
Abstract
Objective:
This randomized controlled study was designed to compare the wound closure efficacy and safety of barbed suture in comparison to the conventional interrupted suture for total knee arthroplasty (TKA).
Methods:
This multicenter, single-blind, randomized controlled trial enrolled 184 patients who underwent elective TKA between June 2017 and April 2018. The subjects were randomized between two groups. Surgical incision closure time was considered as the primary end point.
Results:
A total of 184 patients participated in this randomized controlled trial; 91 patients had wound closure that involved barbed suture and 93 patients underwent conventional treatment—that is interrupted suturing with nonbarbed sutures. The surgical incision closure time was shorter (p < 0.0001) in the barbed suture group compared with the control group (15.5 ± 4.88 vs. 20.9 ± 6.30 min). However, both groups were found to be equal in terms of the rate of postoperative complications.
Conclusion:
Usage of the symmetric anchor designed barbed suture is safe, efficacious, and demonstrates a decrease in surgical incision closure time in patients undergoing TKA compared to interrupted closure using conventional sutures. Future studies are warranted to demonstrate clinical and economic benefits of barbed sutures.
Introduction
Over the past 20 years, the number of total knee arthroplasties (TKAs) conducted has been increasing due to the following factors: an aging population, the development of new diagnostic and surgical technologies, and continuous improvements in surgical instruments. 1 –5 While an ideal implant is crucial for the success of TKA, effective and secure wound closure techniques are essential to allow optimum wound healing, achieve acceptable cosmesis, and a reduced risk of adverse events (AEs), such as wound dehiscence and other complications. 6
Currently, interrupted suturing technique using nonbarbed sutures is used by most surgeons during TKA for closing surgical incisions in China. In comparison to the traditional continuous suture technique, the interrupted closure technique may improve suture strength to meet the needs associated with early functional exercise. Nevertheless, the interrupted technique has relatively low suture efficiency and may be associated with prolonged suturing and operative times compared to the continuous technique. Operative time reduction is associated with a diminished risk of complications, especially surgical site infection (SSI). 1
Antimicrobial sutures, such as VICRYL® Plus (Ethicon Inc., Somerville, NJ, USA) a triclosan-coated polyglactin 910 suture, have been proven to be effective in preventing SSIs and were developed to address the unmet need of SSI by protecting the sutures against colonization. It’s quite recent that this technology has been added on to barbed sutures.
Barbed sutures have been considered good alternatives over conventional sutures. Since their invention, barbed sutures have been used in various specialties, including cosmetic, urologic, general, obstetric and gynecologic, and orthopedic operations. The main advantages of barbed sutures are the lack of knots, a secure approximation of tissues with an equal distribution of tissue strength and tension, and its association with a favorable learning curve and reduced wound closure time. 7,8 Barbed sutures do not require an assistant to apply tension to the suture thread as the tissues are being apposed.
Examples of orthopedic procedures where barbed sutures have been used include total joint arthroplasty, including total hip arthroplasty (THA) and TKA. 9 –12 Based on the results of multiple meta-analyses, barbed sutures were found to be an effective tool in surgeries when compared with conventional sutures, yielding shorter operative times leading to cost-effectiveness and similar rates of wound complications. 6,12 –15 Furthermore, the presence of barbs securely anchors the tissue, without allowing the suture to slide back. This leads to a uniform distribution of tension along the suture line which was found to lead to less complications, such as wound dehiscence and hematomas. 5,15 –21
The symmetric anchor designed barbed suture (SADBS; STRATAFIX™ Symmetric PDS™ Plus, Ethicon Inc.) is an antibacterial, monofilament, barbed suture constructed from polydioxanone. This product contains triclosan—a broad-spectrum antimicrobial agent. Sutures coated with triclosan have been proven to have a lower risk of SSI and are recommended by the World Health Organization (WHO), 22 the American College of Surgeons (ACS), 23,24 and the Centers for Disease Control and Prevention (CDC). 25 –27 With the increased surface area that barbed sutures possess and the propensity to trap fibers/gauze, the risk for infection is increased so an antimicrobial coating is necessary. 28 –30 SADBS has a unique symmetric anchor barbed design (Figure 1), which is different from the other available barbed sutures and allows surgeons to perform highly efficient continuous suturing and may improve operative efficiency. Nevertheless, this is a relatively novel product and more studies are required to confirm its safety and efficacy.

