
Abstract
Introduction:
For the fixation of displaced midshaft clavicular fractures, different plates are available, each with its specific pros and cons. The ideal plating choice remains subject to ongoing discussion. Reconstruction plates are cheap and easily bendable, but their strength and stability have been questioned. The anatomical precontoured locking plates provide better stability and strength compared with the reconstruction plate.
Materials and methods:
We have analyzed both prospectively and retrospectively 55 cases of displaced midshaft clavicular fractures treated surgically using precontoured anatomical locking plate (24 cases) or reconstruction plate (31 cases) for patients admitted in our institute between January 2011 and December 2017. The clinical and radiological outcomes between the reconstruction plate and precontoured anatomical locking plate were compared using Quick Disability of the Arm, Shoulder and Hand (DASH) score and plain radiographs, respectively.
Results:
The mean time to union was 16.3 weeks in the reconstruction plate group compared with 13.4 weeks in the precontoured locking plate group. The mean score in Quick DASH was 32.65 in the reconstruction group and 25.44 points in the precontoured locking plate group. We had complications such as hypertrophic scar, painful shoulder, and restricted range of motion in both the groups, whereas screw cutout and plate failure were noted only in the reconstruction plate group, which needed implant removal. The mean follow-up period was 16.44 months (14–31 months). The removal of implant was carried out in three patients in the reconstruction group. None of the group had nonunion.
Conclusion:
Surgical management of fresh middle third clavicle fractures with anatomical precontoured locking plate provided stable fixation, faster union, and better functional outcome compared with the reconstruction plating. Anatomical plate had the advantage of less soft tissue stripping, and there is less need for lag screw fixation of the plate for fracture stability as precontoured plate itself provides a rigid construct.
Keywords
Introduction
The clavicle is an S-shaped bone and is the only osseous link between the upper extremity and the trunk. Fractures of clavicle are common injuries in adults, accounting for 5% of all fractures and 44% of all shoulder fractures. 1 –3 Historically, the midshaft clavicle fractures have been usually treated by conservative measures. 4,5 However, in recent literature, there is a growing trend toward operative treatment for displaced, comminuted fractures resulting from high-energy injuries, such as motor vehicle accidents, industrial accidents, and sporting injuries. This is done to prevent shortening or angular deformities that can cause pain, 6 and also the importance of obtaining functional satisfaction with early exercise has been emphasized. 7 There are various surgical methods for treating clavicle midshaft fractures, such as intramedullary K-wires or Steinmann pins fixation and plate fixation. 8 –11 In particular, plate fixation can help obtaining firm anatomical reduction in severe displaced or comminuted fracture and restoring the biomechanics of shoulder girdle. In this study, we aimed at elucidating the clinical and radiological outcomes between the reconstruction plate and precontoured anatomical locking plate for displaced midshaft clavicle fractures and compared their functional results using Quick Disability of the Arm, Shoulder and Hand (DASH) score 12 and plain radiographs, respectively.
Materials and methods
This retrospective and prospective study was conducted after obtaining institutional ethical committee clearance. The study was started in 2015 where we retrospectively reviewed cases operated for displaced midshaft clavicle fractures in adults by open reduction and internal fixation with a plate and screws from January 2011 to December 2015 and prospectively included patients who were operated with reconstruction plates or anatomical precontoured clavicle locking plates from 2015 to 2017. All the surgeries were performed by trauma surgeons with a minimum of 5 years of experience in fracture fixation surgeries.
The operative indications were fractures involving ≥20 mm displacement or shortening, comminuted fractures, fractures with suspected soft tissue interposition that could not be reduced by a closed reduction, open fractures, multiple fractures, and fractures with a neurovascular injury and associated fractures. A decision on plate selection was not affected by the indications. Pediatric clavicle fractures and undisplaced clavicle fractures in adults were excluded from this study.
