
Abstract
Purpose:
Postoperative anemia has been a threat to total hip arthroplasty patients. We introduced a novel medullary cavity hemostasis (MCH) technique and combined it with tranexamic acid (TXA) to prevent postoperative anemia in elder patients. This trial was conducted to evaluate the effectiveness and safety of this technique.
Methods:
In this retrospective consecutive study, each group has 88 patients who were all over 70 years old. In the control group, patients were given TXA. In the experimental group, the MCH technique and same TXA application were used.
Results:
The average of total blood loss, drainage volume, and hidden blood loss were significantly less in the experimental group. The postoperative hemoglobin (Hb) level was significantly higher in the experimental group (100.6 g/dL) than it is in the control group (81.4 g/dL). None of the patient has shown signs of prosthesis subsidence, periprosthetical osteolysis, or stem loosening during follow-ups in the average follow-up time of 3 years.
Conclusion:
We discovered that application of TXA alone is not sufficient to prevent postoperative moderate anemia in patients over 70 years old. Combination of TXA and MCH is an effective and safe way to alleviate the severity of postoperative anemia.
Introduction
As the most commonly performed orthopedic surgery for many end-stage hip diseases, the demand for total hip arthroplasty (THA) has increased continuously. 1,2 THA is associated with significant blood loss and often leads to severe postoperative anemia. To address this issue, current research studies have focused on autologous transfusion and blood dropping. A vast number of studies have centered on the application of tranexamic acid (TXA). The dosage, frequency, and route of administration of TXA have been thoroughly discussed and the reported perioperative blood loss has been reduced. 3 –5
However, in elder patients, postoperative anemia remains an unsolved problem even with the application of TXA. The total blood loss (TBL), including intraoperative hemorrhage, hidden blood loss (HBL), and stress response, can result in Hb levels reduction by 30 g/L, 6,7 and these old patients often present with several comorbidities, reduction in physiological reserves, or a disorder of age-related hematopoiesis. 8 The negative impact of anemia on the elderly has been well established. It often associated with increased mortality, higher incidence of cardiovascular disease, cognitive impairment, and an increased risk of falls and fractures. 9 Postoperative anemia also increases the transfusion rate, which could not only raise the economic cost but also provoke heart, renal failure, or infectious disease. 10,11 Therefore, a more aggressive hemostasis method is needed to reduce the postoperative anemia rate and improve the quality of life in elders.
In this study, on the basis of TXA application, we introduced a novel medullary cavity hemostasis (MCH) technique (MHT). We conducted a retrospective analysis on 176 elder THA patients with an average of 3 years of follow-up time. The aim of this study is to evaluate the effectiveness of MHT combined with TXA on anemia rate, TBL, and transfusion rate, as well as the safety in the follow-up time.
Materials and methods
Study design and patients
This level 3 retrospective single-centered clinical study was designed to test the effectiveness and safety of MHT in THA patients aged over 70 years. The study protocol was approved by the local ethical committee. THA patients decided whether to use this technique. In this study, a total of 176 patients undertook the THA in our university hospital between June 2013 and October 2015 were reviewed. There are 88 patients in the experimental group who received the MHT and 88 patients received routine THA as the control group. The inclusion criteria for patients who received the MHT were THA patients older than 70 years old, with preoperative Hb level over 120 g/L (male) or 110 g/L (female). The exclusion criteria were contraindications for rivaroxaban. The detailed information about eligible patients is listed in Table 1. Baseline characteristics showed no statistical significance.
Patient details.a

BMI: body mass index; Hb: hemoglobin; Hct: hematocrit.
a Data are reported as mean ± SD or total sum.
Interventions
All THAs were performed with spinal anesthesia by the same surgery group. The standard surgical procedure involved a minimally invasive posterior approach and a primary hip prosthesis. Two implant systems were used randomly in both control and experimental groups. One hip system was Tri-Lock Bone Preservation Stem (DePuy Orthopedics, Warsaw, Indiana, USA) and another was M/L Taper (Zimmer Biomet, Warsaw, Indiana, USA), both of them were metaphyseal stabilized stem which have similar design and similar surgical procedure. In recent years, most studies indicated that the cemented prosthesis was associated with more intraoperative blood loss, longer operative time, and more heterotopic ossification. 12,13 Therefore, uncemented prostheses were used for primary hip arthroplasty routinely in our department.
The application of TXA was identical to both control and experimental groups. It involved intravenous (IV) administration of TXA 30 min before the surgery (15 mg/kg), and a topical intra-articular TXA (7.5 mg/kg) injection right after the surgery with a 6-h clamp drain. The prosthetic stem was implanted directly into the femoral medullary cavity. One intra-articular drainage tube was placed at the end of surgery and removed once the drainage volume was <50 mL in 24 h.
In the experimental group, patients received MHT and same TXA application. MHT was performed before implantation of the prosthetic stem. The technique was performed as follows: First, a slice of absorbable gelatin sponge was folded and stuffed in the medullary cavity at the distal end of the prosthetic stem. The component of the sponge is type 1 collagen. It was used for local hemostasis and filling. Then 1 g hemostatic powders (Shandong Saikesaisi Co., Ltd, China) were added on the sponge. Third, another slice of gelatin sponge was folded and placed on top of the powder layer. Last, before prosthetic stem was press-fitted into the femoral canal (Figure 1), 2 g of hemostatic powders were then sprayed onto the wall of the femoral medullary cavity. All remaining factors were the same for both groups.
