
Abstract
Background:
The best strategy for implant selection in midshaft clavicular fractures (MCF) remains controversial. The present study aims to determine the optimal strategy for implant selection by comparing plate and Titanium Elastic Nail (TEN) with respect to outcomes and related complications and analyze the results based on fracture patterns.
Methods:
A total of 97 patients with MCF who underwent plate (48 patients) or TEN (49 patients) fixation were retrospectively reviewed. Both groups were divided into three subgroups by fracture type using the AO Foundation/Orthopaedic Trauma Association classification: simple fracture (type A), wedge fracture (type B), and multi-fragmentary fracture (type C). The observed outcome measures were bone union rate, related complications, functional scores, and patient satisfaction score. These outcomes were analyzed based on the fracture classification.
Results:
Both groups demonstrated excellent union rates (p = 0.495) and similar functional scores (p > 0.05). Visual analog scale (VAS) for satisfaction was better in TEN than plate fixation (p < 0.001). In type A and B subgroups, there were no significant difference in functional scores between plate and TEN fixation (p > 0.05). In type C subgroup, however, both VAS for pain and DASH score in TEN fixation were significantly worse than in plate fixation at 2 and 6 weeks postoperatively (p < 0.05). The incidences of clavicle shortening and skin irritation are higher especially in type C subgroup of TEN fixation (p < 0.05).
Conclusion:
Patient satisfaction of TEN fixation was higher than that of plate fixation, but TEN fixation had a higher incidence of early postoperative pain and migration in type C fractures. Therefore, type A and B fractures can successfully be treated with plate or TEN fixation, but type C fractures should be treated with plate fixation.
Keywords
Introduction
Clavicle fractures are common injuries accounting for 2.6 to 4.0% of all fractures. 1 It has been previously published that mid-third fractures constitute approximately 80% of all clavicle fractures. 2 Over the last 15–20 years, treatment of adult clavicle fractures has dramatically changed. Traditionally, midshaft clavicle fractures (MCFs) have been treated non-operatively with the expectation of good clinical outcomes and a high rate of fracture union. 2 Recent studies, however, demonstrated that malunion and nonunion rates with non-operative treatment are higher than anticipated. 29,30 According to a meta-analysis of recent randomized studies, the nonunion rate for nonoperative treatment was 16.5%, which is higher than the 1.9% found after surgical treatment. 3 Additionally, analysis of functional outcomes showed better results following surgical treatment. Accordingly, the proportion of clavicle fractures being treated with surgery is increasing. 4
Plate fixation is the standard surgical method for MCFs. 5 This method is advantageous because of restoration and preservation of the natural anatomy and length of the clavicle. 3,5 However, reported complications include wound infection and non-union because of extensive periosteal stripping. 5,6 And other complications are skin numbness and poor cosmetic results due to the larger incision. 5 –7
Another surgical option for MCFs is intramedullary (IM) nailing. IM devices utilize minimally invasive surgical techniques, resulting in smaller incisions, preserved periosteum and shorter operation times. 8,9 Because of these, advantages of IM nailing are lower incidence of infection, nonunion, skin numbness and scar. 8,9 Various devices for IM clavicle fixation are available, including Kirschner-wires, Rockwood Pins, Hagie Pins, Rush pins, Küntschner nails and Knowles pins. 5,8 However, the most widely used and studied implant is the titanium elastic nail (TEN). 5,8 TEN has been successfully used for treating MCFs and shows comparable results in terms of functional outcomes and union rates to plate fixation. 10
Although several comparative studies between plate and TEN fixations have been conducted, 7,11 –13 the optimal operation strategy for MCFs remains unclear. And to our knowledge, few studies have compared both methods on the basis of MCF fracture pattern as we have done. Therefore, the purpose of this study are to determine the optimal strategy for implant selection by comparing plates and TENs with respect to outcomes and related complications and to analyze the results based on fracture patterns.
Materials and methods
Patient selection and demographics
From January 2015 to June 2018, 151 consecutive patients with MCFs who underwent internal fixation with plate or TEN were retrospectively reviewed. This study was reviewed and approved by the institutional review board for our institution and informed consent was obtained from all participants. Operative indications for MCFs include clavicle shortening greater than 1.5 cm, angulation exceeding 30 degrees, and/or displacement by one bone width on radiography. Exclusion criteria included: neurovascular injury, surgery performed more than 3 weeks after fracture, no follow-up more than 1 year postoperatively, open or pathologic fractures, and concomitant injury or re-fracture of the clavicle.
