
Abstract
Purpose:
According to the concept of the constitutional varus, the tibial articular surface (TAS) has varus inclination. On the other hand, it has been reported that proximal tibia vara involved medial shift of the TAS. However, it has not been assessed whether varus inclination of the TAS has a correlation with the medial shift. We investigated whether varus inclination of the TAS has a correlation with the medial shift. If there is a correlation between two parameters, the influence of the medial shift of the TAS on the value of the hip–knee–ankle (HKA) angle and the femorotibial angle should be considered.
Methods:
A total of 112 patients who underwent total knee arthroplasty had anteroposterior view tibia digital radiograph on which five parameters were analyzed. Varus angle of the TAS, the distance between the mechanical axis and the anatomical axis on the articular surface, and the width of the articular surface were measured.
Results:
The more the proximal tibia had varus deformity, the more the TAS shift medially would be. Therefore, the mechanical axis does not match the anatomical axis. Because the HKA angle was assessed based on the concept that the mechanical and anatomical axes match on the tibia, this angle may not express the true alignment of the lower extremity in knees with proximal tibia vara.
Conclusion:
In varus knees, the proximal tibia has a medial shift of the TAS that may influence the value of the HKA angle.
Introduction
Since the concept of “constitutional varus” knee was established, proximal tibia vara is recognized even in the normal knees. 1 In Asia, more varus alignment of the proximal tibia has been reported in knees with medial osteoarthritis. 2 –5 It has been reported that the proximal tibia vara involved the medial shift of the tibial articular surface (TAS). 4,6 –8 However, it is still obscure that the varus inclination of the TAS has a correlation with the medial shift of the TAS. The constitutional varus knee could be the consequence based on Hueter–Volkmann’s law, which states that growth at the epiphyses is retarded by increased compression, whereas reduced loading accelerates growth. 1 Our hypothesis was that if the varus deformity occurs at the proximal metaphysis of the tibia, the tibial condyle tilts medially and the TAS shifts medially. This study was performed to assess the correlation between the varus angle and the medial shift distance of the TAS. Then, the importance of the medial shift of the TAS was discussed because the hip–knee–ankle (HKA) angle that expresses the coronal alignment of the lower extremity is measured based on the concept that the mechanical axis matches the anatomical axis on the tibia. The medial shift of the TAS means the mechanical axis locates medial to the anatomical axis. This discrepancy of the two axes may influence the value of the HKA angle. The expression of the alignment of the tibial component in total knee arthroplasty (TKA) was also discussed because the alignment would be changed according to the choice of the mechanical or the anatomical axes. In this study, we aimed to determine whether the increased tibia vara was correlated with the medial shift in the TAS.
Material and methods
We performed TKA in 129 Kellgren–Lawrence grade 4 osteoarthritis (OA) cases between July 2015 and December 2016. This study consists of 112 knees with only medial OA among these TKA. The mean age was 75.5 years (range 57–91 years). There were 81 females and 31 males. The digital radiograph showing the anteroposterior (AP) view of the tibia was taken with the patella oriented forward in all cases before TKA so that the femoral condyle and the patella were also shown on the radiograph (Figure 1(a)). The X-ray beam was centered on the tibia with the radiography tube at a distance of 130 cm. A 14 × 17 inch2 cassette was placed immediately behind the subject, and the digital radiograph (Toshiba, Japan) was taken (Figure 1). A setting of 200 mA and a kilovoltage of 50 kV were used. The contours of bones were clear in all cases. Cases with lateral OA, bowing of the tibial shaft, and cases with torsion of the tibia were not included in this study. 8,9 Also, cases in which we were not able to identify the midpoint of the medial and lateral TAS were not included, as the TAS was defined as the line connecting the midpoint of the medial and lateral TAS. In total, 17 cases were excluded for these reasons. The center of the tibial plafond was located on the central line of the tibial diaphysis (the anatomical axis of tibia) in all cases. The digital data of the radiograph of the tibia were analyzed by the computer software (Toshiba). On the AP view radiograph of the tibia, the anatomical axis, the mechanical axis, and the tibial plateau tangent were drawn. The anatomical axis was the central line of the diaphysis of the tibia. The intersection between the anatomical axis and the plateau tangent was defined as point A. The mechanical axis was the line between the center of the notch of tibial spine (point M) and the center of the tibial plafond (Figure 1(b)). Two angle parameters and three distance parameters were measured. Those are the angle between the anatomical and mechanical axes (angle MA, the value was positive when the mechanical axis located medial to the anatomical axis), the angle between the tibial plateau tangent and the line perpendicular to the anatomical axis (angle SA), distance between point A and point M on the tibial plateau (distance MA, the value was positive when point M located medial to point A), the width of the TAS, and the distance between the medial edges, except the osteophyte of the TAS and point M (distance MM). One of us (RN) made all radiographic measurements. The measurement was repeated three times, and the average of the three values was used for the analysis. Reproducibility was performed on 40 subjects by two readers based on the previous studies to assess inter- and intraobserver reproducibility. 1,10,11 Reproducibility was blinded, with all measurements carried out with no knowledge of prior results, and all markings were erased for each reader. The intraobserver agreement of angle MA, angle SA, distance MA, width of the TAS, and distance MM was 0.80 (p < 0.01), 0.99 (p < 0.01), 0.98 (p < 0.01), 0.93 (p < 0.01), and 0.95 (p < 0.01), respectively. The interobserver agreement of angle MA, angle SA, distance MA, width of the TAS, and distance MM was 0.84 (p < 0.01), 0.99 (p < 0.01), 0.98 (p < 0.01), 0.89 (p < 0.01), and 0.90 (p < 0.01), respectively.

