
Abstract
Background:
Previous studies about antibiotic prophylaxis in foot and ankle surgery have focused on perioperative intravenous administration, with few studies reporting on the efficiency of postoperative oral antibiotics. The purpose of this study is to investigate differences in the rate of postoperative infection and wound complications between patients with and without postoperative oral antibiotics and to identify independent risk factors for these complications following foot and ankle surgeries.
Methods:
A retrospective review of all elective foot and ankle surgeries with at least a 6-month follow-up was performed over a 2-year time span. Patients were divided into 2 groups based on if they received postoperative oral antibiotics. We compared the rates of postoperative infections and wound complications between the 2 groups. The surgical site, the number of Current Procedural Terminology codes, and the number of surgical incisions were also noted. Multivariable logistic regression analysis was performed to identify independent risk factors of postoperative infection and wound complications.
Results:
A total of 366 patients were included in this study—240 with antibiotics and 126 without antibiotics. There was no significant difference in the rates of postoperative infection and wound complications between the 2 groups. The rate of superficial infection, deep infection, and wound complications was 1.7%, 0.8%, and 5.8% in the antibiotic group vs 3.2%, 0.0%, and 4.0% in patients without antibiotics, respectively. Multivariable logistic regression analysis identified independent risk factors of postoperative infection and wound complications as follows: smoking (OR: 4.7), male (OR: 4.0), history of neoplasm (OR: 6.7), and multiple incisions (OR: 4.1).
Conclusion:
Our results suggest that routine postoperative prophylactic oral antibiotics are not needed following elective foot and ankle surgeries. However, certain risk factors may increase the risk for postoperative infection and wound complications in foot and ankle surgery.
Level of Evidence:
Level III, case-control study.
Keywords
Introduction
Previous studies have reported that the rates of postoperative infection in foot and ankle surgery range from 0.5% to 6.5%.9,15,24 Surgical site infections (SSIs) can range from being minor, requiring a course of oral antibiotics, to major, requiring a return trip to the operating room with intravenous antibiotic management. Costs of managing this complication ranges from $400 to $30 000 depending on the severity of the infection. 29
Recommendations in prophylactic postoperative oral antibiotics for patients undergoing foot and ankle surgery are not universal. A 2014 survey showed that 52% of foot and ankle surgeons never prescribe prophylactic oral antibiotics. Of providers who prescribe postoperative oral antibiotics, there is no universal agreement for the type of antibiotics and the dosages or the durations of these postoperative antibiotic prescriptions. 24 Many studies about antibiotic prophylaxis in foot and ankle surgery have focused on the preoperative administration of intravenous antibiotics and the immediate postoperative period before hospital discharge rather than postoperative oral antibiotics.2,7,17,28 Despite the amount of literature on perioperative antibiotics on postoperative infections, there are only a few studies focusing on postoperative oral antibiotics following foot and ankle surgeries.6,8,24
The purpose of this study is 2-fold. The first is to investigate differences in the rates of postoperative infection and wound complications between patients who received postoperative oral antibiotic prophylaxis and patients who did not. The second is to identify independent risk factors of postoperative infection or wound complications following elective foot and ankle surgeries through a multivariable logistic regression analysis.
Materials and methods
After obtaining institutional review board (IRB) approval, we performed a retrospective chart review over a 2-year time span. Inclusion criteria included all elective foot and ankle cases, ages ≥18 years, and at least 6 months of postoperative follow-up. Patients were excluded if they had any evidence of preoperative wounds or infections, and patients with Charcot. Ultimately, 366 patients met inclusion criteria. These patients were divided into 2 groups based on if they received postoperative oral antibiotics.
All patients received perioperative antibiotics, most commonly cefazolin. Clindamycin or vancomycin was used in patients with a cefazolin allergy. The perioperative antibiotic was given prior to surgical incision tourniquet inflation in all patients. The default postoperative oral antibiotic was cephalexin, and clindamycin was used in patients with cephalexin allergies. Notably, cephalexin was used in the majority of cases (84.2%, 202/240), and followed by clindamycin (15.0%, 36/240). In the study period, the standard duration for postoperative oral antibiotics was 7 days. In patients who had hindfoot surgeries, a thigh tourniquet was used, and in patients who had forefoot or midfoot surgeries, a calf tourniquet was used.