Of the 151 patients reviewed, 116 (76.8%) had a fracture of the middle third according to the AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification of clavicle fractures. 14 However, 19 were excluded from the study because they met the exclusion criteria. A total of 97 patients with MCFs who met the study criteria were evaluated in our study. The patients were divided into two groups based on the fixation method: plate and TEN. The plate and TEN fixations were performed for 48 and 49 patients, respectively (Figure 1). Table 1 summarizes the characteristics of both groups. We further divided patients into subgroup A, B, and C by fracture type using the AO/OTA classification: simple fracture (type A), wedge fracture (type B), and multi-fragmentary fracture (type C) (Figure 2). 14

Flowchart of patient selection for this study. TEN: titanium elastic nail.
Patient demographics.

a Data presented as mean ± standard deviation and statistical comparison performed using the independent t-test or Mann-Whitney U-test in cases of non-normal distribution.
b Data presented as number (%) and statistical significance was determined by Pearson’s chi-square test.

Midshaft clavicle fractures classified according to the AO/OTA classification. (a) The diaphysis is defined as that part of the bone between the two end segments. Diaphyseal fractures are divided into three subtypes based on fracture morphology; (b) Type A-simple: a single circumferential disruption, (c) Type B-wedge: contact between the main fragments after reduction usually restoring the normal length of the bone, and (D) Type C-multifragmentary: many fracture lines and fracture fragments. AO/OTA: AO Foundation/Orthopaedic Trauma Association.
Surgical procedure and postoperative rehabilitation
All surgeries were performed by two experienced trauma surgeons at our institution. The fixation device was chosen according to surgeon preference. Both surgeons performed both surgery types.
Clinical and radiological assessment
Postoperative functional outcomes were assessed using visual analog scale (VAS, 0–10 cm) for pain and Disabilities of the Arm, Shoulder and Hand (DASH) score at each follow-up appointment 2, 6, and 12 weeks, and 6 and 12 months postoperatively. The shoulder active range of motion (ROM) were measured with a goniometer for forward flexion, abduction, external rotation, and internal rotation at final follow up. The satisfaction of the patients after surgery was quantified using VAS (0 being least satisfied and 10 being most satisfied) at 12 months postoperatively. Complications such as superficial infection, skin numbness, skin irritation, wound dehiscence, implant migration, implant breakage, and refracture after implant removal were assessed in the outpatient clinic.
Nonunion was defined as the lack of callus, and periosteal or endosteal healing response after 6 months. 15 Delayed union was defined as the lack of callus between 3 and 6 months after surgery. 15 The length of clavicles was measured with method by Lazarides and Zafiropoulos. 16 Comparing the operated to the non-operated clavicle, significant clavicle shortening was considered to be present when there was more than 15 mm difference in length between the two sides. Measurements and review of the radiographs were performed by the two surgeons and two independent researchers.
Statistical analysis
The categorical variables age, sex, mean follow-up, mechanism of injury, intermediary fragment, fracture type, and complications were presented as absolute numbers (percentage) and compared between TEN and plate groups. Groups were compared with independent t-test or Mann-Whitney U-test in cases of non-normal distribution and Pearson’s chi-square test or the Fisher’s exact test in cases of low cell frequencies. Statistical significance was set at p < 0.05. SPSS 19.0 statistical software (IBM, IL, USA) was used to analyze the data.
Results
Clinical outcomes
The mean postoperative DASH scores at 12 months was not significantly different (p = 0.637) between the plate (3.9 ± 4.6; range: 0 to 13.3) and TEN (3.5 ± 4.3; range: 0 to 15.8) fixation groups. Both groups showed similar shoulder pain at 12 months as measured by VAS (plate fixation: 0.6 ± 0.9; TEN fixation: 0.9 ± 1.1; p = 0.216). There were no differences in VAS for pain and DASH score of the plate and TEN fixation groups at every other follow-up time point (Figure 3) (Online Supplementary Table A). Shoulder ROM at final follow up showed satisfactory results in both plate and TEN fixation groups, and there was no statistically significant difference between both groups (Table 2). Mean VAS for patient’s satisfaction at 12 months after the surgery was better in TEN fixation than plate fixation (plate fixation: 7.3 ± 1.6; TEN fixation: 8.2 ± 1.1; p < 0.001).

