
Abstract
Aim:
This study compared the results of tarsal tunnel syndrome release surgeries using mini-open incisions and standard incisions.
Patients and Methods:
From January 2012 until April 2018, 31 feet of 29 patients diagnosed with tarsal tunnel syndrome were treated surgically. 15 feet of 15 patients underwent surgeries utilizing minimally open technique and 16 feet of 14 patients underwent surgeries utilizing standard incisions. The following preoperative and postoperative data was obtained: foot and ankle muscle testing results, posture analyses, anthropometric measurements, joint movement ranges, pain complaints, endurance evaluation results, and functional test results. The mean follow-up period was 38 months (13–88 months).
Results:
The mean operation times were 26.8 min (23–30 min) using the standard incision and 13.3 min (9–17 min) using the mini-open incision (p < 0.05). In the preoperative and postoperative comparisons of the total muscle strength and total joint limit values of the healthy and affected feet, statistically significant improvements were observed in both the mini-open incision and standard incision groups (p < 0.05). Moreover, statistically significant improvements were seen in both groups in the postoperative repeated toe raises for 1 minute assessments of the affected foot (p < 0.05). In the foot function index and functional foot score values, statistically significant improvements were seen between the preoperative and postoperative values in both groups (p < 0.05).
Conclusions:
Based on the results of this study, using a tunnel ligament release instrument assisted minimally open surgery to loosen the laciniate ligament may present an alternative to the standard incision, with its significantly decreased morbidity rate and cosmetic success.
Introduction
Tarsal tunnel syndrome is an entrapment neuropathy caused by the compression of the posterior tibial nerve in the tunnel formed by the flexor retinaculum behind and below the medial malleolus of the ankle. The patient complaints include pain along the posteromedial hindfoot and ankle, with occasional pain radiation, numbness, and/or paresthesia distally within the plantar surface of the foot or proximally along the medial side of the leg. During a clinical examination, palpation and percussion (Tinel’s sign) cause paresthesia along the medial or lateral plantar nerve. 1– 3 Dorsiflexion of the ankle, heel eversion, or dorsiflexion and eversion applied together by stretching the tibial nerve cause the symptoms to reappear.
The diagnosis of tarsal tunnel syndrome first rests on the patient’s history and clinical examination. Electrodiagnostic tests are used to support the diagnosis or to differentiate tarsal tunnel syndrome from L5–S1 radiculopathy and sensory peripheral neuropathy. Diagnostic ultrasonography (USG) is useful for detecting ganglia, varicose veins, lipomas, tenosynovitis, and talocalcaneal coalitions. 4 Magnetic resonance imaging (MRI), which can add further detail at a high accuracy rate (83%), can be used to identify soft tissue lesions. 5 – 8 Moreover, plain radiographs of the ankle can be used to demonstrate structural abnormalities, such as hindfoot varus/valgus, tarsal coalitions, osteophytes, or evidence of a previous trauma. 9
Although the entrapment is often idiopathic within the fibro-osseous tarsal tunnel, in approximately 50–60% of the cases, a compression etiology is identifiable, such as a ganglion cyst, lipoma, venous anomaly, or previous trauma. 10 Surgical treatment includes nerve decompression as well as the treatment of any associated etiology. 9–11
In this paper, we proposed a minimally open surgical technique by using a tunnel ligament release instrument to release the laciniate ligament. The purpose of this study was to determine whether there were any differences in the results between a tunnel ligament release instrument assisted minimally open surgery and a conventional open surgery in the treatment of tarsal tunnel syndrome
Patients and methods
Approval for this study was granted by the local ethics committee (07.11.2019-190214). From January 2012 until April 2018, a retrospective evaluation of patients who operated by three surgeons due to tarsal tunnel syndrome surgeries in three different clinics was conducted. The following were obtained by another orthopedic surgeon rather than the operating surgeon from each patient’s medical records; demographic data, incision type, surgery time, complications, preoperative and postoperative foot function index 12 and functional foot scores, 13,14 foot and ankle muscle test results, posture analysis, anthropometric measurements, joint movement range, pain (location, time, type, and relationship to movement), and endurance evaluation results (while the patient was standing unsupported on the affected foot, with the other leg flexed at 90°, the number of repeated toe raises for 1 minute was recorded).