Demographic data included age, sex, race, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, smoking status, history of diabetes mellitus (DM), history of rheumatoid arthritis (RA), hypertension (HTN), history of thyroid condition, and history of neoplasm. Surgical sites (hindfoot vs other than hindfoot), the number of Current Procedural Terminology (CPT) codes, and the number of incisions made in surgery were also noted. Stab incisions for percutaneous screw insertion and arthroscopic portals were not counted as incision sites.
Infections were classified as superficial infections or deep infections. Superficial infection was defined as skin or subcutaneous issues with erythema, and swelling that required oral antibiotics prescribed at follow-up. Deep infection was defined as an infection including the muscle or fascia requiring a return to the operating room for operative debridement. Wound complications were defined as any wound dehiscence or delayed healing, but without signs of infection such as redness, swelling, or a heating sensation, and requirement of oral antibiotics.
We compared the demographic data between the groups as well as their respective rates of postoperative infections and wound complications. Furthermore, the patients were also divided into those who had a postoperative infection or wound complications (n = 29) and those who did not (n = 337). We compared the demographic variables between these groups to see if there were any risk factors for postoperative wound infection and wound complications. A multivariable logistic regression analysis was performed with possible risk factors of postoperative infections and wound complications. The variables included in this regression analysis were decided by the results of this study as well as the results from previous studies.5,6,8,24 Some cases included multiple procedures, surgeries combined with forefoot, midfoot, and hindfoot as well as arthroscopy. We simplified the surgical site as hindfoot vs other than hindfoot. If the case was combined with any hindfoot procedure, the surgical site was considered hindfoot.