Graph showing functional outcomes between plate fixation and TEN fixation. Error bars represent 95% confidence intervals. TEN: titanium elastic nail; VAS: visual analog scale; DASH: Disability of the Arm.
Shoulder range of motion at final follow up between plate fixation and TEN fixation.a

a Data presented as mean ± standard deviation and statistical comparison performed using the independent t-test or Mann-Whitney U-test in cases of non-normal distribution.
When comparing the functional outcomes between the plate and TEN fixation groups in each fracture type, functional outcomes between the two fixation groups did not differ significantly in type A and B fracture at every other follow-up time point (Figure 4(a) and (b)) (Online Supplementary Table B and C). In type C fracture, however, both VAS for pain and DASH scores in TEN fixation were poor than plate fixation at 2 and 6 weeks postoperatively (Figure 4(c)) (Online Supplementary Table D).

Graph showing functional outcomes between plate fixation and TEN fixation in (a) type A fractures, (b) type B fractures, and (c) type C fractures. *p < 0.05. Error bars represent 95% confidence intervals. TEN: titanium elastic nail; VAS: visual analog scale; DASH: Disability of the Arm.
Radiological outcomes
Both methods of fixation had high rates of union; 97.9% (47/48) with plate fixation and 100% (49/49) with TEN fixation (Figure 5). There was a single case of nonunion after plate fixation that was treated with auto-iliac bone graft and revision plate fixation (Table 3). Delayed union was seen in a single TEN patient, but no additional surgical treatment was done and the bone was united by 9-month follow-up.
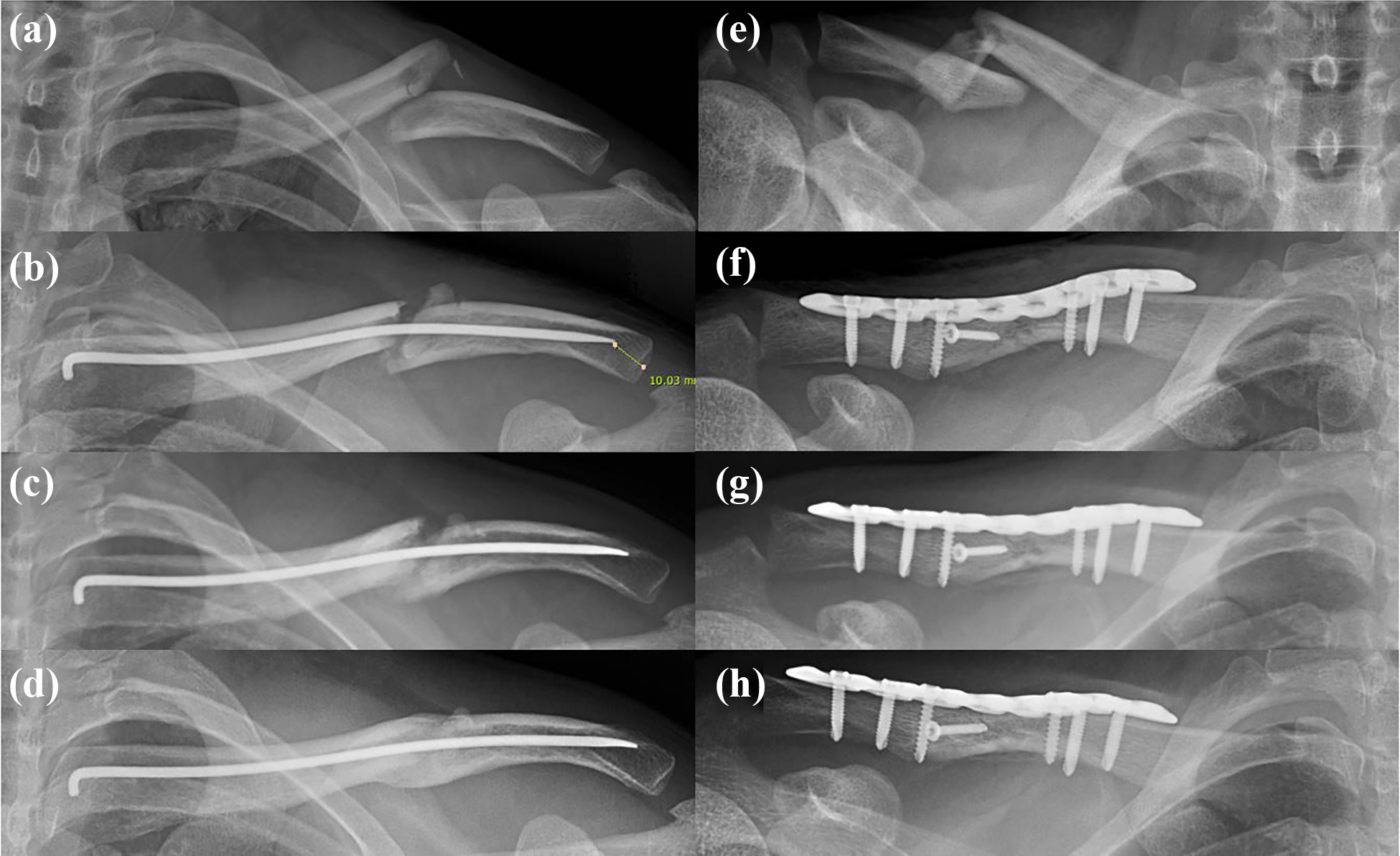
(a) A left simple midshaft clavicle fracture (type A) with marked displacement. (b) Postoperative radiography after closed reduction and internal fixation with TEN of the clavicle fracture. (c) Radiography at 6 weeks postoperatively showing callus formation at the fracture site. (d) Radiography at 6 month postoperatively showing fracture union. (e) A right wedge-shaped midshaft clavicle fracture (type B) with marked displacement and shortening. (f) Immediate postoperative radiograph shows successful open reduction and plate fixation with an additional lag screw. (g) Radiography at 6 weeks postoperatively. (h) Radiograph at 6 months postoperatively shows fracture union.
Postoperative complications.a

a Data presented as number (%).
