
The most common item disposed into general waste was surgical face masks (clinics: 24.8%, wards: 23.9%, surgeries non-COVID-19 patients: 13.1% and surgeries COVID-19 patients: 13.1%). The most common items disposed into biohazard bins were surgical face masks (clinics: 36.9%, wards: 35.1% and surgeries non-COVID-19 patients: 28.4%) and N95 masks (surgeries COVID-19 patients: 67.6%). Biohazard bins were significantly (p < 0.05) preferred as the method of disposal for all types of PPE items compared to general waste. More PPE were disposed into the biohazard bins for COVID-19 positive surgeries (34.2–67.6%) when compared to clinics (15.8–36.9%), wards (12.6–35.1%) and COVID-19 negative surgeries (12.6–28.4%) (Table 3).
Personal protective equipment (PPE) disposal methods in the clinics, wards and operation theatres for surgeries involving COVID-19 negative patients and COVID-19 positive patients.
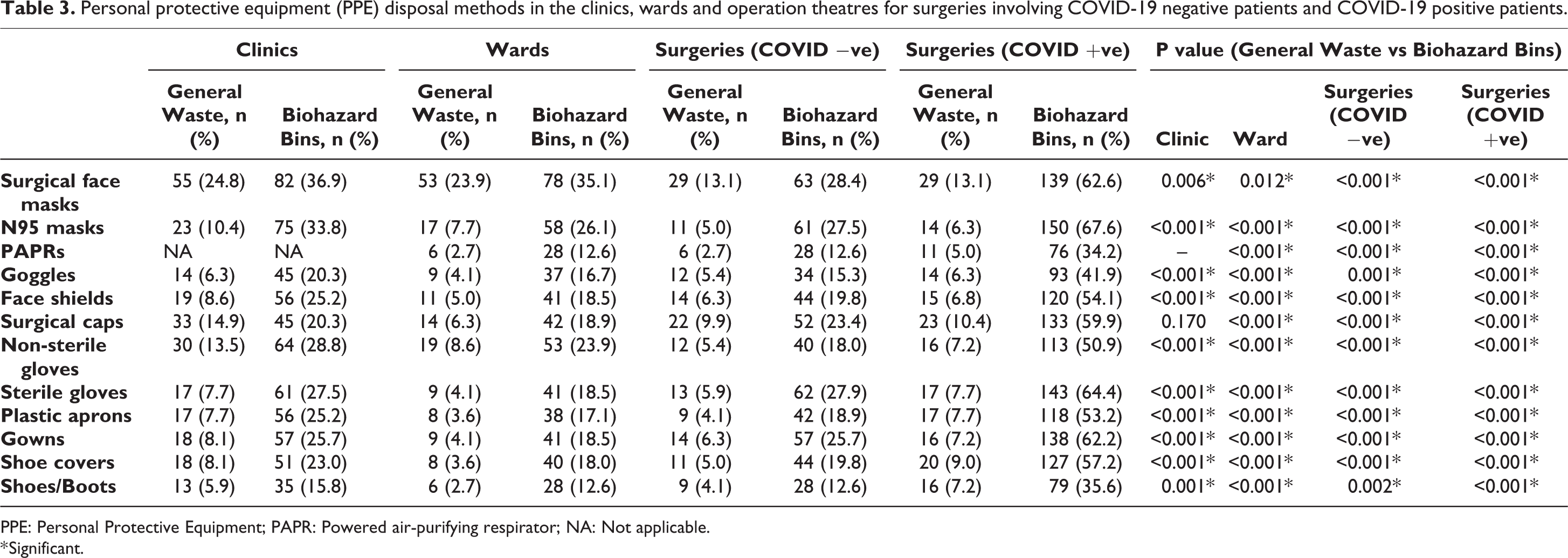
PPE: Personal Protective Equipment; PAPR: Powered air-purifying respirator; NA: Not applicable.
* Significant.
Discussion
Healthcare workers were exposed to a higher risk of COVID-19 infections. It had been reported that their risk factors were higher if they worked in high-risk departments (departments with interventional medical or surgical procedures that generate respiratory aerosols, including the respiratory department, infection department, ICU and surgical department), had longer duty hours, had severe fatigue, did not practice optimal hand hygiene, and were not trained to handle PPE or not using proper PPE. 3,4,14 This has impacted the mental health and psychological wellbeing of healthcare workers who are still required to continue their clinical work during this outbreak. 15 –17 The provision and usage of PPE can provide protection to prevent the transmission of disease to healthcare workers. 5 –9 However, amidst the surge of this pandemic, due to shortages of PPE, countries such as Italy had experienced high number of deaths among their healthcare workers. 12 Similarly in China, the lack of preparedness, understanding and the usage of PPE, up until 24 February 2020, contributed to more than 2000 healthcare workers infected with COVID-19 with 22 deaths. 4
With the lack of PPE, an increased transmission of COVID-19 to Orthopaedic surgeons also had been reported. 3 This has triggered the need for increased supply and sustainability of PPE, and as such, early work on extending the use of PPE and possibly recycling the PPE had begun. 13 Recently, the United States government had responded on the shortage of N95 mask by lifting the Food and Drug Administration (FDA) standards, stating that non-FDA approved N95 masks which were approved by the National Institute for Occupational Safety and Health could be used by healthcare workers. 12 Healthcare workers were urged to adopt guidelines formed by The World Health Organization on the usage of PPE in order to prevent shortages. 10 Therefore, the usage, recycling and disposal of PPE is currently very important globally as we face the threat of this pandemic.