Operative technique
The patients underwent surgery within 2 weeks after the injury by various orthopedic surgeons at our academic institution who used the same surgical indications, surgical technique, and rehabilitation protocol. Prophylactic antibiotics were given. With the patient under general anesthesia, in the beach-chair position, a transverse skin incision was made along the superior border of the clavicle under general anesthesia. 7 Fixation was performed following a reduction with minimal periosteal stripping. In reconstruction plate groups, plates were contoured to the shape of the clavicle, and in anatomical locking plate group, plate matching the contour of the native bone was chosen in such a way that three screws were made on either sides of the fracture as shown in Figure 1.
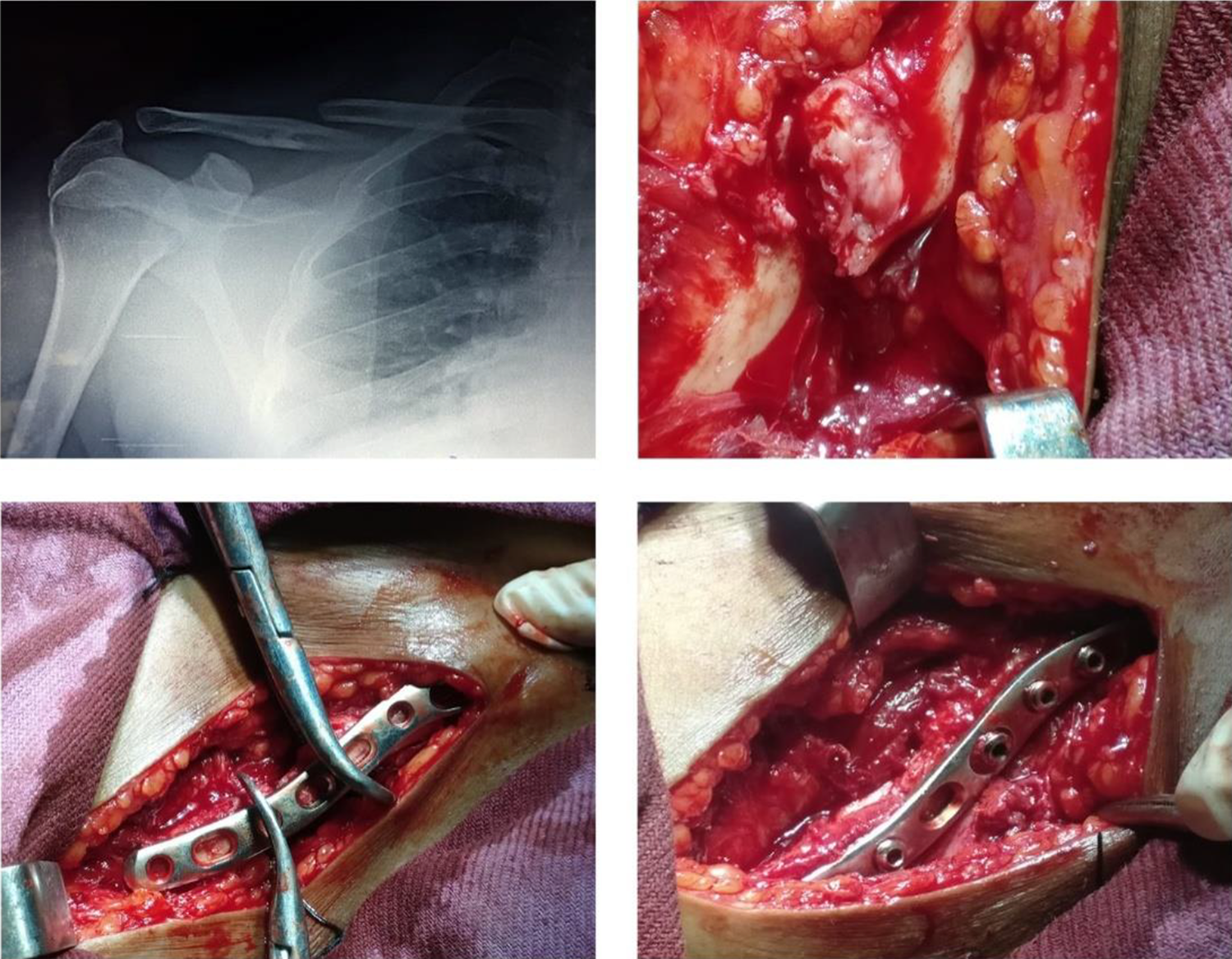
Minimal periosteal stripping and intraoperative ease of reduction of the fracture with the precontoured plate and its fixation.