b Statistical significance was determined by Pearson’s chi-square test, or, in cases of low cell frequencies, the Fisher’s exact test.
The incidence of clavicle shortening was significantly higher after TEN fixation compared to the plate group (p < 0.001), and 12 TEN patients (24.5%) presented with clavicular shortening exceeding 1.5 cm (Table 3). Shortening with angulation occurred in two TEN cases; with undersized nails (2.0 mm) used in both instances (Figure 6). These cases showed angulation of 25 and 35 degrees, respectively. There were significant differences in the incidence of clavicle shortening between fracture subgroups following TEN fixation (p < 0.001). The incidence of clavicle shortening was higher in type C (77.8%) fractures than in type A (7.7%) and B (28.6%) (Table 4).

A left clavicle midshaft fracture in a 18-year-old male with narrow intramedullary cavity. (a) Plain radiography corresponds to simple fracture (type A) by AO/OTA classification. (b) TEN fixation with 2.0 mm was performed after reduction. (c) The operated clavicle shortened and angulated at 2-weeks postoperatively. (d) Bone union was achieved without further angulation at 24-weeks postoperatively. AO/OTA: AO Foundation/Orthopaedic Trauma Association; TEN: titanium elastic nail.
Complication between subgroups of TEN fixation.a

a Data presented as absolute numbers (percentage).
b Statistical significance was determined by Fisher-Freeman-Halton test.
Complications
Patients in the TEN group had a higher rate of skin irritation than plate group (p = 0.028); with 2 plate patients (4.2%) reporting irritation over the surgical site due to the plate and screws, and 10 TEN patients (20.4%) reporting irritation proximal to the nail insertion site. Skin perforation in two patients required revision shortening of the TEN (Figure 7). There was no statistically significant difference in reoperation (p = 0.617). Superficial infection occurred in two patients with plate fixation and one patient with TEN fixation; however, all patients were treated with oral antibiotics and union occurred successfully with no statistically significant differences (p = 0.617). There were no cases of deep infection in either group. Skin numbness occurred in 20 plate patients (41.7%), which was significantly higher than in the 2 TEN patients (4.1%) (p = 0.001). Wound dehiscence was not significantly different between fixation groups (p > 0.999). There was one re-fracture after TEN removal, and a plate was used to correct re-fracture. These data are summarized in Table 3.