The symmetric anchor designed barbed suture.
The aim of this study is to evaluate the wound closure effectiveness and safety of SADBS in comparison to the conventional interrupted technique using nonbarbed sutures for TKA.
Materials and methods
Study design and patients
This prospective, multicenter, single-blind, randomized controlled trial (NCT03305887) was conducted in accordance with the International Council of Harmonization Guideline for Good Clinical Practice (1996), the Declaration of Helsinki (2008), China Food and Drug Administration Regulations, Regulations on the supervision and administration of medical devices (State Council Decree No. 650), Guideline for Chinese Good Clinical Practice (CGCP), as well as any other applicable local regulatory requirements. This study was approved by the Ethics Committee in all participating hospitals.
The study included 184 eligible patients treated at seven hospitals in China (Figure 2; Table 1), who underwent elective TKA from June 2017 to April 2018. The inclusion criteria were (1) 18–79 years of age; (2) scheduled to undergo elective unilateral TKA for osteoarthritis; (3) willing to participate in the study, comply with the protocol, and give written informed consent; and (4) agreed to no additional elective surgeries until the end of this study. The exclusion criteria were (1) pregnancy or lactation; (2) body mass index >40 kg/m2; (3) inability to walk independently (inability to walk at least 10 consecutive meters without a walking aid); (4) history of surgical intervention during the past 30 days for treatment of joint pain or its underlying etiology; (5) previous open surgery on the affected joint other than arthroscopy; (6) active collagen diseases (i.e., scleroderma) or any other conditions that would interfere with wound healing; (7) hypersensitivity to poly (p-dioxanon), triclosan, or D&C Violet No. 2; (8) uncontrolled diabetes (fasting plasma glucose ≥10.0 mmol/L); (9) history of immunosuppressive drug use, including steroids, within the last 6 months; (10) history of chemotherapy or radiotherapy within the last 6 months before enrollment or scheduled for chemotherapy or radiotherapy during the study period; (11) personal or family history of keloid formation or scar hypertrophy; (12) dermatologic conditions known to impair wound healing; (13) participating in any other clinical trials of drug (within 30 days or 5 half-lives of a study drug) or medical device; (14) any physical or psychological condition which would impair study participation; or (15) unsuitable to participate in the study for any other reasons, as judged by the investigator.

Patient flowchart.
Enrollment in each site.

SADBS: symmetric anchor designed barbed suture.
Randomization and surgery
The patients were randomized into either SADBS group or the conventional interrupted suture group. A central randomization system was used. Patients were blinded to the type of wound closure suture used.
The wound closure was performed according to the site requirements or specific guidelines, and with a surgical approach. 31 –35 For patients assigned to the SADBS group, the deep and intermediate layers were repaired and closed continuously using STRATAFIX Symmetric PDS Plus. For patients assigned to receive conventional sutures, CR8 VICRYL® Plus was used to close the deep and intermediate layers via the interrupted technique. For both groups, the STRATAFIX Spiral PGA-PCL Knotless Tissue Control Device was used to close the intradermal layer with continuous technique and the DERMABOND™ Advance™ Skin Closure System was applied for skin closure (Table 2). Postoperative care and range of motion (ROM) exercises were performed according to standard of care at each site.
Suture material and technique in two groups.
