
Abstract
Purpose:
Constitutional varus in the coronal plane is formed based on the Hueter-Volkmann’s law. The varus deformity occurs at the proximal metaphysis of the tibia and the tibial condyle rotates medially. In the sagittal plane, we hypothesized that the posterior slope angle of the tibial articular surface may also occur at the proximal metaphysis and the tibial condyle rotates posteriorly. The purpose of this study was to verify the hypothesis.
Methods:
A total of 208 patients who underwent TKA had lateral view proximal tibia digital radiograph on which seven parameters were analyzed. The posterior slope angle of the tibial articular surface relative to the anterior wall of the tibial condyle and that relative to the anterior cortex of the tibial shaft were assessed. Correlation between the position of the tibial condyle and the posterior slope angle of the articular surface were assessed.
Results:
The proximal tibial condyle itself did not have a posterior slope in the 86.5% of the participants. Posterior rotation of the tibial condyle created posterior slope of the tibial articular surface relative to the anterior cortex of the tibial shaft. The more tibial condyle was posteriorly rotated, the more the tibial articular surface shifted posteriorly.
Conclusion:
Study findings showed that the posterior tibial slope occurs at the proximal metaphysis of the tibia, and the tibial condyle rotates posteriorly. The posterior tibial slope involves the posterior shift of the tibial articular surface. The posterior tibial slope is mainly created by the posterior rotation of the tibial condyle.
Introduction
It is a common knowledge that proximal tibiae have some degree of varus alignment that is called as the constitutional varus. 1 –3 Proximal tibia vara involves the medial shift of the articular surface. This is because the varus deformity occurs at the proximal metaphysis of the tibia and the tibial condyle rotates medially. 2 This proximal tibia vara in the coronal plane is based on the Hueter-Volkmann’s law. 1 According to this law, growth at the physes is retarded by increased compression, whereas reduced loading accelerates growth. In the sagittal plane, proximal tibiae have various posterior slope angles of the tibial articular surface (Figure 1). Our hypothesis stated that the tibial posterior slope could also be the consequence of the Hueter-Volkmann’s law, and the tibial condyle rotates posteriorly relative to the tibial shaft in the sagittal plane at the proximal metaphysis of the tibia. In this study, two angle parameters of the tibial posterior slope were assessed. The first tibial posterior slope angle is relative to the tibial condyle and the second is relative to the tibial shaft. To assess these two angles, three parameters and four distance parameters were established.

(a) and (b). A tibia without a posterior slope of the tibial articular surface (a) and a tibia with a larger posterior slope (b). The distances between the tibial tuberosity and the tibial articular surface and the distance between the tibial tuberosity and the femoral condyle are different between (a) and (b).
We had five hypotheses. Hypothesis 1 stated that the posterior slope of the tibial articular surface was formed by the posterior rotation of the tibial condyle at the proximal metaphysis based on the consequence of the Hueter-Volkmann’s law. Hypothesis 2 stated that the tibial posterior slope angle had correlations with the posterior shift of the tibial articular surface. Hypothesis 3 stated that the posterior slope of the tibial articular surface in the sagittal plane had correlation with the varus angle of the articular surface in the coronal plane. Hypothesis 4 stated that the posterior condyle hangover from the posterior cortex gradually becomes larger according to the posterior shift of the tibial articular surface. Hypothesis 5 stated that the posterior slope angle of the tibial articular surface had no correlation with age. In this study, by clarifying these hypotheses, we could prove that the tibial posterior slope is formed by the posterior rotation of the tibial condyle.
Materials and methods
The institutional review board approved this study protocol before the study begun. A retrospective review of all patients who underwent total knee arthroplasty (TKA) from January 2017 to December 2019 in our institute was performed. Of a total amount of 276 TKA cases, only cases with medial osteoarthritis were selected. The exclusion criteria were: cases with lateral osteoarthritis, or with patellofemoral arthritis, or with post trauma arthritis (these knees may probably have a malrotation of the tibia relative to the femur), cases with bone defect or with destruction of the articular surface, cases with osteophytes on the posterior condyles (the most exact posterior point could not be decided), cases that had undergone a second TKA, and cases with rheumatoid arthritis. Consequently, 68 cases were excluded with the above reasons; 208 cases were assessed in this study.