A right clavicle midshaft fracture in a 55-year-old male. (a) Plain radiography corresponds to multifragmentary fracture (type C) by AO/OTA classification. (b) TEN fixation was performed after reduction. (c) The clavicle shortened and TEN migrated to the proximal direction at 2 weeks after surgery. (d) The photography showing penetrating the skin and the nail protruded. (e) 6-weeks after nail cutting, bone union was achieved without further shortening. AO/OTA: AO Foundation/Orthopaedic Trauma Association; TEN: titanium elastic nail.
Discussion
TEN showed excellent results in bone union rates and functional outcomes as good as plate. Even overall patient satisfaction at final follow up after surgery was higher in TEN fixation than plate fixation. However, the most relevant difference was in postoperative complications, with TEN associated more often with clavicle shortening and angulation, as well as implant-related skin irritation. In type C fractures, TEN fixation had significantly higher incidence of clavicle shortening and skin irritation compared to plate fixation. The VAS for pain and DASH scores of plate fixation group at the first 6 weeks showed better results compared plate fixation group.
Traditionally, MCFs have been treated nonoperatively using a Figure-8 bandage wrap or sling. 2,17 Currently, however, many different operative treatment options are available for MCFs including IM nails, wires, plates, minimally invasive plate osteosynthesis, and several others. With plate fixation, the surgeon can perform a direct reduction of the fractured clavicle fragments, making it the standard operative method for MCFs. 5 In several studies, plate fixation has shown good union rates and improved functional outcomes. 13 The present study also showed good union rates and functional outcomes following plate fixation. However, devascularization of soft tissues is inevitable with this method, and direct visualization of the fractured fragments results in a subsequent incapacitation of bone and increased blood loss. 8,15,18 Furthermore, there is a stripping of periosteum, which increases the risks of postoperative infection and non-union, and the large incision can yield cosmetically unacceptable scars and skin numbness. 5,6 Taking these complications into account, IM fixation was devised as a less invasive alternative to plate fixation for the surgical treatment of MCF. Peroni first described IM fixation for clavicle fractures 1950, which induces secondary bone healing by preserving the biology of fractured bone. 19,20 However, IM fixation has been associated with insufficient rotational stiffness, weaker compression forces at fracture sites, and pin migration. 21,22 The use of TEN for clavicle fractures was first described by Jubel et al. 20,23 TEN fixation leads to functional outcomes and union rates comparable to those observed in plate fixation.
Several studies have reported faster recovery following plate fixation compared to TEN fixation. 11,13 The present study showed no differences between both fixation methods in functional recovery measured by DASH score. However, in type C fractures, TEN fixation showed worse VAS for pain and DASH score at the 2 and 6 weeks follow-up than plate fixation. Therefore, multiple intermediary fragments interfered with the restoration of function after IM fixation, 24 making plate fixation preferable with in cases with higher comminution, which is supported by our study. After the 12-week follow-up, there was no difference in VAS for pain and DASH score, which is the result of callus formation that stabilized the fracture and alleviated pain, thus diminishing functional outcome differences.