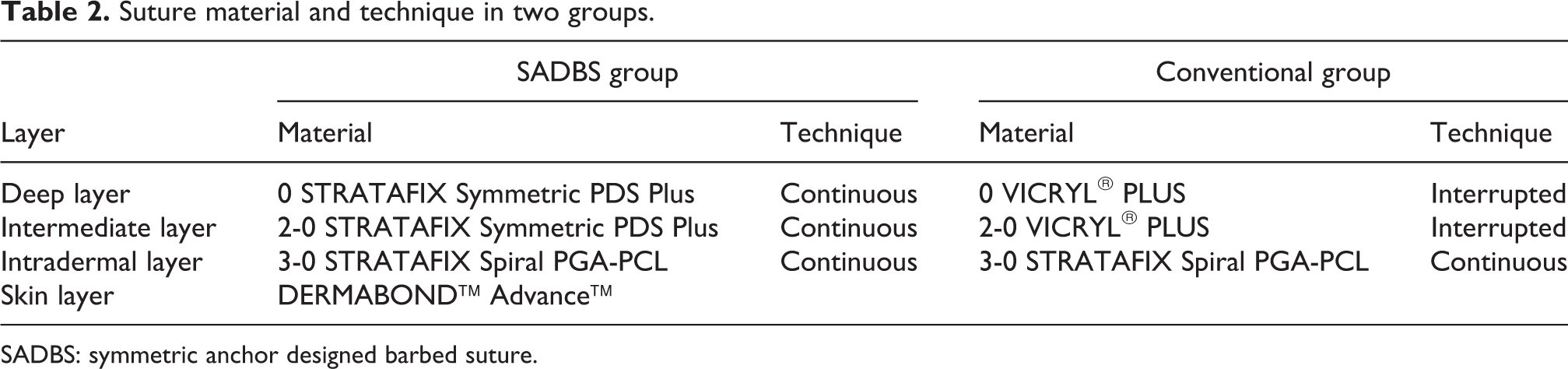
SADBS: symmetric anchor designed barbed suture.
End points
The primary end point was the surgical incision closure time, which was defined as time in minutes between the start of the first suture throw placed in the deep tissue and the completion of intradermal layer closure (capturing the suturing time only). The secondary efficacy end points were operative time (defined as the start of the first incision to the completion of skin closure), total operating room time (defined as the time from anesthesia to exiting the operating room), length of stay (defined as the time from surgery to discharge), knee pain, ROM of knee, and health-related Quality of Life (QoL). The secondary safety end points were SSI incidence, Additional treatment, Serous discharge, Erythema, Purulent exudates, Separation of deep tissues, Isolation of bacteria, Stay in hospital prolonged over 14 days (ASEPSIS) score, Acute Inflammatory Response Evaluation (AIRE) score, wound separation or dehiscence requiring intervention, delayed wound healing, wound closure-related AEs, and wound closure-related serious AEs (SAEs).
Follow-up
Patients were followed up during hospitalization and 30–42 days after operation. Knee pain at rest and motion were assessed using a 10-point visual analogue scale (VAS), with higher score indicating greater pain. Health-related QoL was assessed using Euro QoL five-dimensions-three-level questionnaire, which consists of a descriptive system that assesses QoL based on five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Patients were asked to answer each dimension at three levels: no problem, moderate problem, or extreme problem. Each combination of answers to the questionnaire was converted into a summary score, with a higher score indicating better QoL.
SSIs were recorded according to the criteria set by the CDC. 36 The ASEPSIS score, used to assess a wound based on the appearance of the wound over the first week after surgery and on the clinical consequences of infection, was assessed only in patients with confirmed SSI. 37,38 AIRE score was assessed based on erythema, edema, pain, and temperature. 39
AEs, SAEs, adverse device effects, and serious adverse device effects were recorded and classified according to the Medical Dictionary for Regulatory Activities (MedDRA) 21.0.
Statistics analysis
This was a superiority trial. The sample size calculation was based on a review of the literature, 5,16 –19 and the mean incision closure time for conventional interrupted sutures was generally calculated to be 16.9 min. It was expected that the SADBS can reduce the wound closure time by 25% (12.7 min) when compared to conventional interrupted sutures. The standard deviation (SD) for this study, thus, was conservatively assumed to be 8 min in both groups. 5,16 –19 A total of 77 patients per arm achieved 90% power to detect the expected difference in means of 4.2 min, using a one-sided two-sample t-test with a one-sided significance level of 0.025. The sample size was adjusted to 92 subjects per arm to account for a drop-out rate of 16%. 40 –43
The primary end point was analyzed using both As-Treated (AT) and per-protocol (PP) sets. All secondary efficacy end points were summarized descriptively in the AT set. All secondary safety end points and AEs were summarized descriptively in the safety set. No imputations for missing data were performed. No inferential statistics were generated for the secondary end points. SAS 9.4 (SAS Institute, Cary, NY, USA) was used for statistical analysis. Continuous variables were expressed as mean ± SD. Categorical variables were expressed as count and frequency (percentage). If the upper bound of the confidence internal for the difference in the treatment group’s mean surgical incision closure time was less than 0, then it was concluded that the SADBS was superior to conventional interrupted suture.