If necessary, lag screw was used in cases where fracture reduction could not be achieved due to a severe comminuted fracture with ≥2–3 bone fragments. In cases where severe comminution was observed in the inferior surface of the clavicle, autogenous iliac bone grafting was also performed to avoid nonunion or fixation failure or metal breakage caused by tension (cantilever mechanism). The plate was positioned in the superior aspect of the clavicle, which was found to be anatomically and biomechanically ideal for the reduction and fixation as described in various studies. 13,14 Screw length was strictly monitored to prevent any neurovascular complication from screw prominence. An arm sling was used for approximately 2 weeks after surgery.
The exercise protocol consists of pendulum exercises up to functional movements without weight-bearing in the first 2 weeks. More active exercise is initiated between 2 and 4 weeks postoperatively. After 6 weeks, strengthening exercises of shoulder were started.
Assessment of treatment outcome
The patients were seen at 6 weeks and at 3, 6, and 12 months after surgery. At each visit, and for any complications, anteroposterior radiographs were made. Radiographic union was defined as complete cortical bridging across the fracture site. Functional assessment was done using the DASH scores as suggested by the American Academy of Orthopaedic Surgeons. Statistical analysis was performed using SPSS Version 25.0 (SPSS Inc., Chicago, Illinois, USA). An independent t-test and χ 2 test were used. A p-value < 0.05 was considered significant.
Results and observation
The demographic profile of the study population is compared in Table 1, and it has been noted that fractures were found in the working age-group mostly with male predominance and dominant side injury mostly in both the groups. Manual laborers are mostly affected with high-velocity road traffic accidents contributed to most of the injuries resulting in clavicular fractures.
Demographic profile of the study population.
The patients’ age, gender, cause of injury, and fracture pattern were not statistically significant between the two groups (p > 0.05). The mean operative time was 85.1 min (standard deviation (SD) = 19.4 min) in the reconstruction group, and it was 59.3 min (SD = 12.6 min) in the anatomical locking group, showing notable intergroup differences. We found a significant difference with the number of fractures requiring lag screw usage to achieve reduction and bone grafting between these groups. The shorter time is mainly due to the less need for plate contouring in the precontoured plate group compared with the reconstruction plate group where most of the time was spent in contouring the plate to match the native bone curvature.
Bony union was achieved in all the cases after surgery at 16.3 weeks (range: 8–31 weeks) and 13.2 weeks (range: 8–18 weeks) in the reconstruction and anatomical locking groups, respectively, indicating a significant intergroup difference (p < 0.05). In the clinical assessment, the reconstruction group and anatomical locking group showed a mean Quick DASH score of 32.65 (SD = 9.4 points) and 25.44 points (SD = 12.7 points), respectively (p > 0.05).
Figure 2 shows the comparison of the fixation of displaced midshaft clavicle fracture with reconstruction plate and precontoured locking plate highlighting the ease of reduction of fracture without any interfragmentary lag screws in the precontoured plate providing adequate stability.

A1 & A2 shows pre-op and post-op x rays of fixation with precontoured anatomical locking plate B1& B2 shows pre-op and post-op x rays of fixation with reconstruction plate.
Postoperative complications were noted in both the groups. All the patients of both the groups had plate prominence, but it does not seem to be of major concern for our patients. We used implants which provided us with three designs of precontoured plates with varying sizes in each of them, which mostly matches the native contour of the patients. However, in some patients, mild offset of 2–4 mm can be tolerated, which was the main reason behind the complication of hardware prominence noted in this group as shown in Figure 3.

Complications such as screw cutout and implant prominence which needed implant removal.