There were studies that IM nail of MCFs leads to excellent functional results and excellent cosmetic and resulting in high overall satisfaction. 7,25 In the present study, the overall patient satisfaction measured by VAS at the last follow-up showed better results in TEN than the plate, showing the same results as in the previous study. TEN utilize minimally invasive surgical techniques, resulting in smaller incisions, less skin numbness, and better cosmetic results. 7 In addition, no foreign substance was visible and touched on the skin
TEN patients experience higher incidence of clavicle shortening. 7,24 The present study confirmed these findings, although to a lesser extent than those reported previous studies. Clavicle shortening of more than 15 mm is associated with shoulder discomfort and dysfunction. 16,26 In this study, clavicle shortening exceeding 15 mm occurred in 12 (24.5%) cases of TEN fixation. Although there was no statistical difference in functional and VAS for pain scores between the shortened and non-shortened groups, this study showed the trend from previous studies demonstrating a relationship between discomfort and dysfunction. No clavicle shortening occurred in the plate fixation group. Multi-fragmentary fractures could lead to the overlapping of fragments which then results in clavicular shortening. 27 In subgroup analysis of TEN, clavicle shortening occurred in 77.8% of type C fractures and only 7.7% of type A fractures and type B fractures resulted in clavicle shortening less frequently (21.4%) (Table 4). It is believed that, unlike in multi-fragmentary fractures, proximal and distal fragments closely touched, allowing for these fragments to support each other reduced the potential for shortening. In the type A subgroup of TEN, two patients experienced clavicle shortening related to angulation from fixations where narrow IM cavities were treated with 2.0 mm nails. TEN is not suitable for narrow IM cavities, and patients who cannot tolerate nails thicker than 2.5 mm should be treated with plate fixation. In type C fractures with the highest rate of clavicle shortening, there were no differences in VAS for pain and DASH scores between both fixation after 6 weeks postoperatively. Functional outcomes tended to be poor in patients with clavicle shortening in the early stages with less stability before bone healing. However, after bone heals, the presence of shortening does not seem to affect functional outcome. Another complication after TEN fixation is skin irritation to the nail insertion site because of nail migration. The incidence of skin irritation in TEN fixation was from 5.2% to 66.1%. 7,11,23,24,28 In the present study, TEN fixation showed the higher incidence of skin irritation than plate fixation (TEN fixation, 20.4%; Plate fixation, 4.2%), especially in type C fractures (Type A, 11.5%; Type B, 14.3%; Type C, 55.6%). It is consistent with the tendency of the incidence of clavicle shortening. Multi-fragmentary clavicle fractures are prone to clavicle shortening causing the TEN to migrate and irritate. 11 Also, when the lateral tip of TEN was located far from the acromioclavicular joint, poor fixation stability resulted in clavicle shortening and TEN migration. 7 In two patients who underwent revision surgery to shorten the TEN because of skin perforation and medial migration of TEN, in present study, the lateral tip of TENs was located more than 3 cm from the acromioclavicular joint (Figure 7(b)). Thus, positioning the lateral tip of TEN as close to the lateral cortex of the clavicle without perforating the cortex as possible would be a good way to achieve better fixation stability and to prevent from skin perforation, irritation, and TEN migration. 28
There are several limitations to this study. First, this is a retrospective study. However, despite the two different surgical methods, we minimized enrollment bias by applying uniform surgical technique and rehabilitation strategy. Additionally, demographic and clinical evaluations of patients during follow-up periods were as similar as possible. Second, the follow-up period only extended 1-year after surgery. This is a relatively short period of time to evaluate recovery, but ample for observing fracture union and functional recovery. Finally, type C fractures have a less influence on our results because more than half in TEN fixation group were type A fractures. However, as the plate and TEN groups did not show significant differences in distribution of fracture types, the comparison between them was meaningful. A randomized controlled trial with same distribution of fracture types may be needed to provide a higher level of evidence. There are limitations, but we believe our analysis is the first to compare functional scores and complications based on AO/OTA classification and thus aids in fixation method selection based on fracture type.
Conclusion
Both plate and TEN fixation showed excellent results in bone union rates and functional scores in all fracture types. Patient satisfaction of TEN fixation was higher than that of plate fixation, but TEN fixation had a higher incidence of early postoperative pain and migration in multi-fragmentary clavicle fractures. Therefore, simple and wedge fractures can successfully be treated with plate or TEN fixation, but multi-fragmentary clavicle fractures should be treated with plate fixation.
Supplemental material
Supplemental Material, Supplementary_Table - Plate fixation versus titanium elastic nailing in midshaft clavicle fractures based on fracture classifications
Supplemental Material, Supplementary_Table for Plate fixation versus titanium elastic nailing in midshaft clavicle fractures based on fracture classifications by Jun Sung Park, Sang Hyun Ko, Taek Ho Hong, Dong Jin Ryu, Dae Gyu Kwon, Myung-Ku Kim and Yoon Sang Jeon in Journal of Orthopaedic Surgery
Footnotes
Acknowledgement
This study was supported by Inha University research grant.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The protocol for this study was approved by the Institutional Review Board of Inha University Hospital, Incheon, Korea (IRB No. INHAUH 2019-06-030).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.