Tarsal tunnel syndrome was diagnosed with both history, clinical findings including pain, numbness and paresthesia within the plantar surface of the foot or proximally along the medial side of the leg, Tinel’s sign and EMG testing. EMG testing and plain radiographic imaging of the ankle were performed routinely in all of the patients, and the EMG results were used to pinpoint the nerve entrapment. More than 50% differences between the nerve conduction velocity (NCV) of two sides, distal motor latencies more than 7.0 msec and sensory latencies prolonged more than 2.3 msec were the findings used in this study to diagnose TTS. After the EMG examination, all of the patients underwent USG examinations. USG images were videotaped, collected and reevaluated by a experienced radiologist in a single center in order to detect any ganglia, varicose veins, lipomas, tenosynovitis, and/or talocalcaneal coalitions. 4 MRI examinations were not performed routinely, but only if they were deemed necessary after the USG, especially for suspected space-occupying lesions. Following the clinical evaluation, before considering surgery, conservative treatments were attempted in all of the patients. The conservative treatment options included anti-inflammatory medications and activity modifications in combination with various physiotherapy agents and stretching programs, such as wearing comfortable shoes in order to correct instability or impaired biomechanics, orthoses for arch support and to achieve a neutral position for the foot, immobilization with night splints or removable walking boots, bandaging, steroid injections, and ice packs. 9,15,16 If the conservative treatment for a mean of 2 months was insufficient, decompression surgery was considered.
Retrospective evaluation of patients who underwent tarsal tunnel syndrome surgeries through standard incision and mini-open incision by using tunnel ligament release instrument (KnifeLight system, Stryker Instruments, Kalamazoo, MI, USA) in three different clinics was conducted. The inclusion criteria were as follows; tarsal tunnel syndrome diagnosed with electromyography (EMG), complete preoperative and postoperative medical records, no systemic diseases that could account for lower extremity neuropathy (such as gout, diabetes mellitus, or hypothyroidism), not lacking vitamin B12, and no regular alcohol consumption. The exclusion criteria were as follows: incomplete follow-ups and/or medical records, tarsal tunnel syndrome revision surgery, history of healthy or affected foot and ankle surgery, severe foot deformity requiring additional surgery, post-traumatic tarsal tunnel syndrome, and masses (such as ganglion cysts, lipomas, and venous anomalies).
Statistical analysis
All of the data was recorded and analyzed by another author (D.N.D.) using IBM SPSS Statistics for Windows (Version 20.0; IBM Corp., Armonk, NY, USA). A frequency analysis was performed, and the conformity to normal distribution was tested using the Kolmogorov-Smirnov test. For those values with abnormal distributions, logarithmic conversions were made and the distributions were reassessed. Parametric tests (Independent samples t test and post hoc Tukey test) were used for the groups with normal distributions, while nonparametric tests (Mann-Whitney U test and Kruskal-Wallis test) were used for those with abnormal distributions. The continuous data was presented as the mean ± standard deviation (SD) or median (minimum–maximum), as appropriate. All of the hypotheses were two-tailed, and an alpha critical value of 0.05 was considered to be statistically significant.