In the reconstruction group, there was hypertrophic scarring without pain in three cases (9.6%), limited shoulder motion in two cases (6.4%), painful shoulder in one case (3.2%), screw cutout in two cases (6.4%) as shown in Figure 3, and plate failure in one case (3.2%). In the anatomical locking group, hypertrophic scarring was observed in two cases (8.2%) and painful shoulder in one case (4.1%), but neither screw loosening nor plate failure was observed in this group. Infection and nonunion were not observed in either group (Table 2).
Outcome analysis between the two groups.

Quick DASH: Quick Disability of the Arm, Shoulder and Hand; SD: standard deviation.
Discussion
Most clavicle midshaft fractures are treated conservatively. In 1960, Neer 15 reported that nonunion occurred only in 3 of the 2235 patients in whom clavicle midshaft fractures had been treated nonsurgically. In 1968, Rowe 16 reported that nonoperative treatments resulted in nonunion only in 4 of the 566 clavicle midshaft fracture cases and the surgically treated patients presented with more postoperative complications and nonunion. Accordingly, nonoperative treatments have been preferred by many surgeons. However, according to Zlowodzki et al., 13 nonunion occurred after nonoperative treatments in 6% of 1145 clavicle midshaft fracture cases; the percentage increased to 15–20 particularly in the 159 fracture cases with severe displacement, while only 2% nonunion was noted in the surgically treated cases. In addition, the extent of fragment displacement is closely associated with fracture union, 17,18 and anatomical restoration of the displacement is considered essential for rapid healing and quick recovery.
Hence, there has been an increasing interest in surgical treatments with open reduction and internal fixation. In particular, operative treatments are performed more often for the treatment of clavicle midshaft fractures due to the increasing instances of severely displaced and comminuted fractures caused by high-energy injuries in motor vehicle accidents, industrial accidents, and sport injuries. 6,7 Shen et al. 11 obtained satisfactory outcomes in 94% of the 232 cases by open reduction and plate fixation.
In 2007, the Canadian Orthopaedic Trauma Society reported that internal fixation with plates resulted in more rapid union, excellent clinical outcomes, and lower complication rates in 132 patients with displaced clavicle fractures compared with nonoperative treatments. 19 The operative methods for the treatment of clavicle midshaft fractures involve intramedullary K-wire fixation or Steinmann pin fixation and plate fixation. The procedures using the former two materials result in low resistance to torque, carry risks of pin loosening and infection, and require a long-term fixation period. 20,21
Open reduction and internal fixation with plates, such as Sherman plates, dynamic compression plates, and semi-tubular plates, can be effective in obtaining anatomical reduction, applying direct compression to the fracture site, and producing resistance to torque. However, it is disadvantageous in achieving firm fixation because it is difficult to hold the plates to the clavicle in severely comminuted fracture cases. 22
In contrast, reconstruction plates can be manipulated to fit the contour of the clavicle and fracture pattern to obtain firm fixation, are lighter and thinner than locking precontoured plates, and are durable to multidirectional mechanical stress imposed on the fracture site. 11,14 On the other hand, the penetration of the opposite cortical bone for screw fixation may cause damage to the subclavian artery, and firm fixation may be difficult to maintain in osteoporotic patients over 50 years of age. 23,24 Here the precontoured locking plates come into play by increasing the screw hold in the osteoporotic bones along with a stable and rigid fixation.
The clavicle is a complex of five joints, and disturbances at any of these joints are likely to interfere with the smooth rhythm observed in movements of this complex. The overall ratio of scapulothoracic to gelenohumeral movements of 1:2 is made possible by a clock work mechanism that involves movements at these two articulations with an axial rotation of the clavicle that connects the shoulder girdle to the torso. 25 Clavicular elevation is rather consistent in the first 90° of humeral elevation. For every 10° of humeral elevation, there is a 4° of clavicular elevation. The rotation of the clavicle also occurs. 26 Shortening or malunion affects this normal biomechanics resulting in late complications.