There were 162 females and 46 males. The mean age was 75.1 years old (range, 57 – 91 years). The mean height, weight, and BMI were 152.8 cm, 60.9 kg, and 26.0, respectively. The lateral view digital radiograph before TKA was used for this study (Figure 1). The x-ray beam was centered on the knee with the radiography tube at 100 cm. An 8 × 10-inch cassette 2 was placed immediately behind the participant, and the digital radiograph (Toshiba, Japan) was taken. A setting of 200 mA and a kilovoltage of 50 kV were used. For the true lateral view, radiographs with the distance between the most posterior points of the lateral and medial femoral posterior condyles of 2 mm or less were used for the measurements. The anteroposterior digital radiograph of the tibia was also taken before TKA according to the previous study. 2
The digital data of the radiograph was analyzed using the computer soft-ware (ShadeQuest/ViewR, Yokokawa Medical Solutions Corporation, Japan). The flexion angle between the femur and tibia was expressed using the anterior cortex of the shaft. The mean angle between the anterior cortex of the distal femoral shaft and the anterior cortex of the tibial shaft was 57.4° ± 12.1°. Six lines were drawn on the proximal tibia for angle parameters (Figure 2). Line 1 represented the anterior cortex of the tibial shaft. Line 2 represented the middle one-third of the medial articular surface. The medial articular surface has three slopes. The middle one-third area was used in this study.
4
Line 3 represented the anterior wall of the tibial condyle. Line 4 represented the posterior cortex of the tibial shaft. Line 5, drawn parallel to Line 2, represented the length of the tibial condyle so that the end of the line was the most posterior point of the condyle. Line 6 was the line perpendicular to Line 1. Three angle parameters were measured. Angle TS was the angle between Line 6 and Line 2. Angle TS represented the tibial articular slope angle relative to the anterior cortex of the tibial shaft. Two new angle parameters, Angle AW and Angle CS, were defined. Angle AW was the angle between Line 1 and Line 3. Angle AW represented the posterior tilting angle of the anterior wall of the tibial condyle relative to the anterior cortex of the tibial shaft. Angle CS was the angle between Line 2 and Line 3. Angle CS presented the tibial articular slope angle relative to the anterior wall of the tibial condyle. Angle TS and Angle AW were measured, and Angle CS was calculated using Angle TS and Angle AW. (a)–(c). Seven parameters on the lateral view of the proximal tibia. (a) A lateral view of the proximal tibia. (b) Six lines were drawn, and the midpoint of the tibial condyle was set. The midpoint was the center of Line 5. (c) Three angular and four distance parameters were measured.

With these angle parameters, the posterior slope angle of the articular surface relative to the tibial condyle and relative to the tibial shaft were assessed.
Four distance parameters were measured. Line 5 represented the length of the tibial condyle. Distance CO was the distance from L1 to the midpoint of Line 5 along Line 5. Then Distance AC was calculated using Distance CO and Angle TS

Distance AC represented the posterior shift distance of the midpoint of the tibial condyle from Line 1. Distance PC was the distance from Line 4 to the most posterior point of Line 5. Distance PC represented the tibial posterior condyle offset from the posterior cortex of the tibial shaft with the same concept of the femoral posterior condyle offset. 5 With these distance parameters, the effect of Angle TS on the position of the tibial articular surface relative to the anterior cortex of the tibial shaft was assessed.
On the anteroposterior view radiograph of the tibia, Angle SA that was the angle between the tibial plateau tangent and the line perpendicular to the anatomical axis of the tibia was measured with the same method as the previous study. 2,3
The lines and parameters used in this study were originated by the authors. Reliability of all parameters was assessed using the intraclass correlation coefficients. One of the authors measured all parameters three times and assessed the intra-observer reproducibility in 40 participants. Three of the authors measured all parameters independently and assessed the inter-observer reproducibility in 40 participants using the protocol of previous studies. 6 –8 The reproducibility method was blinded, and the readers performed all measurements without knowledge of prior results; all markings were erased for each reader. The intra-observer agreement of Angle TS, Angle AW, Distance CO and Distance PC were 0.95 (P < 0.01), 0.99 (P < 0.01), 0.92 (P < 0.01), and 0.99 (P < 0.01), respectively. The inter-observer agreement of Angle TS, Angle AW, Distance CO, and Distance PC were 0.97 (P < 0.01), 0.99 (P < 0.01), 0.95 (P < 0.01), and 0.99 (P < 0.01), respectively. One of the authors (R.N) measured all parameters three times, and the average of the three values was used for the analysis. The correlation among parameters were assessed. Five hypotheses were also verified.