Results
Characteristics of the patients
A total of 185 patients were recruited between June 2017 and April 2018. One patient was excluded because of a history of previous open knee surgery. As a result, 184 (99.5%) patients were randomized either to the SADBS group (n = 91) or the conventional suture group (n = 93). Finally, the AT included 90 patients in the SADBS group and 89 in the conventional group. The baseline patient characteristics are summarized in Table 3. A total of 163 (88.1%) subjects have completed the study, with 80 (87.9%) subjects in the SADBS group and 83 (89.2%) subjects in the conventional suture group. Lost to follow-up (n = 11, 5.9%) and withdrawal of consent (n = 6, 3.2%) were the primary reasons for early termination. Study discontinuation occurred in 2 (1.1%) subjects due to protocol deviation and 3 (1.6%) subjects due to other reasons. The patient flowchart is shown in Figure 2 and the disposition of enrolled subjects by treatment group is summarized in Table 4.
Demographics and baseline characteristics—AT set.a

BMI: body mass index; VAS: visual analog scale; ROM: range of motion; SADBS: symmetric anchor designed barbed suture; AT: As-Treated.
a Data are shown as mean ± standard deviation or n (%).
bTwo-sample t-test (equal variance).
cChi-square test.
Disposition of enrolled subjects by treatment group.a

SADBS: symmetric anchor designed barbed suture.
a Percentages were based on the number of enrolled subjects in total or each treatment group. Enrolled subjects were the subjects who signed the informed consent.
b One patient withdrawn the consent before randomization.
Wound closure time
The surgical incision closure time for each group is represented in Table 5. The difference between wound closure time (15.5 ± 4.9 vs. 20.9 ± 6.3 min) was statistically and significantly different (one-sided upper 97.5% confidence bound: −3.69 min in the AT analysis) between the SADBS group compared and the conventional suture group in both AT set and PP analyses.
Surgical incision closure time—AT set.

SD: standard deviation; SADBS: symmetric anchor designed barbed suture; AT: As-Treated.
aTwo-sample t-test (unequal variance).
Secondary efficacy results
As presented in Table 6, the length of incision, anesthesia methods, operative time, total operating room time, knee ROM, and length of stay were similar between the two groups.
