
Abstract
The two main surgical options for patients with persistent or recurrent cubital tunnel syndrome are subcutaneous and submuscular transposition. We retrospectively analysed the results of 34 patients with recalcitrant cubital tunnel syndrome who underwent submuscular transposition with musculofascial lengthening at our institutions. Of the 34 patients, 21 improved clinically after submuscular transposition with musculofascial lengthening, of which 16 were still satisfied at a mean follow-up of four years. In addition, all articles published between 1974 and January 2015 on subcutaneous and/or submuscular transposition of the ulnar nerve for recalcitrant cubital tunnel syndrome were reviewed. We found that previously published studies on this subject are too heterogeneous to compare. No recommendation can thus be made regarding the surgical technique for persistent or recurrent cubital tunnel syndrome. Our series shows that the musculofascial lengthening technique for submuscular transposition is a good option. More research is needed to compare the different surgical treatments.
Keywords
Introduction
Symptoms of cubital tunnel syndrome (CuTS) frequently persist or recur after primary surgery, about 30% in the prospective randomized trial by Bartels et al. (2005). Revision surgery may therefore be needed in some of these cases. Several studies have investigated the effectiveness of subcutaneous (SCT) or submuscular transposition (SMT) for recalcitrant CuTS (Aleem et al., 2014; Bartels and Grotenhuis, 2004; Broudy et al., 1978; Davis and Bulluss, 2005; Gabel and Amadio, 1990; Goldfarb et al., 2009; Holmberg, 1991; Rogers et al., 1991; Sarris et al., 2002; Vogel et al., 2004). Nevertheless, there is still no consensus on what type of anterior transposition is best in patients with recurrent or persistent symptoms of CuTS. The choice of either SMT or SCT often depends on the preference and experience of the surgeon. A potential disadvantage of SMT is secondary compression due to shortening of the muscle after transection, but this can be overcome by the musculofascial- or Z-lengthening technique (Dellon and Coert, 2004). This technique significantly reduces the intraneural pressure compared to the Learmonth technique for SMT (Dellon et al., 1994).
In this study, we present our results for ulnar nerve revision surgery in 34 patients using SMT with musculofascial lengthening. We have also performed a literature search to try to answer the following PICO (population, intervention, comparison, outcome) question: ‘Which of the most widely used surgical techniques (SMT or SCT) gives the best relief of ulnar nerve-related symptoms in adult patients with recurrent or persistent symptoms of CuTS?’
Patients and methods
Patient population
Between January 2003 and January 2014, a total of 40 adult patients with recurrent or persistent CuTS were operated on in a university hospital and a large teaching hospital. Six patients were excluded from analysis: two who had previously had cervical spine surgery at the C6–C7 level (because of the double level lesion/compression); one with polyneuropathy of the upper extremities; two with a follow up of less than 12 months; and one who died during follow-up due to another cause. The final study group therefore consisted of 34 patients. All procedures were performed by two experienced peripheral nerve surgeons (J.H.C. and G.d.R.), with level 4 and 5 experience (Tang and Giddins, 2016). Both surgeons work in the two medical centres and evaluated the outcome pre- and postoperatively.
Patients with persistent or recurrent symptoms of CuTS met the indications for operation. Symptoms consisted of pain, tingling and/or progressive motor and/or sensory loss, after one or multiple previous procedures. Symptoms that were not relieved by the original surgery were classified as ‘persistent’, while those that recurred after original improvement were classified as ‘recurrent’. For recurrences, the interval from failure to revision surgery was calculated from the time the complaints had recurred. Although revision surgery was performed as early as three months after the first treatment, it was usually after a longer interval (between six months and one year).
Demographics of patients in the study including previous operations and investigations.