Statistical analysis was performed using regression analysis to assess the relationships among the parameters. All statistical analyses were conducted using JMP version 14.2 (SAS Institute Inc, Cary, NC, USA). Statistical significance was set at P < 0.01.
Result
The mean (± SD) Angle TS, Angle AW, and Angle CS was 9.45° ± 3.70°, 15.7° ± 6.64°, and 96.2° ± 5.69°, respectively. Angle CS was less than 90° in 28 knees (13.5%) and was more than 90° in 180 knees (86.5%). Angle CS had a strong positive correlation with Angle AW (correlation coefficient r was 0.83, P < 0.01) (Figure 3). Angle TS had a moderate positive correlation with Angle AW (r = 0.52, P < 0.01) (Figure 4). However, no correlation was found between Angle TS and Angle CS (r = −0.047, P = 0.50) (Figure 5). The results showed that the tibial condyle itself did not have a posterior slope in 180 knees (86.5%). In such knees, the tibial condyle rotated posteriorly and the articular surface had a posterior slope relative to the tibial shaft. In 28 knees, the tibial condyle itself had a posterior slope. The larger the Angle AW, the larger the Angle CS (Figure 3). In general, Angle TS had a positive correlation with Angle AW and did not have a correlation with Angle CS. These data showed two results. First, the posterior slope of the tibial articular surface was mainly created by posterior rotation of the tibial condyle. Second, the point where Angle AW was 7.0°, Angle TS was 90.0° (Figure 3), meaning the tibial condyle was like a rectangle. As the tibial condyle rotated posteriorly, the tibial condyle changed its shape just like a rectangle transformed to a rhombus. The mean (± SD) length of Line 5, Distance CO, Distance AC, and Distance PC were 53.1 ± 4.65 mm, 32.4 ± 4.42 mm, 31.8 ± 4.19 mm, and 16.3 ± 3.05 mm. The mean (± SD) posterior condyle offset ratio (Distance PC/length of Line 5 X 100) was 30.7 ± 4.75%. The length of the tibial condyle (length of Line 5) had no correlation with Angle TS (r = 0.076, P = 0.28). Distance CO had a moderate positive correlation with Angle TS (r = 0.52, P < 0.01). Distance AC also had a moderate positive correlation with Angle TS (r = 0.45, P < 0.01) (Figure 6). Distance AC had a strong positive correlation with Angle AW (r = 0.62, P < 0.01). Distance PC had a positive correlation with Angle AW (r = 0.31, P < 0.01). Distance PC had a strong positive correlation with Distance CO (r = 0.59, P < 0.01). The results showed that the midpoint of the tibial condyle shift posteriorly according to the posterior rotation of the tibial condyle. This posterior shift of the tibial condyle increased the tibial posterior condyle offset. Angle TS, Angle AW, or Angle CS had no correlation with Angle SA (r = 0.13, 0.14, and 0.083; P = 0.070, 0.042, and 0.23, respectively). Angle TS, Angle AW, Angle CS or Angle SA did not have correlation with age (r = 0.12, −0.032, −0.11 and −0.038; P = 0.095, 0.65, 0.11, and 0.58, respectively).

Strong positive correlation between Angle AW and Angle CS. The larger the Angle AW, the larger the Angle CS was.

Positive correlation between Angle TS and Angle AW. The posterior tibial slope is mainly created by the posterior rotation of the tibial condyles.