Intraoperative events and secondary end points.a
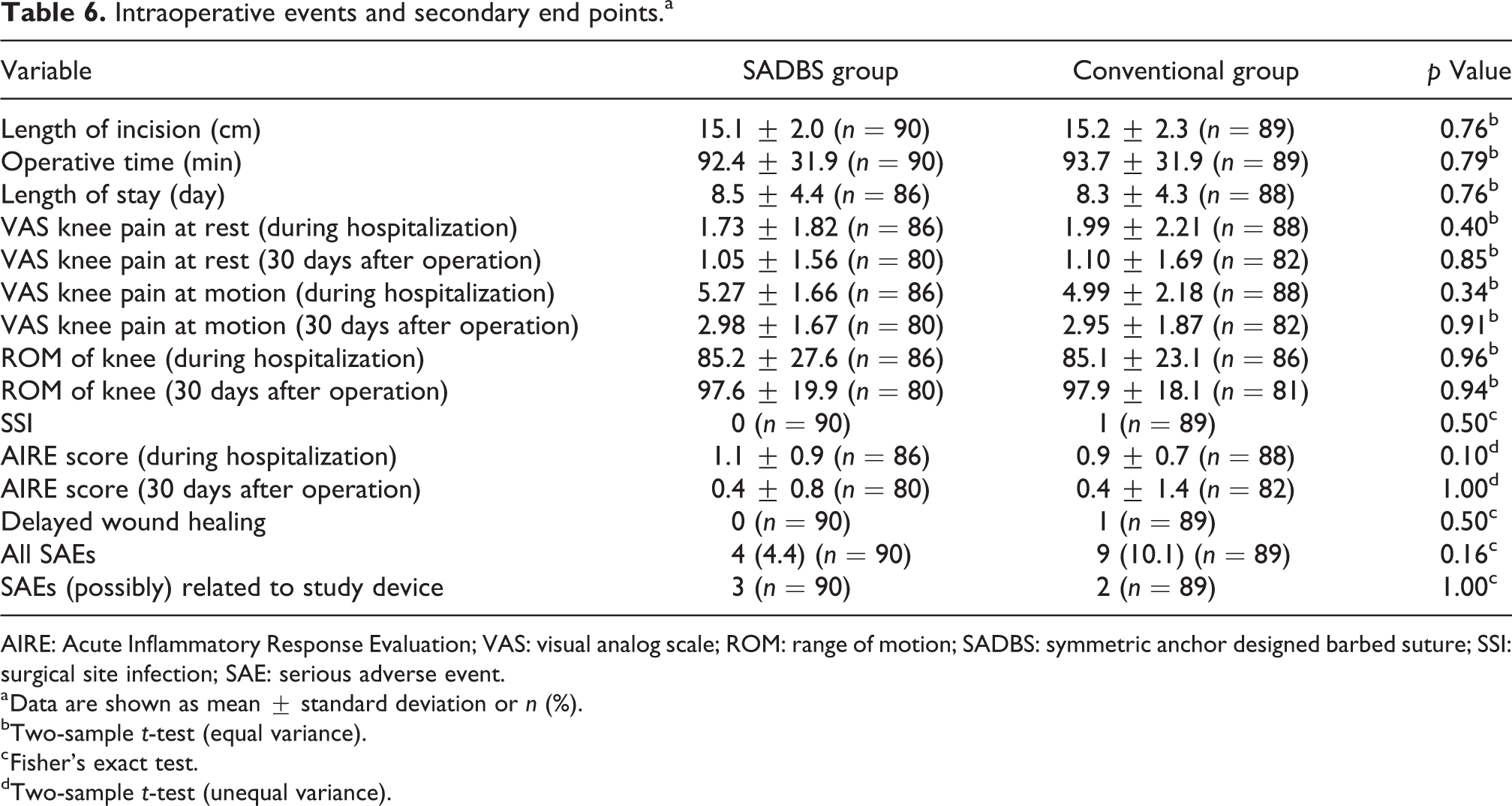
AIRE: Acute Inflammatory Response Evaluation; VAS: visual analog scale; ROM: range of motion; SADBS: symmetric anchor designed barbed suture; SSI: surgical site infection; SAE: serious adverse event.
a Data are shown as mean ± standard deviation or n (%).
bTwo-sample t-test (equal variance).
c Fisher’s exact test.
dTwo-sample t-test (unequal variance).
Safety results
All the safety results are also summarized in Table 6. The SSIs, ASEPSIS score, AIRE score, incidence of wound separation or dehiscence requiring intervention, incidence of delayed wound healing, wound closure-related AEs, and wound closure-related SAEs were similar between the two groups. SAEs were reported by 4 (4.4%) SADBS and 9 (10.1%) conventional suture subjects. Furthermore, SAEs (possibly) related to study device were reported by 3 (3.3%) SADBS and 2 (2.2%) conventional suture subjects. In SADBS group, the three device-related events were postoperative pain and two wound drainage; in conventional group, the events were wound drainage and SSI. The subject from conventional suture group involving SSI was considered possibly related to the study device (VICRYL® Plus). The patient was a 68-year-old female who underwent TKA and developed a confirmed SSI 28 days operatively by knee synovial fluid cultures. The pathogen detected was methicillin-resistant Staphylococcus aureus (MRSA). After revision surgery and antibiotics, the event was resolved.
Discussion
This study demonstrated that SADBS may significantly reduce surgical incision closure time in comparison with conventional interrupted sutures. Using the AT analysis, SADBS was shown to be superior to conventional sutures, with a mean difference of −5.35 ± 5.63 min. The one-sided upper 97.5% confidence bound was −3.69 min, which is smaller than 0 and is, therefore, statistically significant (p < 0.0001). In terms of the PP analysis set, the difference in mean closure time between SADBS and conventional sutures was −5.16 ± 5.66 min. The one-sided upper 97.5% confidence bound was −3.47 min, further reiterating the superiority of the SADBS compared to conventional sutures in shortening wound closure time.