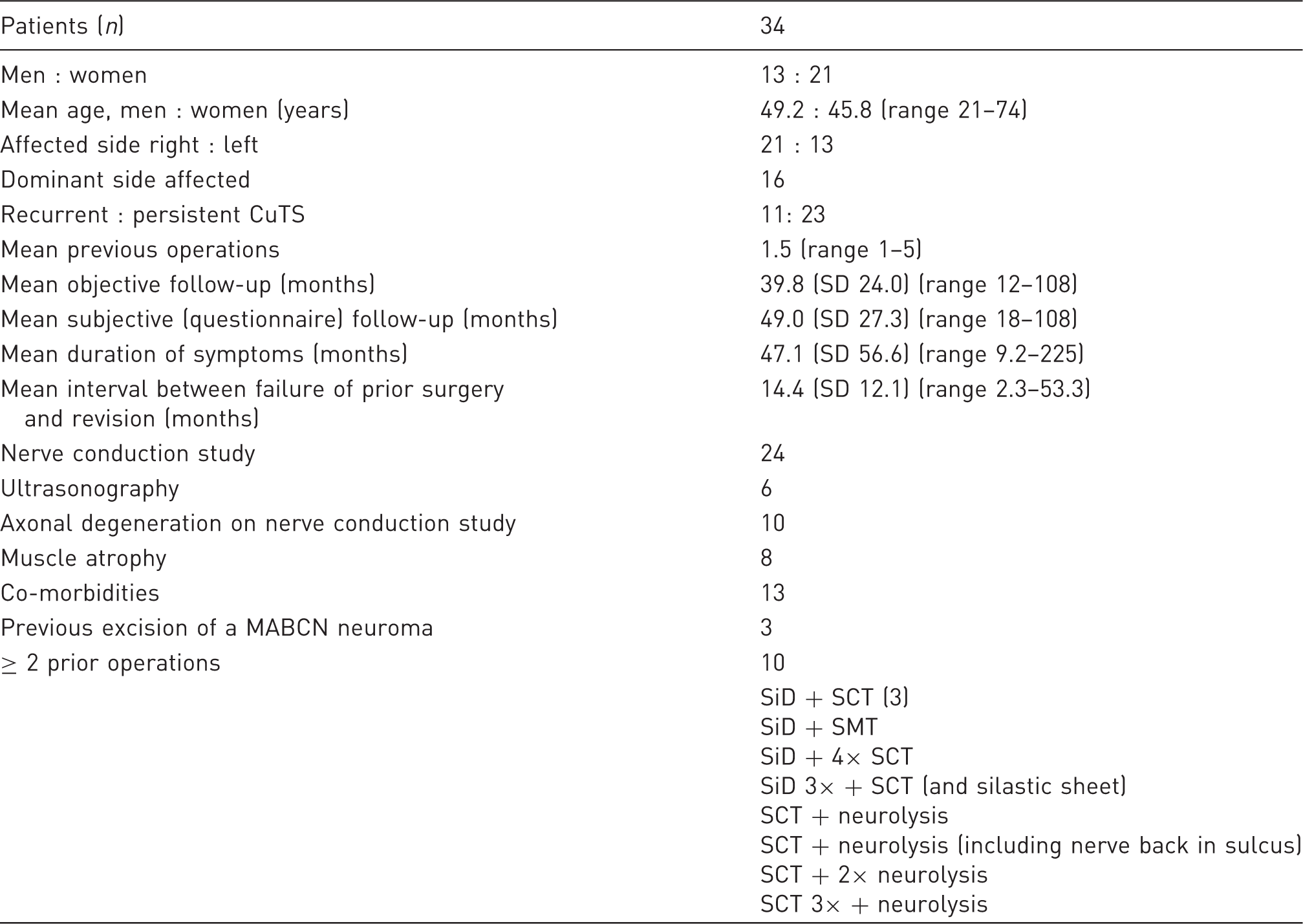
CuTS: cubital tunnel syndrome; MABCN: medial antebrachial cutaneous nerve; SCT: subcutaneous transposition; SD: standard deviation; SiD: simple decompression; SMT: submuscular transposition.
Surgical procedure and postoperative care
In all patients, submuscular transposition of the ulnar nerve with musculofascial lengthening, previously described by Dellon and Coert (2004), was performed. In short: a z-lengthening incision is made through the attachment of the flexor pronator mass to the medial epicondyle. After transposition of the ulnar nerve across the medial epicondyle, the longer part of the muscular mass is re-attached to the longer part of the tendon. This lengthening of the muscle creates extra submuscular space for the ulnar nerve and prevents secondary compression by the flexor pronator mass. In cases of failed Learmonth SMT, the flexor-pronator mass is transected in a step-cut lengthening fashion at the origin of both muscles. A v-shaped incision is also made in the intermuscular septum proximal to the medial epicondyle. The MABCN neuromas were surgically excised and subsequently buried in the triceps muscle without tension and secured with two or three nylon sutures to prevent displacement.
Postoperative care consisted of, first, one week of immobilization with the arm in 90° flexion, allowing minimal forearm pronation. Subsequently, the patients underwent two weeks of passive mobilization in a sling, followed by three weeks of active mobilisation without lifting objects weighing more than 1 kg.
Clinical outcome
Clinical outcome was assessed for resolution of tingling and recovery of sensation and motor weakness (intrinsic muscles of the affected hand, adductor pollicis and abductor digiti minimi muscles) recorded at the first follow-up or later times. Patients were scored as either ‘improved’, ‘unchanged’ or ‘worsened’. ‘Improved’ patients showed clear improvement after surgery in one or more clinical features. Sensibility was measured by touch and skin prick tests, and strength was scored with the MRC muscle grading system. Successful outcome was defined as complete or partial resolution of preoperative symptoms.