Surgical technique
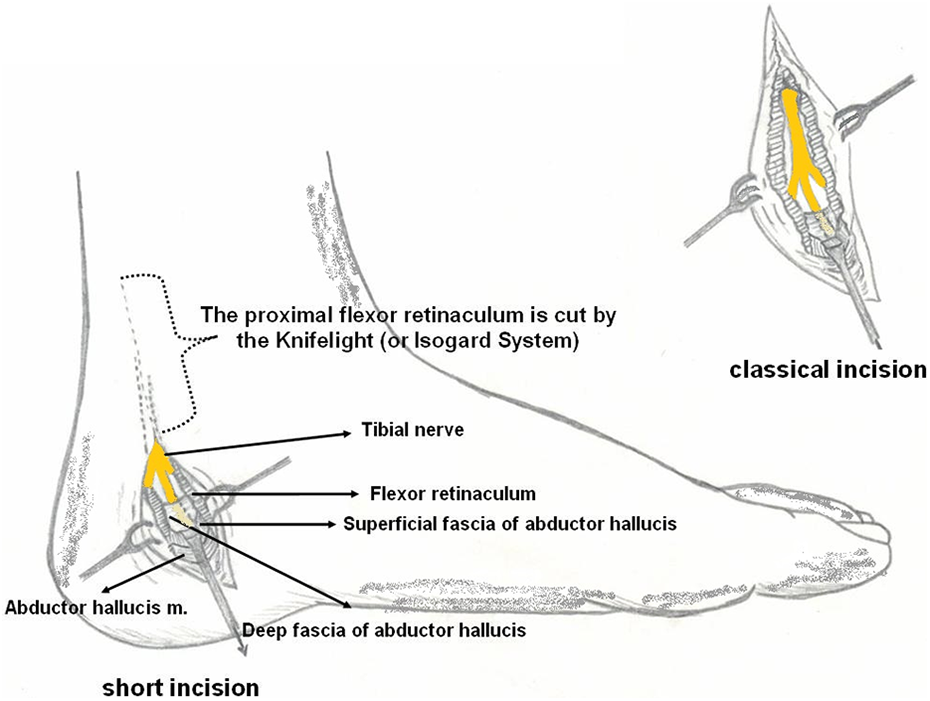
Each patient was positioned in a supine on the operating table, and either spinal anesthesia or general anesthesia was used. Typically, 2.5× loupe magnification was used in these procedures. An incision was made over the course of the tibial artery, which can usually be palpated easily. This incision was approximately 1 cm from the tip of the medial malleolus and approximately 2–3 cm behind the medial edge of the distal tibia. Distally, after passing the calcaneofibular axis, the incision was directed anteriorly in a curved fashion. The superior extension of the classical incision was not performed when using this modified technique, and generally, a 3–4 cm incision was sufficient for this procedure. The differences between the mini-open and standard incisions are shown in Figures 2 and 3 .

(a) KnifeLight system. (b) Isogard system..
Medial aspect of the ankle. Incision for tarsal tunnel release.

The left foot of a 45-year-old female. The proximal flexor retinaculum is cut using the KnifeLight system.
Next, a gentle, sharp dissection continued through the subcutaneous tissue with careful attention placed on the piercing branches of the calcaneal nerves. Distally, the superior edge of the abductor hallucis was identified. The fascia of the abductor muscle was opened and retracted, thus opening a small window through the inferior aspect of the laciniate ligament. The superior and inferior walls of the flexor retinaculum were detached using the handpiece of an Adson-Brown blunt dissector. Although, we preferred to use the KnifeLight system (Stryker Instruments, Kalamazoo, MI, USA), the Isogard system (Koby Surgical, Houston, TX, USA) can also be used for this modification. The KnifeLight was turned on, and the long blade was inserted under the flexor retinaculum. With the short blade in the space between the flexor retinaculum and the underlying tissues, the cutting edge was placed in the previously cut groove. The knife was gently directed toward the flexor digitorum longus tendon. The cut edges of the flexor retinaculum were then retracted in order to inspect the canal contents, and to check for the completeness of the structure division.
Finally, the tourniquet was released, and hemostasis was obtained. The skin was closed subcutaneously in the usual manner. The neurovascular bundles on the medial and lateral sides of the foot were identified in the distal aspect of the incision. The reason for using the minimally open tunnel ligament release instrument system for the surgical decompression of the tibial nerve was to avoid a longer incision (Figure 2 ), especially in the superior direction. This technique should not be used for the release of the distal part of the tibial nerve after tibial nerve branching (Figure 3 ).