Our study found that the usage of PPE was generally high among all countries especially for surgeries involving COVID-19 positive patients (Figure 2). Certain countries had usage as high as 100% and majority had usages more than 70%. This was expected as healthcare workers were frontliners during this pandemic and were exposed to a higher risk of contracting this illness. PPE were used as protection to prevent transmission of diseases. However, a few countries such as Myanmar and Nepal had low usages of PPE (less than 30%) in clinics, wards and/or surgery for COVID-19 negative patients. This may be due to low number of COVID-19 cases or possibility of low supply of PPE. Overall, the commonly used PPE were surgical face masks, surgical caps, gowns, sterile gloves, and face shields (Table 2). For surgeries involving COVID-19 positive patients, there was significantly increased usage of all PPE except surgical face masks and non-sterile gloves. The commonly used PPE for surgeries involving COVID-19 positive patients were N95 masks, sterile gloves, gowns, surgical caps, face shields, goggles, shoe covers, plastic aprons and shoes/boots. Surgical face masks were the most common PPE used in clinics, wards and for surgeries involving COVID-19 negative patients. N95 masks were the most common PPE used for surgeries involving COVID-19 positive patients.
Our study found that the provision of adequate PPE by hospitals were variable among countries in the Asia Pacific region (Figure 1). This had led to some differences in the usage of PPE among various countries (Figure 2). Singapore had 100% usage for clinics, wards, and surgeries for COVID-19 positive patients and 88% for surgeries for COVID-19 negative patients. Myanmar had low PPE usage in clinics (13%), wards (25%), and surgeries for COVID-19 positive patients (13%) whereas Nepal had the least PPE usage in wards (14%), and surgeries for COVID-19 positive patients (29%). This could be due to the shortages in PPE supply among those countries with low PPE usage, especially when dealing with surgeries involving COVID-19 positive patients.
Current options of extending the usage of PPE and recycling have not been well established in literature. Dargaville et al. 13 had recommended the scientific community to embark on research and development to improve the sustainability of PPE by safely extending its usage and finding various methods to recycle them. In our study, most respondents had not recycled PPE to be used again (Figure 3). More than half of the respondents who used PPE, recycled less than 5% of the PPE used. For those who did, the PPE were mainly recycled by sun exposure, washing with Clorox, or washing with spirit (Figures 4 and 5).
Proper disposal of PPE may be an important factor to prevent disease transmission. Hallihan et al. 18 had performed a study on the issues in disposal of PPE and found that improper disposal of PPE was a risk factor for transmission of diseases to healthcare workers. In our study, we found that biohazard bins were significantly preferred as the method of disposal for all types of PPE items compared to general waste (Table 3). More PPEs were disposed into the biohazard bins after COVID-19 positives surgeries (34.2–67.6%) when compared to clinics (15.8–36.9%), wards (12.6–35.1%) and COVID-19 negatives surgeries (12.6–28.4%) (Table 3). Disposal of PPE into biohazard bins can reduce the risk of disease transmission when handling these wastes. However, the cost of biohazard or biomedical waste disposal can be considerably higher. 19,20 Moreover, PPE disposed as biohazard or biomedical waste cannot be recycled. Therefore, there is a need for future research on this issue focusing more specifically on when, what, and how PPE should be disposed as biomedical waste.
There were several limitations in this study. This survey had the participation of 222 surgeons only. Among the total of 19 countries, only 10 countries had more than five respondents (Table 1). The rest of the countries had five or less respondents and were excluded from analysis when we compared the result between countries. Due to this the overall results cannot be generalized to all countries in the Asia Pacific region. We were unable to calculate the actual participation rates for each country (Table 1) because this survey was anonymous, and we only have the data on the surgeons’ country of origin if they had participated in this survey. The next limitation was that the respondents were requested to provide their opinions on how they would use, recycle, and dispose PPE for surgeries done on COVID-19 positive patients even though they have not performed it before. This was an assumption on how they would handle PPE if they had treated patients with COVID-19. The method to confirm COVID-19 positive patients for every hospital/clinic for every respondent were not determined. We did not ask in our questionnaire regarding any hospitals mandating all used PPE to be disposed into biohazard bins. Another limitation was that this study was a survey in which the data acquired were opinions given by respondents and may lead to bias. However, we do not think that the bias will be significant as the questions were information from the respondent’s daily clinical practice and had no ordinal preferential opinion which is more subjected to bias.
Conclusions
The usage of PPE was generally high among most countries especially for surgeries involving COVID-19 positive patients except for Myanmar and Nepal. The provision of adequate PPE by hospital were variable among countries in the Asia Pacific region. Overall, the most used PPE were surgical face masks, followed by surgical caps, gowns, sterile gloves, and face shields. For surgeries involving COVID-19 positive patients, the most used PPE were N95 masks, followed by sterile gloves, gowns, surgical caps, face shields, goggles, shoe covers, plastic aprons, and shoes/boots. Most PPE were not recycled to be used again. Biohazard bins were the preferred method of disposal for all types of PPE.
Supplemental material
Supplemental Material, sj-pdf-1-osj-10.1177_2309499020988176 - Personal protective equipment usage, recycling and disposal among spine surgeons: An Asia Pacific Spine Society survey
Supplemental Material, sj-pdf-1-osj-10.1177_2309499020988176 for Personal protective equipment usage, recycling and disposal among spine surgeons: An Asia Pacific Spine Society survey by Chee Kidd Chiu, Chris Yin Wei Chan, Jason Pui Yin Cheung, Prudence Wing Hang Cheung, Siti Mariam Abd Gani and Mun Keong Kwan in Journal of Orthopaedic Surgery
Footnotes
Author contributions
CKC and CYWC contributed equally to this study and therefore share first authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.