SADBS eliminates the need to tie surgical knots. This may explain how it reduces operative time and other potentially related complications such as, hemodynamic instability. 44 The same conclusions can be drawn from a randomized control trial performed by Sundaram et al. 45 where 60 patients who undergone TKA were assigned to receive either running closure of the arthrotomy with barbed sutures (n = 30) or interrupted closure with standard-of-care sutures (n = 30). Arthrotomy closure time was significantly shorter in the barbed suture group (3 ± 2 min) compared to the standard-of-care sutures (13 ± 5 min, p < 0.001) in patients who underwent TKA (n = 60). 45 The average arthrotomy closure was one suture (range = 1–2) versus three sutures (range = 2–4) in the standard-of-care group (p < 0.001). In addition, there were no reports found in the barbed sutures group (0/30) of superficial SSI in comparison to the 30% (1/30) in the standard-of-care group (p = 1.00). Similar results were reported in a study conducted by the same authors in patients who had THA. 46 Results showed that arthrotomy closure was significantly shorted in the barbed suture group (3 min ± 9 s) versus the standard-of-care group (8 min ± 16 s, p < 0.001). Interestingly, the suture utilization for arthrotomy closure was one suture (28/30, 30%) in the barbed suture group versus two to four sutures (27/30, 90%) in the standard-of-care group (p < 0.001). One patient (3%) suffered suture abscess postoperatively in the barbed suture group (p = 1.00). Meanwhile, trochanter bursitis was reported in one patient (3%) in the standard-of-care group (p = 1.00). Overall, the number wound-related complications were equivalent in both treatment groups (p = 1.00). 46 All in all, barbed sutures demonstrated better arthrotomy closure times with less complications compared to standard-of-care sutures.
Like many other surgeries, TKA requires the use of sutures that reduce operating time, wound closure time, and cost, due to the delicate nature of the knee anatomy. 47 TKA requires fast wound closure to reduce superficial and serious infections. Therefore, the use of barbed sutures without knots may be ideal during TKA due to the speed of wound closure. The knot is the weakest point of a suture. 48 As opposed to conventional sutures’ reliance on the knot, barbed sutures, with its knotless design, allow shorter wound closure time, hence possibly reduced infection risk and improved cost-effectiveness. 47 In a meta-analysis of studies on barbed versus conventional sutures, Lin et al. concluded that the orientation of the barbs in relation to the needle allows barbed sutures to appose tissues. 12,45,46 It was found that although barbed sutures reduced suture time (standardized mean difference (SMD) = −0.95, 95% CI: −1.43, −0.46, p = 0.0001) and operative time (SMD = −0.28, 95% CI: −0.46, −0.10, p = 0.003), its use increased the incidence of complications (OR = 1.43, 95% CI: 1.05, 1.96, p = 0.03), 12,45,46 but in our study, the incidence of both AEs and SAEs is similar in two group and the use of SADBS did not increase the incidence of complications.
The design of the SADBS also allowed stronger suture initiation compared with the conventional threads. 9 Since the knot is the weakest point of a suture, 48 its presence may affect wound integrity significantly. 49 Finally, the SADBS did not show higher wound holding strength compared with the conventional 2-0 thread for subcutaneous tissues, but it showed a higher holding strength for musculotendinous tissues. 49 According to Borzio et al., barbed sutures were found to be superior compared to conventional sutures in terms of wound closure time (6.3 min faster, p < 0.05), which also translated to cost savings. 16
The present study, similarly, demonstrated that SADBS is superior to conventional sutures in reducing the surgical incision closure time and difficulty in patients with TKA. 39
The secondary efficacy end point results were similar between the two groups (Table 6). In the present study, no SSIs were reported in the two groups during the fourth visit, and one SSI was reported, however, during the fifth visit in the conventional sutures group. This SSI had an ASEPSIS score of more than 40, indicating that it was a severe wound infection. The small difference in the secondary end points can possibly be attributed to the use of proper aseptic techniques during arthroplasty. 26,50
In addition, the VAS knee pain, QoL, ROM of knee, SSI, and wound healing parameters were similar between the two groups. This is probably due to the low rate of SSI observed in the present study. Two meta-analyses and a more recent randomized controlled trial showed that the complication rates were similar between the barbed and conventional sutures for laparoscopic hysterectomy, C-section, arthroplasty, gastric bypass, and sacrocolpopexy, 12,16,45,46,51 supporting the conclusions of the present study. However, a study by Chawla et al. 30 reported concerns that barbed sutures caused more infections possibly attributed to overtightening. Its noteworthy that the use of barbed sutures by itself did not increase the risk of infections in the present study. The reason for the low occurrence of SSI in the groups could be attributed to the fact that both the sutures groups were Triclosan coated. This is in addition to extremely low rates of infection in TKA procedures. 52