Statistical Analysis
All statistical analyses were performed with SPSS software (version 21.0; IBM, Armonk, NY, USA). Data are presented as the mean and SD. Continuous variables such as age and BMI were compared using Student t test, and categorical variables were compared using chi-square test or Fisher exact test. Variables that can have an effect on postoperative infection and wound complications were investigated, and they were included in a multivariable logistic regression analysis to identify independent predictors of postoperative infection and wound complications following elective foot and ankle surgeries. The level of statistical significance was set as P <.05.
Results
There were 366 patients in this study—240 were with postoperative oral antibiotics and 126 without postoperative oral antibiotics. No significant differences in patients’ demographics were noted between the 2 groups (Table 1).
Patient Demographics.
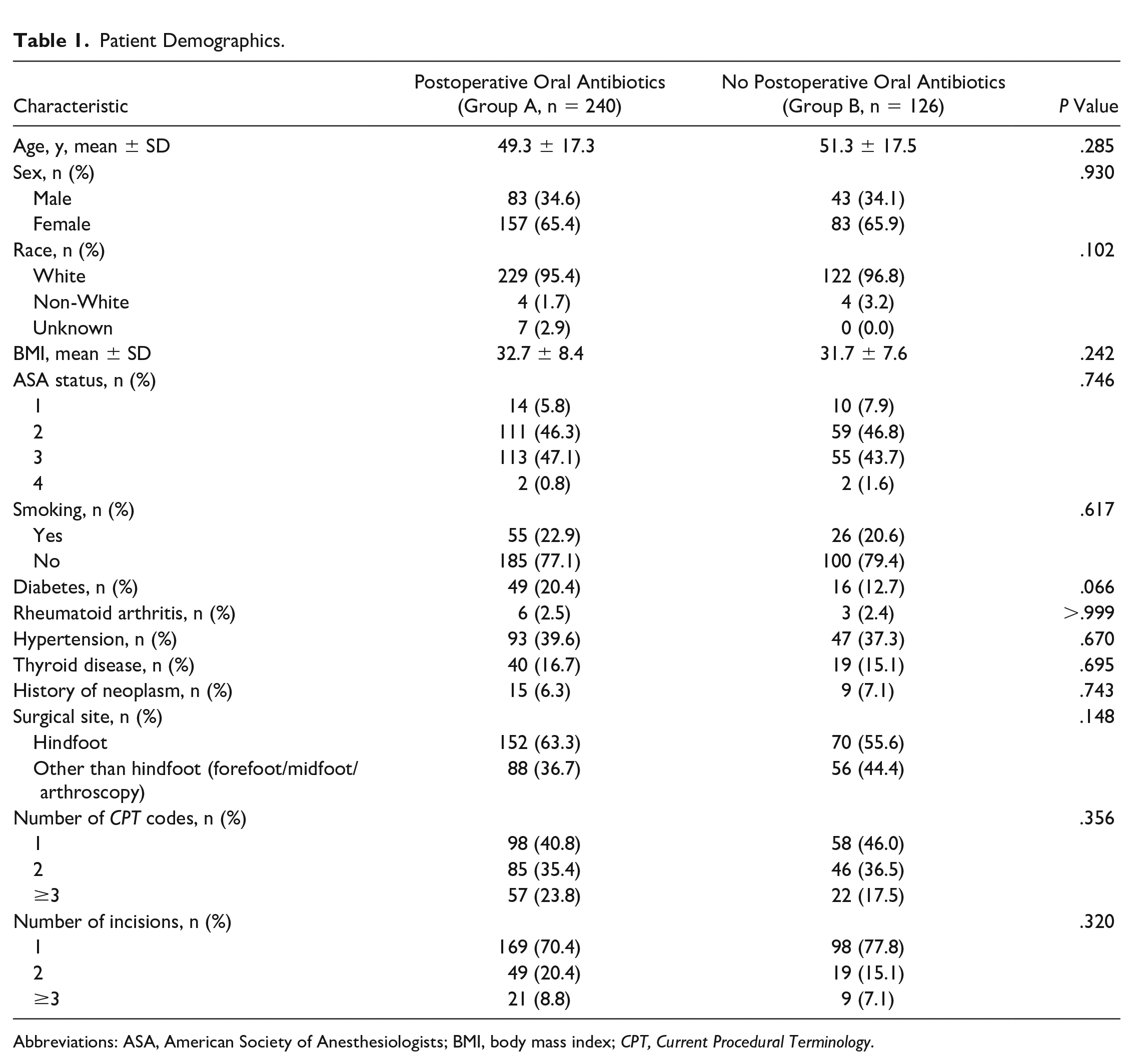
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CPT, Current Procedural Terminology.
There was no significant difference in the rate of postoperative infection or wound complications between the 2 groups (Table 2). The rate of superficial infection, deep infection, and wound dehiscence was 1.7%, 0.8%, and 5.8% in the antibiotic group vs 3.2%, 0.0%, and 4.0% in patients without antibiotics, respectively.
The Rates of Postoperative Infection and Wound Complications Between the 2 Groups.

Table 3 demonstrates the demographic comparison between the postoperative infection or wound complication group and the nonpostoperative infection or wound complication group. There was a statistically significant difference between the number of males and females in each group (P = .004), as well as the smoking history (P = .002), history of neoplasm (P = .007), and the number of incisions (P = .002).
Demographic Comparison Between the Groups With and Without Postoperative Infection and Wound Complications.