(a) An anteroposterior view radiograph of the typical tibia with proximal vara and medial shift of the tibial articular surface. (b) Five parameters on the tibia are shown. Rigid line; anatomical axis: the central line of the diaphysis of the tibia, dotted line; mechanical axis: the line between the center of the notch of tibial spine (point M) and the center of the tibial plafond. Point A: the intersection between the anatomical axis and the plateau tangent. 1. Angle MA: the angle between the anatomical and mechanical axes. 2. Angle SA: the angle between the tibial plateau tangent and the line perpendicular to the anatomical axis., 3. Distance MA: the distance between point A and point M on the tibial plateau. 4. The width of the TAS: the width of tibial articular surface. 5. Distance MM: the distance between medial edge except the osteophyte of the TAS and point M. TAS: tibial articular surface.
This study was approved by the Institutional Review Board of our hospital. Each author certifies that his or her institution has approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Statistical analysis was performed using regression analysis to assess the relationship with each parameter. All statistical analyses were performed using JMP version 12.2 (SAS Institute Inc., Cary, North Carolina, USA). Statistical significance was set at p value <0.01.
Results
The mean (± SD) angle MA and angle SA was 0.53 ± 0.62° (range −1° to 2.3°) and 6.5 ± 2.8° (−0.7° to 13.1°), respectively. The mean distance MA, the width of the TAS, and the distance MM (± SD) was 2.6 ± 3.3 mm (−5.9 to 13.6), 75.9 ± 5.8 mm (65.4–94.9), and 37.8 ± 3.3 mm (30.8–46.6), respectively. Figure 2 shows the relationship between the angle SA and the distance MA. The angle SA significantly correlated with the distance MA. The correlation coefficient was 0.58 (R 2 = 0.34). The more proximal tibia had varus deformity, the more the TAS shifted medially. The results showed that the distance MM was almost 50% of the width of the TAS. The distance between the center of the TAS and the point M was 0.17 ± 1.7 mm (−5.8 to 3.5). These results showed that the point M (mechanical axis) was located at the center of the TAS. The correlation coefficient between the angle SA and the width of the TAS was 0.11 (R 2 = 0.012). The varus angle of the TAS did not have a correlation with the width of the TAS. These results indicated that the more varus deformity of tibia involved more medial shift of the TAS, and the varus deformity was not due to the configuration of the proximal tibia.