Subjective outcome
Long-term subjective outcome was assessed using a modification of the questionnaire introduced by Novak et al. (2002), which was sent to the patients at the time of this retrospective review in 2015 and 2016. The questionnaire provides information concerning pain, sensation, paraesthesia, strength, cold intolerance and the patient’s perception of outcome pre- and postoperatively.
Analysis of data
Pre- and postoperative symptom variables were assessed with the McNemar test. ANOVA was used for continuous variables and chi-squared test for categorical factors. A p-value < 0.05 was assumed to indicate significance.
Literature review
We conducted a search on PubMed, Embase and Cochrane libraries between January 1974 and January 2015 using synonyms for CuTS and SCT or SMT. Our search for titles and abstracts included: ‘(Cubital tunnel OR sulcus ulnaris OR ulnaropathy OR ulnar nerve OR ulnar neuritis AND (Submuscular OR subcutaneous OR transposition OR decompression OR transposing)’. One investigator independently conducted the database search, removing duplicates and screening all titles and abstracts for eligibility. Then the full text was reviewed. References of the final articles were screened and included if deemed relevant. Criteria for inclusion were randomized controlled trials or observational studies of intervention with the SCT or SMT technique for adult patients with recalcitrant CuTS, using clinical and/or subjective outcome measures.
Other characteristics including first author, study type, publication date, patients’ characteristics (age, sample size, surgical technique, follow-up, previous failed interventions, intraoperative findings, persistent versus recurrent cases) and outcome measurements were extracted from the studies. The primary outcome of the review was clinical or subjective improvement after revision surgery. Confidence intervals were calculated for the primary outcome, and subsequently, the data were pooled (if possible) whereby the weighted averages were calculated (Sum [study average × study cohort size 1,2… n/pooled cohort size]). All included articles were screened for risk of bias.
Results
The patient demographics are shown in Table 1.
Intraoperative findings
The following findings were predominantly present: dense scar tissue compressing the ulnar nerve at several levels near and at the cubital tunnel (n = 23); nerve hyperaemia (n = 9); ulnar nerve back in the sulcus after SCT (n = 2); incomplete releases after SCT, SMT and SD (n = 3); and, in case of revision after SCT, compression of the ulnar nerve at its new position (n = 5) and pathology of the posterior branch of the MABCN (n = 5). In five cases, there were no aberrant findings.
Clinical outcome
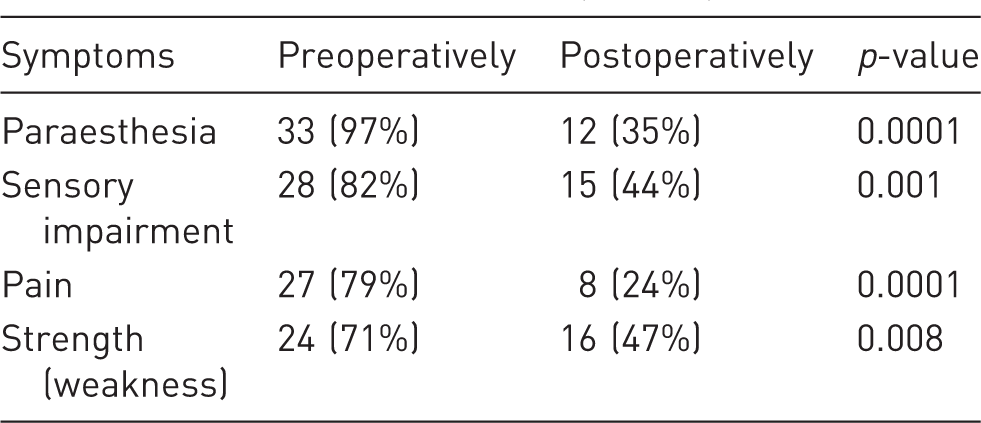
Cubital tunnel symptoms of patients before and after SMT with musculofascial lengthening.
Subjective outcome
One patient declined and therefore 33 patients completed the questionnaire, at a mean of 49 months after operation. Twenty patients improved after surgery, of whom eight were free of symptoms. These eight patients were all clinically scored as improved. Nine patients reported no benefit and four had got worse. Two of these four were clinically identified as worsened. The other two were clinically scored as unchanged or improved. Sixteen patients were satisfied, nine were partly satisfied and eight were not satisfied with the end result. Sensibility improved in 16, of whom ten felt sensation had returned to normal. Thirteen reported no change and four were worse. Postoperative strength improved in 15 patients, of whom six felt they had normal strength. Fourteen reported no benefit and four had deterioration in strength. Pain in the hand, paraesthesia and pain at the elbow showed a statistically significant improvement (p = 0.012; 0.0001; 0.0039).