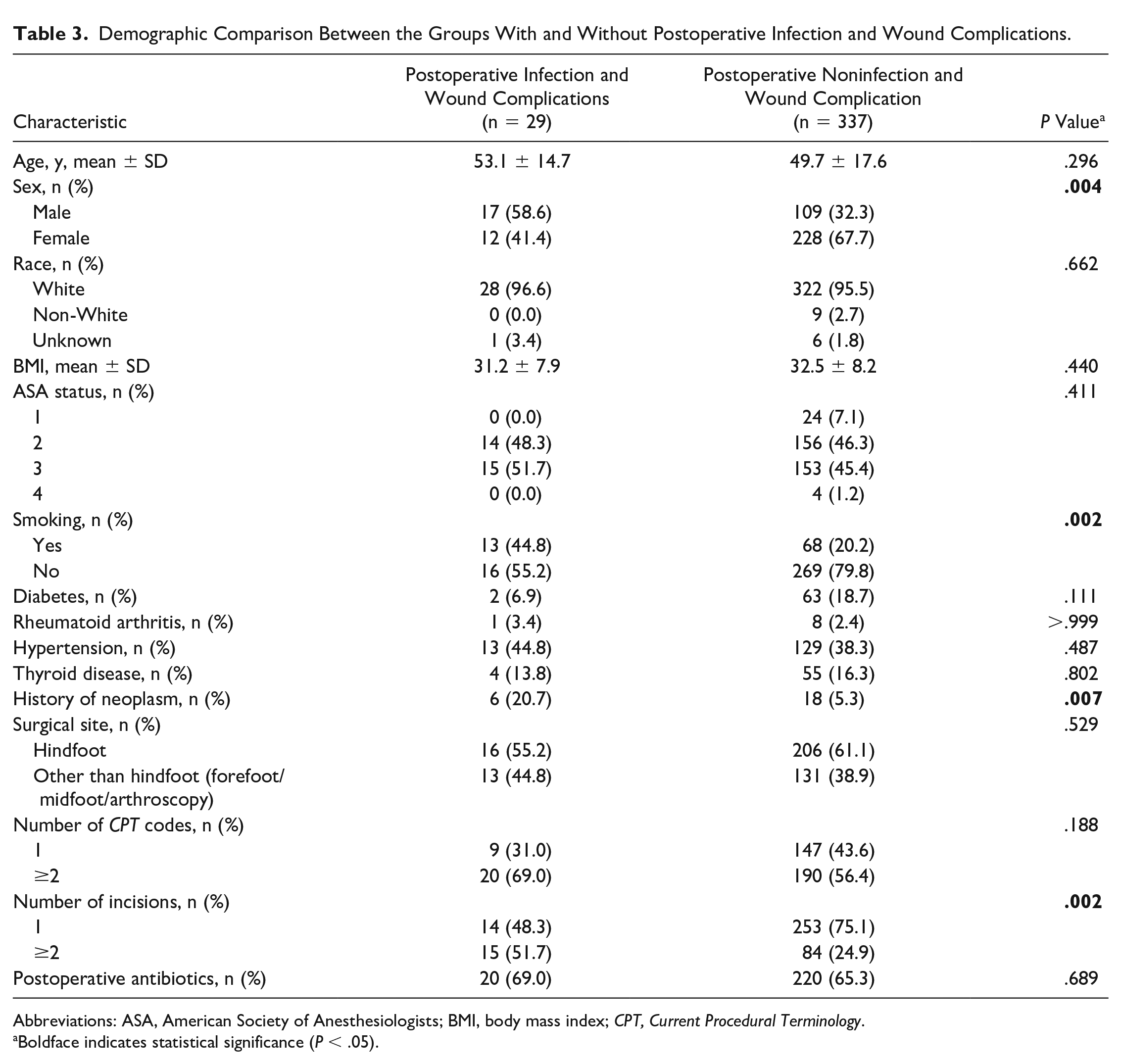
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CPT, Current Procedural Terminology.
Boldface indicates statistical significance (P < .05).
As one of the purposes of this study was to identify independent risk factors of postoperative infection and wound complications following foot and ankle surgeries, a multivariable logistic regression analysis was conducted (Table 4). Smoking (OR 4.668, 95% CI 1.937, 11.253), male sex (OR 3.959, 95% CI 1.678, 9.343), history of neoplasm (OR 6.664, 95% CI 2.044, 21.732), and multiple incisions (OR 4.138, 95% CI 1.740, 9.836) were identified as independent risk factors of postoperative infection and wound complications.
A Multivariable Regression Analysis Investigating Risk Factors for Postoperative Infection and Wound Complications.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CPT, Current Procedural Terminology; DM, diabetes mellitus; HTN, hypertension.
Boldface indicates statistical significance (P < .05).