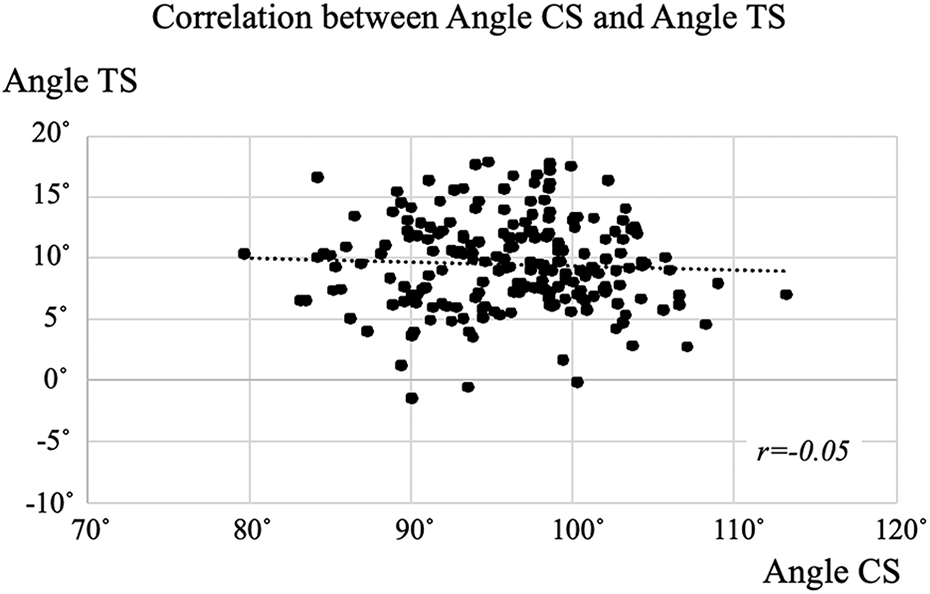
No correlation between Angle TS and Angle CS Angle. CS was more than 90 in 180 knees (86.5%). The tibial condyle itself does not have a posterior slope of the articular surface in such knees.

Positive correlation between Angle TS and Distance CO. The larger the tibial posterior slope, the more the tibial articular surface shifts posteriorly.
Discussion
This is the first paper to focus on the angle of the anterior wall of the tibial condyle relative to the tibial shaft (Angle AW) and the angle between the anterior wall of the tibial condyle and the medial articular surface (Angle CS). The results clearly showed that the tibial condyle itself did not have a posterior slope of the tibial articular surface in more than 86% of the cases. The posterior rotation of the tibial condyle creates the posterior slope of the tibial articular surface relative to the tibial shaft.
Hypothesis 1 was affirmed. Posterior rotation of the tibial condyle supports the concept of “constitutional” based on the Hueter-Volkmann’s law. However, the posterior rotation of the tibial condyle involved transformation. In understanding the mechanism of elasticity, it is necessary to use two areas and two directions of the body weight loading to explain the configuration of the tibial condyle (Figure 7). Without the body weight loading, the tibial condyle moved superiorly with the bone growth of the metaphysis (Figure 7b). The body weight loading has two directions (vertical loading and shear stress) (Figure 7c). In the metaphysis, the bone grows in the anterior region and the growth is retarded in the posterior region by vertical loading based on the Hueter-Volkmann’s law (Figure 7d). In the tibial condyle, the shear strain by shear stress induces a so-called rhombus transformation of the tibial condyle (Figure 7e). Hypothesis 2 was also affirmed. The results clearly showed a positive correlation between tibial posterior slope angle and the posterior shift of the articular surface. Both the posterior rotation and the rhombus transformation of the tibial condyle shift the tibial articular surface posteriorly. Hypothesis 3 was denied. Even though the articular surface in both the coronal and sagittal planes was formed based on the Hueter-Volkmann’s law, the mechanical loading was different between the coronal and sagittal planes. Hypothesis 4 was affirmed. The more posteriorly the midpoint of the condyle shifted, the larger the posterior condyle offset. Hypothesis 5 was also affirmed. No angle parameters correlated with the age. These results supported the concept of the constitutional. According to the constitutional varus in the coronal plane, posterior rotation of the tibial condyle can be called “constitutional posterior rotation” in the sagittal plane. Angle and distance parameters are necessary to analyze the configuration of the tibial condyles in both the coronal and sagittal planes.