Results
Based on the exclusion criteria, three patients undergoing tarsal tunnel syndrome revision surgeries, seven patients with associated space-occupying lesions (such as a ganglion cyst, lipoma, or tumor), and five patients with incomplete records or follow-ups after treatment were excluded. Therefore, this study included 31 feet of 29 patients (2 patients were bilateral) who underwent tarsal tunnel syndrome surgeries, and they were divided into two groups based on the use of a mini-open incision or a standard incision. Group 1 included 15 feet of 15 patients with mini-open incisions, while 16 feet of 14 patients with standard incisions comprised Group 2. Group 1 consisted of nine females and six males with a mean age of 41 years old (range: 22–67 years). Group 2 consisted of 10 females and 4 males with a mean age of 44 years old (range: 25–63 years) (Table 2 ). The mean follow-up period was 38 months (range: 13–88 months).
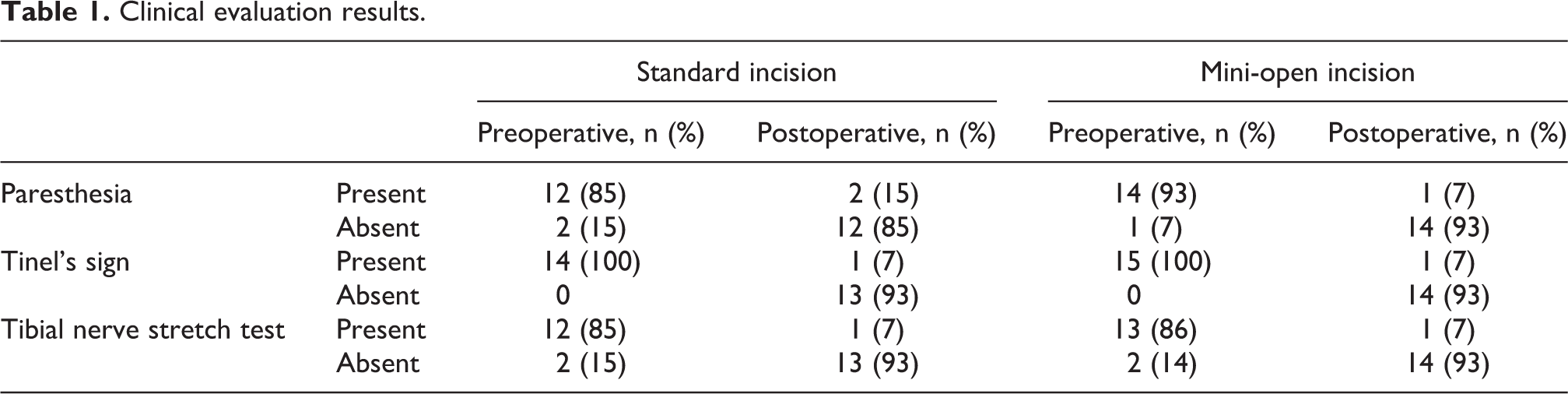
Clinical evaluation results.
Patient demographics and surgery times in Group 1 (mini-open incision) and Group 2 (standard incision).

The clinical evaluations and symptom severities were examined, and there was a postoperative improvement in the patients’ complaints (Table 1 ). Moreover, the operation time means were 26.8 min (range: 23–30 min) for the standard incisions and 13.3 min (range: 9–17 min) for the short incisions (p < 0.05). The reduction in the operation time was determined to be statistically significant (Table 2 ).
Positive Tinel’s signs were present preoperatively in both the short incision and standard incision groups. Postoperatively, the Tinel’s signs resolved in 86.3% and 87.5% of the patients in the short incision and standard incision groups, respectively. There were no statistically significant difference between two groups (p > 0.05).
In the preoperative and postoperative comparisons of the total muscle strength and total joint limit values between the operated feet and the contralateral unaffected side, statistically significant improvements were observed in both the mini-open incision and standard incision groups (p < 0.05). Moreover, statistically significant improvements were seen in both groups in the postoperative repeated toe raises for 1 minute assessments of the affected foot (p < 0.05). Statistically significant improvements between the preoperative and postoperative foot function index and functional foot score values were also seen in both groups (p < 0.05) (Table 3 ).
Pain severity and functional evaluation.