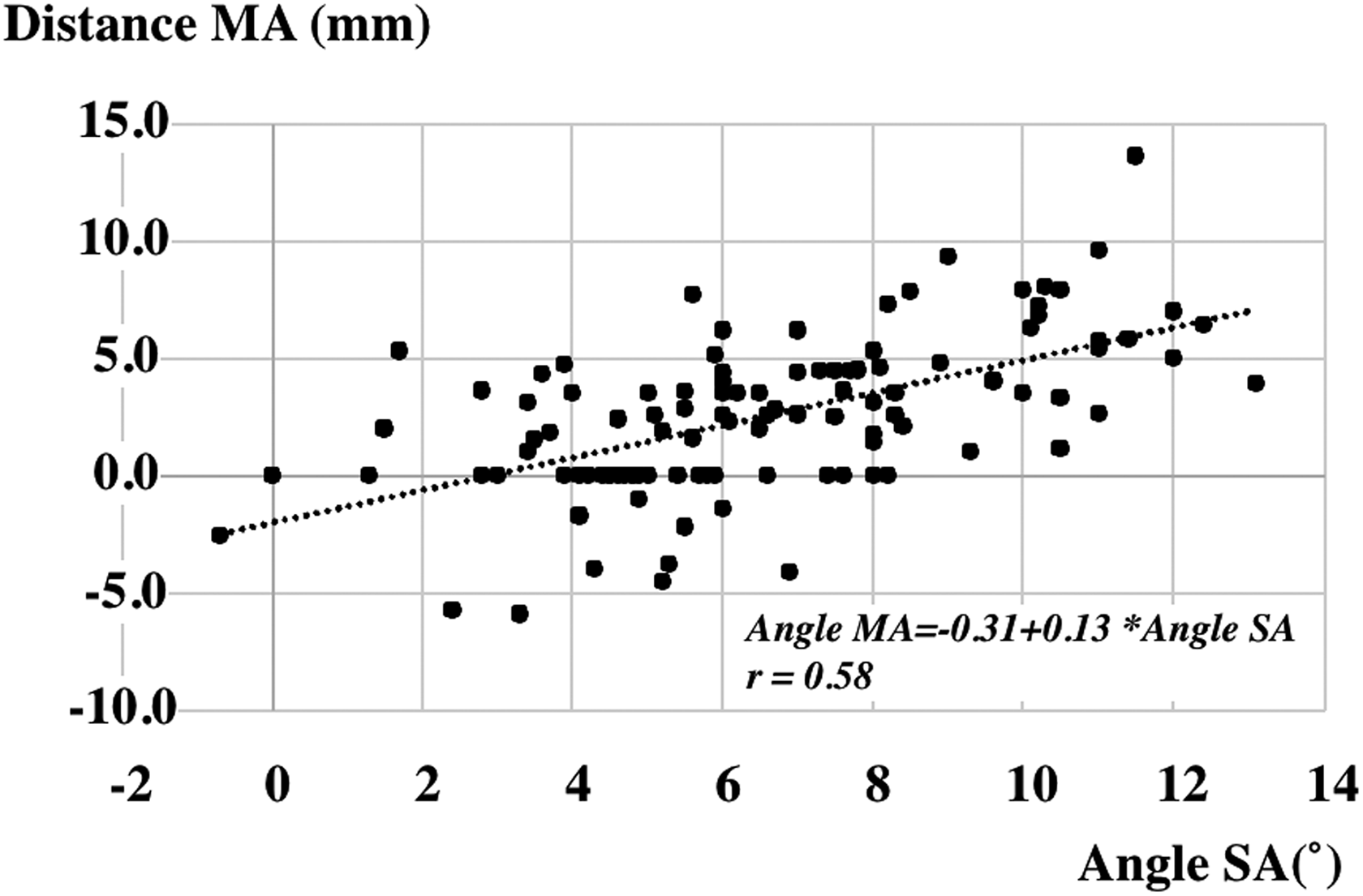
Relationship between angle SA and distance MA.
Discussion
The concept of the constitutional varus is more important in Asia than in Europe and the United States because patients in Asia had more anatomical variations of the femur and the tibia. Many articles reported that the characteristics of the anatomical variations in Asia were lateral and anterior bowing of the femoral shaft, the proximal tibia vara with the medial shift of the TAS, and the medial torsion of the tibia. 4 –6,8,9,12
The results of this study clearly showed the correlation between the varus angle and the medial shift distance of the TAS. The varus angle of the TAS did not influence the width of the TAS. The mechanical axis passed in the center of the TAS. It can be concluded that the medial OA did not change the configuration of the proximal tibia because all cases in this study have advanced OA. The results support that the constitutional varus occurs at the proximal metaphysis of the tibia. The most important finding is that the more varus deformity involved more medial shift of the TAS.
In the knees with proximal tibia vara, the mechanical axis locates medial to the anatomical axis. This discrepancy of two axes influences the value of the HKA angle. Figure 3 shows the problem of the value of the HKA angle in knees with the medial shift of the TAS. Figure 3(a) shows the normal alignment. The angle between the mechanical and anatomical axes of the femur is 6°. The varus angle of the TAS is 3°. The femorotibial angle (FTA) between the anatomical axes of the femur and the tibia was 174°. The HKA angle between the mechanical axes of the femur and the tibia was 0°. Figure 3(b) shows the proximal tibia vara without the medial shift of the TAS. The varus angle of the TAS is set 7°. The FTA is 178° and the HKA angle is −4° (4° varus). Both FTA and HKA angle show the varus alignment. Figure 3(c) shows the proximal tibia vara with the medial shift of the TAS. With the medial shift of the TAS, the ankle relatively shifts laterally from the center of the TAS that is the origin of the mechanical axis. In Figure 3(c), the FTA is 178°, but the HKA angle is 0°. The end point of the mechanical axis shifts laterally and the HKA angle cannot express the varus alignment correctly. The HKA angle underestimates the varus deformity in knees with the medial shift of the TAS.