Literature review
Out of a total of 729 articles retrieved, only ten retrospective studies (six SMT, one SCT and three mixed SCT/SMT) met our predetermined criteria (see Figure S1, flow diagram, online supplementary material). These studies solely focused their intervention on recurrent CuTS with the SCT or SMT technique (see Table S1, literature review, online supplementary material).
The overall objective successful outcome was in the range of 25–75% and 20–100% for SCT and SMT, respectively. Two studies also presented subjective outcome measures. The mean pooled overall improvement was 63% and 54% for SMT and SCT, respectively. Thus, SMT seems to have a slightly better outcome in symptom reduction. However, it is difficult to compare the results of the various studies because of differences in baseline characteristics, potential selection and performance bias (all retrospective studies), potential recall bias (subjective outcome studies) and a wide range of differences in outcome measures. Therefore, the pooled results do not provide a useful value.
Discussion
The results of our series of submuscular transposition with musculofascial lengthening show good results in patients with recalcitrant CuTS. Twenty-one of the 34 patients (62%) improved clinically after SMT, of which 25 (76%) were still (partly) satisfied with the long-term outcome (mean four years). This outcome is comparable with other previous published SMT studies, but comparison cannot be made due to a different SMT technique being used. Musculofascial lengthening of the flexor-pronator mass significantly reduces the intraneural pressure compared to the Learmonth technique for SMT (Dellon et al., 1994) and therefore could be superior to a ‘classic’ Learmonth SMT in recalcitrant cases. Only Vogel et al. (2004) have used the same technique and reported similar rates of 56% (10/18) good to excellent outcome with 78% patient satisfaction, although comparison is difficult because there were more incomplete releases (retained intermuscular septum, arcade of Struthers, common flexor aponeurosis), nerve instability cases and less prior interventions in their series.
It is difficult to compare our results to those for subcutaneous transposition, with only one study reporting results for that technique for recalcitrant CuTS (Caputo and Watson, 2000). In their study, residual compression was noted as the most frequent cause of failure, while this was only the case in three patients in our study. A potential explanation for this difference is the higher proportion of failed anterior transpositions (12 SCT and four SMT in 20 cases) in their series. In our study most patients had previously undergone a SiD. Our feeling is that the chance for success is higher for treatment of incomplete release than extensive scar tissue. In the other studies on SMT (Broudy et al. 1978; Gabel and Amadio, 1990; Rogers et al. 1991; Vogel et al., 2004), incomplete release was noted as the cause in more than 50% of the cases.
The publications on recalcitrant CuTS are quite heterogeneous. A wide range of different outcome measures and follow-up periods were found. Some reports have not defined which grading system was applied. Only the studies by Caputo and Watson (2000) and Gabel and Amadio (1990) have used the same grading system. Gabel and Amadio (1990) found satisfactory results after SMT in 83% and in 50% after SCT while Caputo and Watson (2000) found 75% after SCT. It should be noted that there were only three patients with muscle denervation in the study by Caputo and Watson (2000) in contrast to 15 patients in the study by Gabel and Amadio (1990). Denervation is a potentially negative prognostic factor (Bartels et al., 2005; Gabel and Amadio, 1990). Gabel and Amadio (1990) presented a better outcome for SMT than SCT, although the difference did not reach statistical significance (p = 0.12). Most studies have only looked at objective outcome measures. As Bartels and Grotenhuis (2004) have shown, there may be a discrepancy between the objective and subjective outcome after surgery. Patient satisfaction is probably the most important outcome, and therefore the result could be less favourable than suggested by these studies. Our study demonstrated almost similar objective and long-term subjective outcomes. More research is needed to further investigate potential differences between the two types of operation for recalcitrant CuTS, preferably in a prospective or randomized controlled manner and including patient reported outcome measures (MacDermid and Grewal, 2013), strength and sensibility measurements.
A drawback of the SMT is the relatively long period of restriction of mobilisation after operation. In our study, three elbow contractures were observed, of which two resolved over time. Gabel and Amadio (1990) documented ten elbow contractures that all returned to the preoperative level in six months. Although the risk of this complication is low, it should be discussed with the patient.
Limitations of our study include its retrospective design with potential recall bias and that two different surgeons carried out the surgery. However, both surgeons performed exactly the same procedure and have done a number of cases together to assure this.
In conclusion, this study shows that SMT with musculofascial lengthening is a good long-term surgical option for persistent or recurrent CuTS. There is no consensus in the literature about which surgical technique (SCT or SMT) is best for recalcitrant CuTS.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Board approval by the Medical Ethics Committee Erasmus Medical Center Rotterdam, the Netherlands. Number: MEC2014-128. Informed consent was obtained from all patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.