With regard to the postoperative complications, local infections were seen at the incision sites of two patients in the standard incision group and one patient in the mini-open incision group. A temporary increase in paresthesia was observed in one of the first patients to undergo surgery using a mini-open incision, but the patient had completely recovered by the second postoperative month.
Discussion
Tarsal tunnel syndrome is an entrapment neuropathy that is seen when the tibial nerve or one of its branches is compressed under the tarsal tunnel. Generally, patients complain of a burning pain spreading from the heel to the toes on the plantar surface, as well as pins and needles and numbness. In addition, paresthesia, dysesthesia, and hyperesthesia are among the frequently seen indications. 17,18
The literature has reported success rates of 44–96% after tarsal tunnel decompression surgery. 9 This wide variation in the success rate is probably due to the patient selection, surgical technique, and surgical intervention timing. Nagaoka and Satou and Pfeiffer and Cracchiolo reported that the successful outcomes were seen more often in the cases with space occupying lesions. 1,10 Additionally, Sammarco and Chang reported better outcomes if the patient exhibited symptoms for less than 1 year. 11 Similarly, Takakura et al. reported poor nerve recovery if the decompression surgery was conducted more than 10 months after the onset of symptoms. 5 In our study, Tinel’s sign was the main clinical tool used to evaluate the surgical success. Positive Tinel’s signs were present preoperatively in both the short incision and standard incision groups. Postoperatively, the Tinel’s signs resolved in 86.3% and 87.5% of the patients in the short incision and standard incision groups, respectively. In the comparison of the total muscle strength and total joint limit values between the operated feet and the unaffected contralateral sides, statistically significant improvements were observed in both groups (p < 0.05). Moreover, the comparison between the preoperative and postoperative foot function index, functional foot score, and repeated toe raising for 1 minute test values in the affected feet showed statistically significant improvements in both groups (p < 0.05).
A statistically significantly shorter operating time was seen in the mini-open incision group, with mean operation times of 13.3 minutes for the mini-open incision group and 26.8 minutes for the standard incision group. With the increasing number of operations, the operation time decreased in the incision group. Moreover, the postoperative test results were similar between the two methods, with the mini-open incision being as effective as the standard incision. When both techniques were assessed in terms of complications, no significant difference was seen. Only a temporary increase in paresthesia was encountered in one case in the mini-open incision group.
In this paper, we have reported our experiences with mini-open incisions compared to standard incisions for the treatment of tarsal tunnel syndrome. The short incision technique is contraindicated in tarsal tunnel syndrome revisions, post-traumatic cases, and masses (ganglion cysts, lipomas, and venous anomalies). In order to compare this technique with the standard incision, those patients with trauma etiologies and masses were excluded from both groups. After surgery, according to Tinel’s test, the success rate was over 85% in both groups (86.3% for the mini-open incision group and 87.5% for the standard incision group). Although the patients with space occupying lesions were excluded from this study, favorable results were obtained in both groups with no statistically significant difference.
There is little information in previous studies regarding the gender distribution of tarsal tunnel syndrome. Only the study by Shapiro and Preston reported that a slightly higher risk (56%) was observed in the females. 19 In the current study, 65.5% of the patients were females (19 females and 10 males).
Foot deformities, which comprise a significant contribution to the development of tarsal tunnel syndrome, are most commonly seen in pes planus and valgus heels. 20,21 A study by Lau and Daniels reported that with tarsal tunnel syndrome, a loss of level tread on the ground may develop, or the indicators of this syndrome may increase in severity. 21 It was also stated that while the tarsal tunnel narrows in a varus heel, in a valgus heel, there is increased tension on the tibial nerve. Therefore, in both conservative and surgical treatment, relieving the pressure by loosening the nerve is important for the foot to achieve a neutral tread. 21 In a similar study by Lau and Daniels, pes planus was created surgically in cadavers; then, using tarsal tunnel loosening and stabilization techniques, the effects on the tibial nerve tension were evaluated. 20 The researchers concluded that increasing the foot stability with a triple arthrodesis and calcaneocuboid arthrodesis reduced the tibial nerve tension more effectively. The conclusion implied that there would be a higher success rate in surgical tarsal tunnel decompression by adding a surgical intervention (such as a triple arthrodesis and calcaneocuboid arthrodesis) in tunnel syndrome patients with severe pes planus and foot deformities. 20 In our study, four of the patients with mini-open incisions and three of the patients with standard incisions exhibited those deformities. However, there was no need for additional surgeries in this study because none of the patients had severe foot deformities.