(a) A scheme with normal alignment. The angle between the mechanical axis and anatomical axis of the femur is 6°. The varus angle of the TAS is 3°. The femorotibial angle (FTA) between the anatomical axes of the femur and the tibia was 174°. The HKA angle between the mechanical axes of the femur and the tibia was 0°. (b) A scheme with simple varus alignment. The varus angle of the TAS is set 7°. The FTA is 178° and the HKA angle is −4° (4° varus). (c) A scheme with varus alignment with medial shift of the tibial articular surface. The varus angle of the TAS is set 7°. The FTA is 178°, similar to (b), but the HKA angle is 0°. The end point of the mechanical axis shifts laterally and the HKA angle cannot express the varus alignment correctly. TAS: tibial articular surface; FTA: femorotibial angle; HKA: hip–knee–ankle.
The FTA also has a problem to express the alignment of the lower extremity in the coronal plane. The FTA is also measured based on the concept that the center of the TAS locates on the anatomical axis. The discrepancy between the anatomical and mechanical axes is not taken into account when the FTA is measured.
The medial shift of the TAS also influences the alignment of the tibial component in TKA. In Figure 4, the proximal tibia has the medial shift of the TAS. Therefore, the mechanical axis locates medial to the anatomical axis. Figure 4(a) shows the tibial component set perpendicular to the anatomical axis. This alignment is expressed as neutral by the FTA but is expressed as valgus by the HKA angle. Figure 4(b) shows the tibial component set perpendicular to the mechanical axis. This alignment is expressed as neutral by the HKA angle but is expressed as varus by FTA. One option to match the mechanical axis to the anatomical axis is the reduction osteotomy. This technique has been reported to reduce varus deformity. 12 The tibia is cut perpendicular to the anatomical axis and the tibial tray is set so that the center of the tibial tray is located on the anatomical axis. Size of the tray should be smaller than the size based on the TAS width. The bone that is not covered with the tray in the medial edge of the tibial condyle is resected. The original point M does not exist, and the new mechanical axis is the line between the center of the cut surface of the proximal tibia and the center of the tibial plafond. When using this procedure, the alignment is expressed as neutral by both FTA and HKA angle (Figure 4(c)).

(a) A tibial component is set perpendicular to anatomical axis. (b) A tibial component is set perpendicular to the mechanical axis. (c) A smaller tibia component is set perpendicular to anatomical axis and the reduction osteotomy was performed.
In TKA, the concept of the constitutional varus is one of the theoretical basis for the kinematic alignment. 13 If the kinematic alignment is simply applied to knees with the proximal tibia vara and the medial shift of the TAS, unexpected varus alignment may occur. A mechanical alignment was applied in this TKA series, not a kinematic alignment. The application of kinematic alignment to an Asian knee with a tibia vara may induce excessive varus alignment of the tibia, and the malalignment of the tibia varus position can increase the risk of long-term failure. 14 Care should be taken when the kinematic alignment is applied in the Asian patients.
In Asian patients, other anatomical variations should be considered when the coronal alignment of the lower extremity is assessed. The lateral bowing of the femoral shaft 3,5,15,16 influenced the expression of the HKA angle. The FTA cannot express the exact varus alignment in such knees. In Asia, there are patients who have both lateral bowing of the femoral shaft and the proximal tibia vara with the medial shift of the TAS. Therefore, our proposal is that when the HKA angle is expressed, the content of the anatomic variations is added as the annotation.
Our study has several limitations. First, because knees with only medial OA were assessed in this study, deformity and/or destruction of the knee joint might influence the value of measurements. The cases which had lateral OA, torsion of the tibia, and bowing of the tibial shaft were not evaluated in this series. Second, if the radiograph was taken with malrotation of the tibia, the posterior slope of the TAS may influence the value of the angle SA. Therefore, in this study, only the exact AP view radiograph was used. On the AP view radiograph, the center of the patella located the center of the femoral condyles. The distal tibiofibula joint can be clearly opened in the ankle joint. Third, the detailed configuration of the proximal tibia should be assessed in the three-coordinate system. However, the AP radiograph is the most popular tool to express the coronal alignment of the lower extremity. Fourth, only Asian patients were analyzed in this study; therefore, patients in other races may have different configuration of the proximal tibia vara. Further study is necessary to assess the patients such as in Europe and the United States. Fifth, we did not obtain a postoperative radiograph with a full-length HKA view. It would be valuable to evaluate this and compare pre- and postoperative radiographs for FTA and HKA angle of full-length HKA view in the future.
Conclusion
The proximal tibia vara involves the medial shift of the TAS. This medial shift of the TAS influences the values of the HKA angle and the FTA, and the expression of the tibial component alignment in TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported in part by Grant-in-Aid for Science Research (C), Nos 16K10925 and 19K09564 to MK from the Ministry of Education, Culture, Sports, Science, and Technology, Japan.