Overtightening may predispose tissue to ischemic necrosis. Dead tissue then becomes a foci for secondary infections. 30 On the other hand, a prospective study conducted by Aliano et al. showed that standard sutures increase the risk of tissue ischemia due to increased tension at knotted loops compared to barbed sutures. 44,53 –55 Furthermore, excessive pressure within the tissue can produce enzymatic degradation which induces loss of wound strength and higher incidence of wound dehiscence. 54,56,57 Consequently, tight suturing has demonstrated compromised blood flow and consequent tissue necrosis. 54,58 This information was echoed in the randomized studies performed by Gililland et al. and Chan et al. 5,51 The authors stated that knots may place uneven pressure on the tissue leading to ischemia, while the absorption of bulky knots may cause local tissue inflammation and scaring. This may result in a potential nidus of infection and wound dehiscence. 5,51 As barbed sutures do not require knots because of their self-anchoring design, tissue tension is evenly distributed which may lower the risk of local tissue ischemia. Reducing tissue trauma and utilizing tension free closure may increase blood flow and improve wound healing. 59
In a study by Cortez et al., 60 barbed sutures were found to be associated with higher rates of wound complications. However, this is still dependent on technique and more studies may need to be conducted to have this risk established. 60 It is also important to note that the present study was not designed to detect SSIs. Despite the absence of identified SSIs, other studies have shown that the infection risk ratio is not decreased when using barbed sutures. 30,60 As mentioned earlier in our study, no SSI has been observed in the SADBS group. Since the study was not designed to make claims related to the SSI rate, our results cannot refute the findings in the study by Chawla and Cortez, but they highlight that SADBS coated with triclosan might be better suited for these applications especially in light of recommendations by WHO, ACS, and CDC against SSI.
SADBS has been found to display antibacterial properties as a result of triclosan. Bhende et al., 61 in an in vitro study evaluating the SADBS while being subjected to contaminated wound conditions, found that the utilization of the suture exhibited antibacterial activity against S. aureus, MRSA, Escherichia coli, S. epidermis, and Klebsiella pneumoniae. Here, the control and test articles were placed subcutaneously in the same animal, which was then inoculated with bacteria. The activity against S. aureus and E. coli persisted for up to 3 weeks. 61 The authors also concluded that the SADBS, apart from the inherent benefits of barbed sutures, was also a valuable adjunct in reducing the risk of SSIs. 61
Theoretically, the overall operative time of SADBS group was expected to be shorter. However, the results were similar, which could be attributed to the 5-min differences in wound closure time between the two groups, which was further diluted by an operative time >90 min. In another study by Sutton et al., barbed sutures were also found to be superior to conventional sutures in terms of shorter length of hospital stay after knee or hip arthroplasty (knee = 0.2 days, hip = 0.3 days) and operating time (knee = 7 min, hip = 22 min). 45,46,62 The results of that study support the superiority of barbed sutures over conventional sutures, especially in terms of knee arthroplasty. 62 From a cost perspective, 182 pouches of SADBS (2 pouches per subject) and 315 pouches of VICRYL® Plus (3.4 pouches per subject) were used in this study. The average price in China of SADBS is about US$85 per pouch and US$31 per pouch for VICRYL® Plus, so the cost of sutures in SADBS group is US$170 and US$105.4 for conventional group. It is difficult to comment whether the time savings reported in the current study justifies the additional expense incurred for SADBS and this could be a focus for future studies.
The other adverse event rates were consistent with the expected rates of adverse events as reported in other studies. 12,16,49 This therefore supports that SADBS is comparable in safety and efficacy to other sutures and is associated with a shorter wound closure time.
This study has several limitations. The postoperative follow-up period was short and the long-term outcomes could not be observed. Additional studies are still necessary to elaborate the cost benefits and safety of the SADBS for TKA more comprehensively.
Conclusion
The SADBS reduces the wound closure time when used during TKA compared with conventional interrupted sutures. The results suggest that the SADBS can be an effective and safe alternative to traditional wound closure methods. However, more studies need to be conducted comparing SADBS with conventional sutures to establish its safety and efficacy beyond TKA and in larger or more diverse populations.
Footnotes
Author contribution
Wei Wang, Shigui Yan, and Feng Liu contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by Ethicon, Inc. and Johnson & Johnson Medical (Shanghai) Ltd.