When considering the fact that pain and paresthesia begin or increase with variations in the foot position, Kinoshita et al. developed a test for the clinical diagnosis of tarsal tunnel syndrome. 7 During this test, while the ankle is at maximal dorsiflexion and eversion, the toes are extended. Immediately after placing the foot in this test position, there is pain, and a few seconds later, there is an onset of numbness. This technique is a reliable test for increasing the sensitivity of the clinical examination in a tarsal tunnel syndrome diagnosis. 7 This test was also used in the current study while diagnosing the patients (Table 1 ), but Tinel’s sign was used as the main clinical evaluation tool in the diagnosis and follow-up of the patients. This test was used to determine the success of the operation.
In 1996, Day and Naples described five cases with excellent results in which they performed endoscopic tarsal tunnel decompressions. They concluded that this technique was a good alternative to the classical open approach. 22 In 2006 and 2015, respectively, Krishnan et al. and Yoshida et al. reported endoscopic tarsal tunnel surgeries in limited case series as appropriate and less invasive procedures for the treatment of tarsal tunnel syndrome. 23,24 However, Yoshida et al. emphasized that ganglion and bony spur formation cases (such as tarsal coalition), which are the most frequent causes of tarsal tunnel syndrome, were not indicated for their procedure because complete decompression was not achieved in those cases. 24 Lui reported an endoscopic technique for the release of tarsal tunnel ganglions with the potential advantages of better cosmetic results, minimal dissection, and a reduced risk of perineural fibrosis, as well as the examination of the ganglion origin site and the arthroscopic treatment of any associated pathology. 25 Lui reported that the technique was contraindicated if there was an associated pathology of the tarsal tunnel that warranted open surgery, if the ganglion compressed the nerve from its superficial side, and if there was an intraneural ganglion of the tibial nerve. 25 However, no previous studies have reported a tunnel ligament release instrument assisted minimally open surgery as an alternative to the conventional open surgery.
Those studies that have reported endoscopic tarsal tunnel decompression approaches are very limited, and they require another specialization in this field. In this paper, we reported a mini-open incision technique using a tunnel ligament release instrument for tarsal tunnel decompression, and we compared the results of this technique to patients treated using a standard incision. Many previous carpal tunnel syndrome studies have compared the minimally invasive KnifeLight approach with the conventional open approach. 26– 28 However, none of them have reported its use in tarsal tunnel syndrome. In our paper, this technique presents an alternative to the usual standard incision technique, with a significantly decreased morbidity rate and increased cosmetic success. Similar to Yoshida et al., who emphasized that tarsal tunnel syndrome revisions, post-traumatic etiologies, and masses (ganglion cysts, lipomas, and venous anomalies) were contraindications for their endoscopic technique, these were also limitations of our short incision technique. 24
A major limitation of this study was that it was retrospective; therefore, it was prone to various forms of bias (selection bias and recall bias). Additionally, the number of patients was relatively low. However, the homogeneity between the groups was one strength of this study. Moreover, this was the first study to propose a mini-open incision technique using a tunnel ligament release instrument for tarsal tunnel decompression, with a purpose similar to the endoscopic decompression technique, and the advantages of limited soft tissue trauma and faster healing. Another limitation is that the study is multi-centered and the surgeries are performed by different centers.
Conclusion
This new mini-open incision technique to treat tarsal tunnel syndrome may be a good alternative to the standard incision, because it reduces the anesthesia time and provides a better cosmetic appearance. Prospective, randomized, controlled studies with broader patient populations are needed to further compare the effectiveness of this approach with conventional standard incisions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.