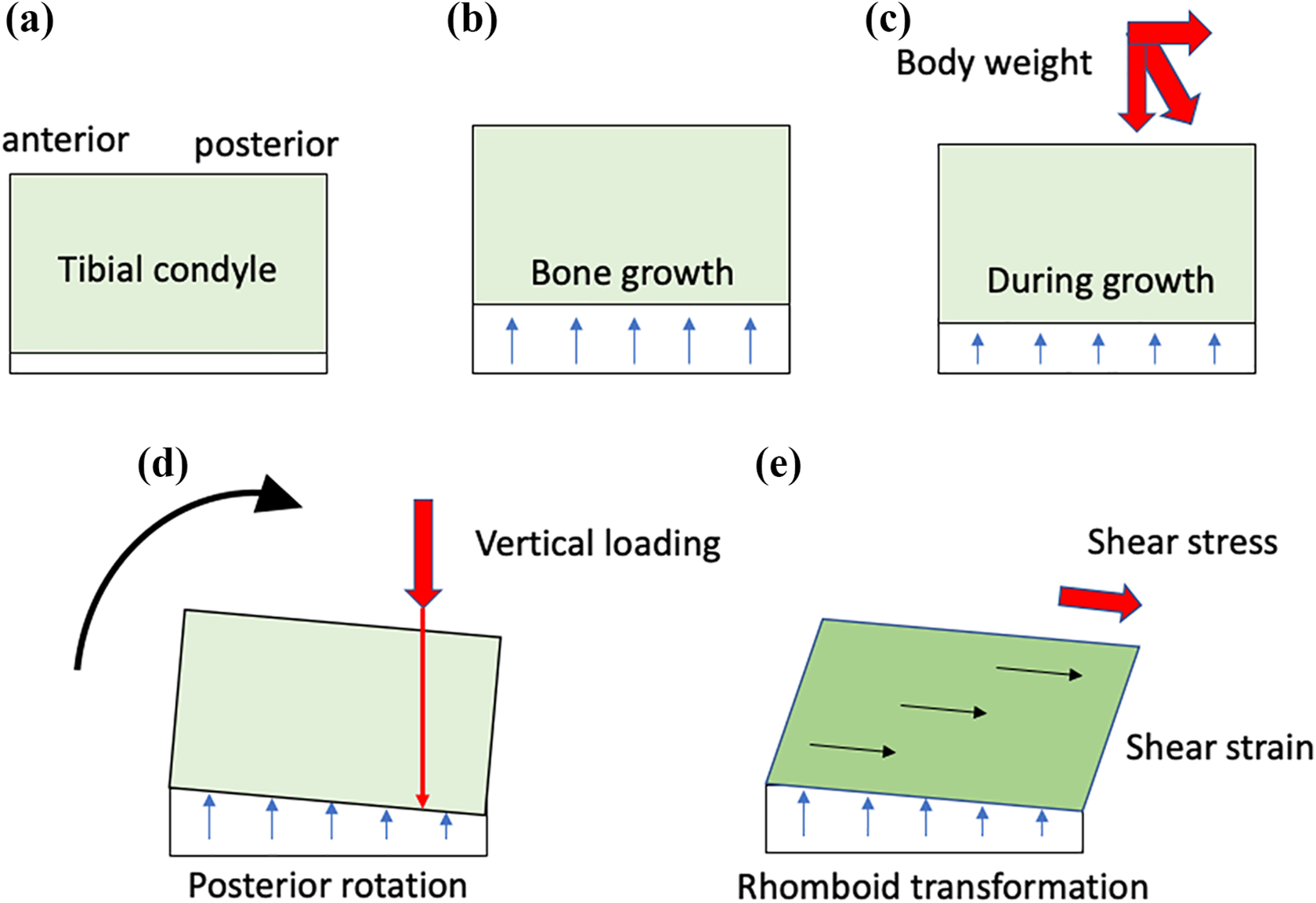
Formation of the tibial condyle in the sagittal plane. (a) Simplified scheme of the tibial condyle. (b) Tibial condyle moves superiorly with the bone growth at the metaphysis without body weight loading. (c) Body weight has two direction (vertical loading and shear stress). (d) With the vertical loading on the posterior part of the metaphysis, the bone growth is retarded and the tibial condyle rotates posteriorly. (e) With the shear stress, the tibial condyle has a rhomboid transformation due to the shear strain.