Discussion
Overall, this investigation found no significant difference in the rates of postoperative infection and wound complications between patients managed with and without postoperative oral antibiotics, which is comparable to the findings from the previous studies.6,8 Multivariable logistic regression analysis identified that patients who were male, a smoker, had a history of neoplasm, and had multiple incisions during their surgery were more likely to develop postoperative infection or wound complications following elective foot and ankle surgeries.
The use of prophylactic postoperative oral antibiotics in foot and ankle surgery remains common, but without absolute guidelines. Although there are many studies investigating the effect of perioperative antibiotics on postoperative infections, only a few studies focused on postoperative oral antibiotics following foot and ankle surgeries.6,8,24 Ruta et al 24 conducted a survey of 312 American Orthopaedic Foot & Ankle Society members that reported 75% of surgeons used prophylactic postoperative oral antibiotics. However, 69% of those surgeons prescribe them for less than 25% of patients. The most common regimen was cephalexin 500 mg 4 times per day for 5-7 days. Indications for prophylactic postoperative oral antibiotics most commonly included previous infection, medical comorbidities, and previous wound healing difficulties. There were no reported differences in SSI rates between those who were prescribed postoperative oral antibiotics and those who were not. 24 There are a few other studies that have examined postoperative oral antibiotics following elective foot and ankle surgery. Carl et al 6 performed a retrospective review of 649 patients and found that the postoperative infection rate in patients who received postoperative prophylactic oral antibiotics was 3% vs 2% for those who did not, which was not a statistically significant difference. No differences in the rates of deep vs superficial infections or delayed wound healing between these 2 groups was detected. 6 Furthermore, Frederick et al 8 performed a retrospective chart review of 3631 patients and found no statistically significant difference in infection rate or severity of infection between patients who received postoperative oral antibiotics and patients who did not.
Previous studies demonstrated several risk factors of postoperative infection after foot and ankle surgery. Wiewiorski et al 30 showed that age >60 years was a risk factor for wound healing following elective foot and ankle surgery, with older patients being more likely to develop an infection. Carl et al 6 also found that patients who experienced postoperative infection were significantly older than those who did not: 55 years vs 45 years. Our data set demonstrated that patients who developed a postoperative infection and/or wound complications were an average of 3.4 years older; however, it was not a statistically significant difference. Further, Butterworth et al 5 found no difference in age of patients sustaining a postoperative infection following foot and ankle surgeries. It still remains unclear if age is a significant factor for the development of a postoperative infection after foot and ankle surgery, but explanations potentially including impaired immunity in elderly patients or compounding comorbidities could increase the risk of infection.
Demographic variables including race and sex also may affect the risk of postoperative infection. Female sex was found to have lower incidence for SSI following elective foot and ankle surgery. This finding is supported by Frederick et al 8 who found female sex had an odds ratio of 0.5 for postoperative infection following foot and ankle surgery. Across the literature, female sex has demonstrated a decreased risk for infection following surgery.1,10,18,19 Aghdassi et al 1 found higher rates of infection in males undergoing orthopaedic surgery in a large surveillance study in Germany. Higher rates of infections were also found in males undergoing primary 19 and revision 10 total knee arthroplasty (TKA) in large-database studies. Frederick et al 8 reported that patients of Caucasian race have a 2.3 times increased chance of developing a postoperative infection. They could not adequately explain a reason for this result, but explained there was a low event rate of postoperative infection, leading to a false positive. 8 Our results did not show any significant effect of the race on postoperative infection and wound complications.