Current radiographic indicators for surgery are displacement and shortening. It is reported that scapular upward rotation, posterior tilting, and internal rotation increase with malunion. 27 A shortening of >2 cm or >10% is presumed to be an indicator of poorer outcomes and of a possible increased risk of glenohumeral arthritis in those treated conservatively. 10,28 –30
In this study, the use of reconstruction plates did not result in complications, such as subclavian artery injuries and brachial plexus injuries, but shoulder pain and limitation of motion occurred during the follow-up period. Although nonunion or functional disabilities were not observed in these cases, it is believed that precontoured locking plates could be used as an alternative to reconstruction plates to reduce the number of complications. The advantages of precontoured locking plate include strong fixation due to locking principle between the screw and the plate and blood supply preservation due to minimal contact between the plate and the cortical bone. 31,32
With conventional screws and plates, fracture site stability is provided by friction between the plate and the bone cortex. Accordingly, screws need to be fixed onto both cortices. In contrast, when a locking plate is used, an external force is transmitted from the cortical bone through the threaded plate hole to the plate because the screw head is locked firmly in the threaded plate hole. Therefore, the plate does not need to be compressed onto the cortical bone for stability, which results in good preservation of the blood supply, and the plate thread is also helpful in preventing screw loosening or instability. 33,34
When locking plates are used to treat clavicle midshaft fractures with a minimum periosteal stripping, it promotes rapid union. 33 There was a significant difference between the reconstruction plate group and anatomical precontoured locking plate group in terms of the union period and surgical time, whereas Quick DASH score at the final follow-up did not yield any significant difference between the two groups. Nevertheless, a precontoured plate can be an effective replacement for a reconstruction plate considering that complications, such as screw loosening and plate failure, which were not observed in the precontoured locking plate group with the added benefit of earlier mobilization.
In noncontoured locking plates, contouring was performed with locking sleeves inserted into screw holes considering the problem of locking compression plates that screw fixation can be weakened if the breakage of the screw holes occurs in the plate thread during plate contouring. It was well addressed in the anatomical precontoured locking plates. In view of the precontoured plates, reduction was achieved easily with the plates, bone grafting was not much needed compared with the reconstruction plates, and a separate lag screw to make the reduction stable was not much needed in the locking plate group as shown in Figure 2.
Unfortunately, surgical treatments for clavicle fractures leave distinct scars on the shoulder. Ali Khan and Lucas 35 suggested that patients with clavicle midshaft fractures could suffer from hypertrophic scarring after surgical treatments with plates. Surgical scars are currently considered major complications due to the increasing demand for esthetics. Six of our patients had hypertrophic scarring after surgery and complained of discomfort in carrying out their daily activities. However, none of them had associated pain. The removal of implant was carried out in three patients in the reconstruction group, where two of them for screw failure and one for plate failure, and but not in patients from precontoured locking plate group. None of the group had malunion or nonunion.
However, the patients should be informed of the possible appearance of surgical scars preoperatively, and surgical techniques should be improved to address the problem. VanBeek et al. 36 reported prominent hardware in 9 of 14 patients (64.3%) in the noncontoured group and 9 of 28 patients (32.1%) in the precontoured group. Similarly, in our study also, most of the patients had prominent hardware less with precontoured plates.
This study had some limitations. The conclusions drawn from this nonrandomized analysis cannot be generalized because of the small number of cases in each group and that the study design included retrospective cases. Therefore, the efficacy of a reconstruction plate and precontoured locking plates for the treatment of midshaft clavicle fractures should be tested in prospective randomized studies involving a larger number of cases.
Conclusion
In conclusion, the surgical management of fresh middle third clavicle fractures with anatomical precontoured locking plate provided stable fixation, faster union, less number of plate-related complications, and better functional outcome compared with the reconstruction plating. The main advantage of operative intervention using precontoured locking plate is restoring the natural anatomical shape of clavicle and its length to maintain the normal biomechanics of shoulder girdle along with earlier mobilization. Treatment should be individualized by the treating surgeon with due consideration of the patient’s age, nature of violence, dominant limb, activity level, associated fractures, and expectations of treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.