This paper has several limitations. First, the knee joints with medial arthritis were analyzed in patients and not in healthy people. Therefore, the normal value of the posterior slope of the tibial articular surface is still unclear. With parameters such as Angle TS and Angle AW, the normal values can be obtained. Although these normal values of all the parameters of the knee joint are very important, for knee surgeons, it is also important for them to have the accurate information on the anatomic variations of the bones in the knee joint of patients including elderly patients. Second, the flexion angle between the femur and the tibia was not the same among the 208 knees. The difference of the flexion angle may mean the difference of the rotation angle of the tibia relative to the femur and may influence the value of the angle parameters. In this study, cases with the flexion angle between the anterior cortex of the distal femoral and the tibial shafts less than 30° were not included because the knees have a screw home mechanism, and the rotation angle of the tibia relative to the femur changed dramatically from full extension to 30° of flexion. From 30° to 90° of flexion, the tibia rotates slightly internally relative to the femur. We assumed that such a small difference did not influence the results of this study. Therefore, radiographs with the angle between the femoral and tibial anterior cortex between 30° and 90° of flexion were used in this study. Third, the osteophytes may influence the shape of the anterior wall of the tibial condyle. In the ordinary knees, the straight part could be identified on the anterior wall of the tibial condyle, and in knees where the straight line could not be drawn were not included in this study. The posterior osteophyte also hinders the decision on the most posterior point of the tibial condyle. Such knees were also not included in this study.
It has been reported that a large posterior tibial slope was the risk factor for anterior cruciate ligament (ACL) injury. 9 –15 The results of this study showed three factors that could be used to assess the cases with ACL injury. First, the posterior rotation of the tibial condyle involves a posterior shift of the tibial articular surface. Therefore, the anatomical axis that is the central line of the tibial shaft does not coincide with the mechanical axis that is defined as the line between the center of the tibial articular surface and the center of the plafond (ankle joint). This discrepancy influenced the value of the tibial posterior slope angle. In previous studies, the reference line of the sagittal view has not been united. 9 –15 The anterior cortex of the tibial shaft may be the best reference line because a reference line can certainly be drawn along the cortex, and Angle AW and Angle CS can be assessed. The second factor is a possible hyperextension of the tibial condyle in knees with a larger posterior tibial slope. Full extension between the femoral and tibial shafts induces hyperextension of the tibial condyle including the articular surface and the ACL relative to the femur (Figure 8). Figure 8c also showed the difference in the location between the central lines of the femoral and tibial shafts because of the posterior shift of the tibial articular surface. The third factor is the distance from the tibial tuberosity to the femoral condyle (Figure 1). Because the position of the femoral condyle was decided on the tibial articular surface, 16 the larger the tibial posterior slope, the longer the distance between the tibial tuberosity and the femoral condyle. These factors may be complex risk factors for ACL injury.

Flexion angle relative to the femur is different between the tibial condyle and the tibial shaft in knees with a larger posterior slope. The solid line shows the central line of the femoral shaft. The dotted line shows the central line of the tibial shaft. (a) A tibia without posterior rotation of the tibial condyle. (b) A tibia with a larger posterior rotation of the tibial condyle. The location of the tibial articular surface with ACL and PCL relative to the femur is the same with (a). (c) Full extension between the femoral and tibial shafts in the knee with a larger posterior rotation of the tibial condyle induces hyperextension of the articular surface and the ACL. The location of the central line is different between the femoral and tibial shafts.
During TKA, the angle and position of the tibial component vary according to the tibial posterior slope. In knees without posterior slope angle, there is a possibility that the stem of the tibial component impinges against the anterior cortex of the proximal tibia if the tibial component is inserted with a larger posterior slope. In knees with a larger posterior slope angle, there is a possibility that the stem of the tibial component impinges against the posterior cortex of the tibia if the tibial component is inserted with no posterior slope. The tibial posterior slope and the posterior condylar offset should be taken into account in TKA to decide the optimal setting of the tibial component. The optimal posterior slope angle for TKA is still obscure. The position of the tibial and femoral components relative to the tibial tuberosity vary according to the posterior shift of the tibial articular surface. Further studies regarding the dependence of clinical results on the tibial posterior slope for TKA and the TKA design are necessary, considering the degree of the posterior shift and the angle of the posterior slope.
Conclusion
The posterior slope of the tibial articular surface is mainly created by the posterior rotation of the tibial condyle. The larger posterior slope of the tibial articular surface involves a posterior shift of the articular surface.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Each author certifies that his or her institution has approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported in part by Grant-in-Aid for Science Research (C), No. 19K09564 to Makoto Kawasaki from the Ministry of Education, Culture, Sports, Science and Technology, Japan.