In contrast to our results, Carl et al 6 found ASA rating and hypertension to be risk factors for infection. These authors believed that in combination, increased rates of infection in patients with hypertension and ASA suggest more medically complex patients. Higher ASA class has been associated with higher rates of medical morbidity and mortality across several surgical subspecialties. 11 Ridgeway et al 23 found higher rates of postoperative infection with higher ASA ratings in patients undergoing total hip arthroplasty (THA) and hemiarthroplasty. Similarly, Peersman et al 22 found postoperative infection was associated with a higher ASA score for patients undergoing TKA when it was due to specific comorbidities including rheumatoid arthritis. In addition, Carl et al 6 found patients who had a history of neoplasm were more likely to develop a postoperative infection, which was also shown in our results. They suspected that patients with neoplasm had higher infection rates because of higher ASA ratings and worse overall health status, instead of the history of neoplasm as an independent risk factor. Although there was no significant difference in ASA status between patients with and without a history of neoplasm in our investigation, patients with a history of neoplasm had significantly higher incidence of thyroid disease and were significantly older. All these findings indicate that we need to consider patients’ combined comorbidities with the history of neoplasm rather than only the history of neoplasm, which could affect the ASA status and eventually the rate of postoperative infection and wound complications.
Patients who were smokers in our study had an increased rate of postoperative infection and wound complications. Smoking is a well-known significant risk factor for infection after foot and ankle surgery, which has been shown in many previous studies. 3 Increased infection rates in smokers undergoing fixation of calcaneal fractures and ankle fractures has been reported.20,27 Bettin et al 4 found active cigarette smokers were 4.3 times more likely to have a complication than nonsmokers following forefoot surgery, including delayed union, infection, delayed wound healing, and persistent pain. Diabetes has been also shown to have an association with increased infection across several studies.33 -35 Wukich et al 35 found patients with diabetes to have an SSI rate of 9.5% vs 3.5% in patients without diabetes undergoing foot and ankle surgery. This risk is exacerbated by uncontrolled diabetes as the risk of surgical site infection is increased by 7.25 times compared with nondiabetic patients and 3.72 times compared to patients with controlled diabetes. In our study, diabetes was not shown to be a significant risk factor of postoperative infection or wound complications, which was supported by other studies. 6 The result in our study regarding the effect of diabetes on postoperative infection and wound complications should be carefully interpreted. Patients were excluded, whose glycated hemoglobin (HbA1c) level was greater than 7.5, with an average HbA1c level was 6.7, indicating that diabetes in all our cohorts was controlled. Therefore, controlled diabetes in our cohorts did not affect the rate of postoperative infection significantly, suggesting controlled diabetes may not be an independent risk factor of postoperative infection and wound complications. Wukich et al 32 demonstrated poor long-term glycemic control, as measured by HbA1c of ≥8%, results in increased risk of infection following foot and ankle surgery. Further studies with more detailed information of HbA1c level for all cohorts can be considered to understand the association of severity of diabetes with postoperative infection and wound complications.
Other high-risk patients include those who have rheumatoid conditions taking prednisone or tumor necrosis factor alpha inhibitors. These patients have demonstrated high infection rates at 8% and 12% respectively.21,26 Because of the low incidence of rheumatoid arthritis, it did not show a statistically significant difference between the groups and was not identified as an independent risk factor for complications. However, rheumatoid conditions could also be considered for oral antibiotic prophylaxis after elective foot and ankle surgery because of their increased risk of infection.
Operative factors also play a significant role in infection risk for patients undergoing elective foot and ankle surgery. Frederick et al 8 in their retrospective case-control study categorized surgical complexity based on CPT volume by investigating the effect of the number of CPT codes on postoperative infection. They reported that a higher volume of CPT codes per procedure was significantly related to higher incidence of postoperative infection and its severity: superficial vs deep. However, the number of CPT codes might not represent the surgical complexity in certain circumstances. One CPT code is used for a hammertoe repair, a relatively simple procedure, but also one CPT code is used for ankle joint arthrodesis procedure or total ankle replacement, which are relatively complex procedures. We stratified the patients into single and multiple CPT codes, and the result did not identify the number of CPT codes as an independent risk factor of postoperative infection. In our study, patients with multiple incisions demonstrated higher risk of postoperative infection, which was identified as an independent risk factor of postoperative infection and wound complications. More incisions with greater amount of dissection and exposure may lead to inadequate blood supply and tissue necrosis, resulting in limited healing. Hindfoot surgery compared to forefoot/midfoot surgery was also reported as a risk factor for postoperative infection in the previous study. 8 They reported that infection after hindfoot surgery was a significant problem and could result in significant complications that may require revision surgeries, including amputation.12,14 Saibaba and Gopinathan 25 reported that limited vascularity combined with the force going through the hindfoot including calcaneus could predispose it to infection. However, there is no consensus for why hindfoot surgery is more risky in postoperative infection compared with the forefoot/midfoot surgery. Our results did not show a statistically significant difference in postoperative infection and wound complications according to the site of surgery: hindfoot vs other than hindfoot.
Given the similar rates of infection and wound dehiscence reported on using postoperative oral antibiotics, the risks may outweigh the benefit of this treatment. Postoperative oral antibiotics add cost onto each operation and can lead to increased antibiotic resistance. Annually, antibiotic resistance is estimated at ≤2 million infections, 23 000 deaths, and a cost up to $70 billion. 16 There are significant rates of methicillin-resistant Staphylococcus aureus in the United States; thus, measures to decrease antibiotic use may lower this percentage. 13 Furthermore, nonadherence to antibiotic protocols may only intensify antibiotic resistance. 31 Thus, improved antibiotic stewardship after elective foot and ankle surgery may improve population health.
There are several limitations to this study. First, there is the inherent risk of bias from the retrospective nature of this study, and the decision to treat or not treat with antibiotics was not controlled. The completeness and validity of the data could be limited by an incomplete medical record. Second, as this study was not a randomized controlled study, there is likely selection bias in which patients received postoperative oral prophylactic antibiotics based on the surgeon’s current practice patterns. The proportion of patients in the group with and without postoperative oral antibiotic was not even, with a larger proportion of patients receiving antibiotics. However, there were no statistically significant differences between the 2 groups in demographics, patient comorbidities, or surgical complexity as evidenced by duration of surgery or the number and size of incisions. Third, the sample size is relatively small. Fourth, we could not account for all possible risk factors like tourniquet time or other comorbidities. However, all procedures and postoperative rehabilitation protocols were identical as a single surgeon completed all cases. Lastly, the type, dose, and duration of postoperative oral antibiotics were not consistent (Appendix A).
Conclusions
Based on our results, we suggest that routine postoperative prophylactic oral antibiotics are not needed following elective foot and ankle surgeries. However, certain risk factors, including male sex, smoking, a history of neoplasm, and multiple operative skin incisions may increase the risk for postoperative infection and wound complications in foot and ankle surgery. Future prospective randomized controlled studies with a larger sample size will be needed to provide a strong guideline for the use or nonuse of postoperative prophylactic oral antibiotics following foot and ankle surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231224796 – Supplemental material for Do We Need Routine Postoperative Prophylactic Oral Antibiotics in Elective Foot and Ankle Surgery?
Supplemental material, sj-pdf-1-fao-10.1177_24730114231224796 for Do We Need Routine Postoperative Prophylactic Oral Antibiotics in Elective Foot and Ankle Surgery? by Andrew D. Lachance, Margaret E. Giro, Alexander Edelstein, Eliza Klos and Wonyong Lee in Foot & Ankle Orthopaedics
Footnotes
Appendix
The Type, Dose, and Duration of Postoperative Oral Antibiotics.

| Antibiotic Type | Dose | Duration | n/N (total: 240) |
|---|---|---|---|
| Cephalexin | 500 mg QID | 7 | 161/240 |
| 500 mg BID | 7 | 39/240 | |
| 500 mg QID | 5 | 1/240 | |
| 250 mg QID | 7 | 1/240 | |
| Clindamycin | 300 mg TID | 7 | 21/240 |
| 150 mg QID | 7 | 12/240 | |
| 600 mg TID | 7 | 3/240 | |
| Sulfamethoxazole and trimethoprim | 800-160 mg BID | 7 | 1/240 |
| Levofloxacin | 500 mg QID | 10 | 1/240 |
Abbreviations: BID, twice a day; QID, four times a day.
Ethical Approval
Ethical approval for this study was obtained from Institutional review board of the Guthrie Clinic (IRB 2210-59).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.