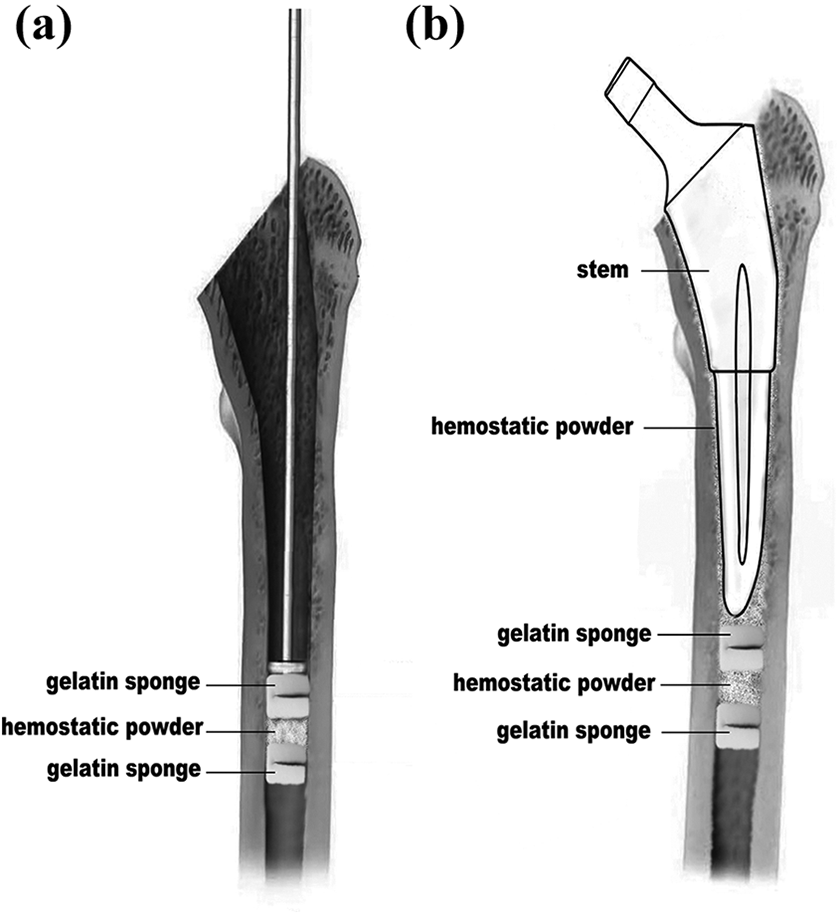
The medullary cavity hemostasis technique: (a) the multilayer plug and (b) the MCH technique. MCH: medullary cavity hemostasis.
After surgery, patients in both groups received rivaroxaban (10 mg once daily) and intermittent pneumatic compression. And they underwent the same rehabilitation protocol. The presence of deep venous thrombosis was examined. Vascular Doppler ultrasonography was used to investigate any calf pain, swelling, or Homan’s sign.
Hb and hematocrit were checked preoperatively, and on postoperative days 1, 3, and 7. HBL was calculated using Sehat et al.’s method on day 3, 14 TBL was calculated using Gross’s method, 15 and patient blood volume is determined using Nadler et al.’s formula. 16
The rehabilitation performance has also been recorded and reviewed in this study. Patients were encouraged to start walking as soon as they feel comfortable to do so.
Transfusion policy
At our university hospital where blood is often in short supply like most hospitals in China, the threshold of blood transfusion is 70 g/L of Hb level.
Follow-up
Patients have been followed up on 1st, 3rd, 6th, 12th, 24th, and 36th month postoperatively. In the follow-ups, patients were assessed with questionnaire, physical examinations, and radiology tests according to Engh et al. standard 17 and Harris score 18 to evaluate the status of the prosthesis. Deep infection, dislocation, and other major complications have also been recorded.
Data collection
The effectiveness outcomes are blood loss-related data including TBL, intraoperative blood loss, drainage volume, HBL, perioperative change of Hb level, postoperative anemia incidence, and transfusion. Time from surgery to walking and time from surgery to a 50 m walking were recorded and reviewed too. The safety outcomes are measured in follow-ups including biological fixation assessed by Engh et al. standard, Harris score, deep infection, dislocation, and other major complications.
Data analysis
Continuous quantitative data were described as mean ± SD. Pearson’s χ 2 test or Fisher’s exact test was used to assess the differences between qualitative variables. Quantitative variables were compared using Student’s independent t-tests. All data analyses were performed using Stata for Mac, version 15.0 (StataCorp LLC 4905 Lakeway Drive, College Station, Texas, USA). The values of p < 0.05 were considered significant.
Results
Effectiveness
Perioperative blood loss, TBL, drainage volume, and HBL were all significantly less in the experimental group than in the control group (Table 2).
Blood loss.a

Hb: hemoglobin.
a Data were checked on postoperative day 3 and reported as mean ± SD or total sum. Mild anemia: Hb: 90–109 g/L (female), 90–119 g/L (male); moderate anemia: Hb: 60–89 g/L; severe anemia: Hb < 60 g/L.
Before surgery, there were no significant between-group differences in Hb levels. However, on postoperative day 3 and 7, the Hb level in the experimental group was significantly higher than the control group (Figure 2).
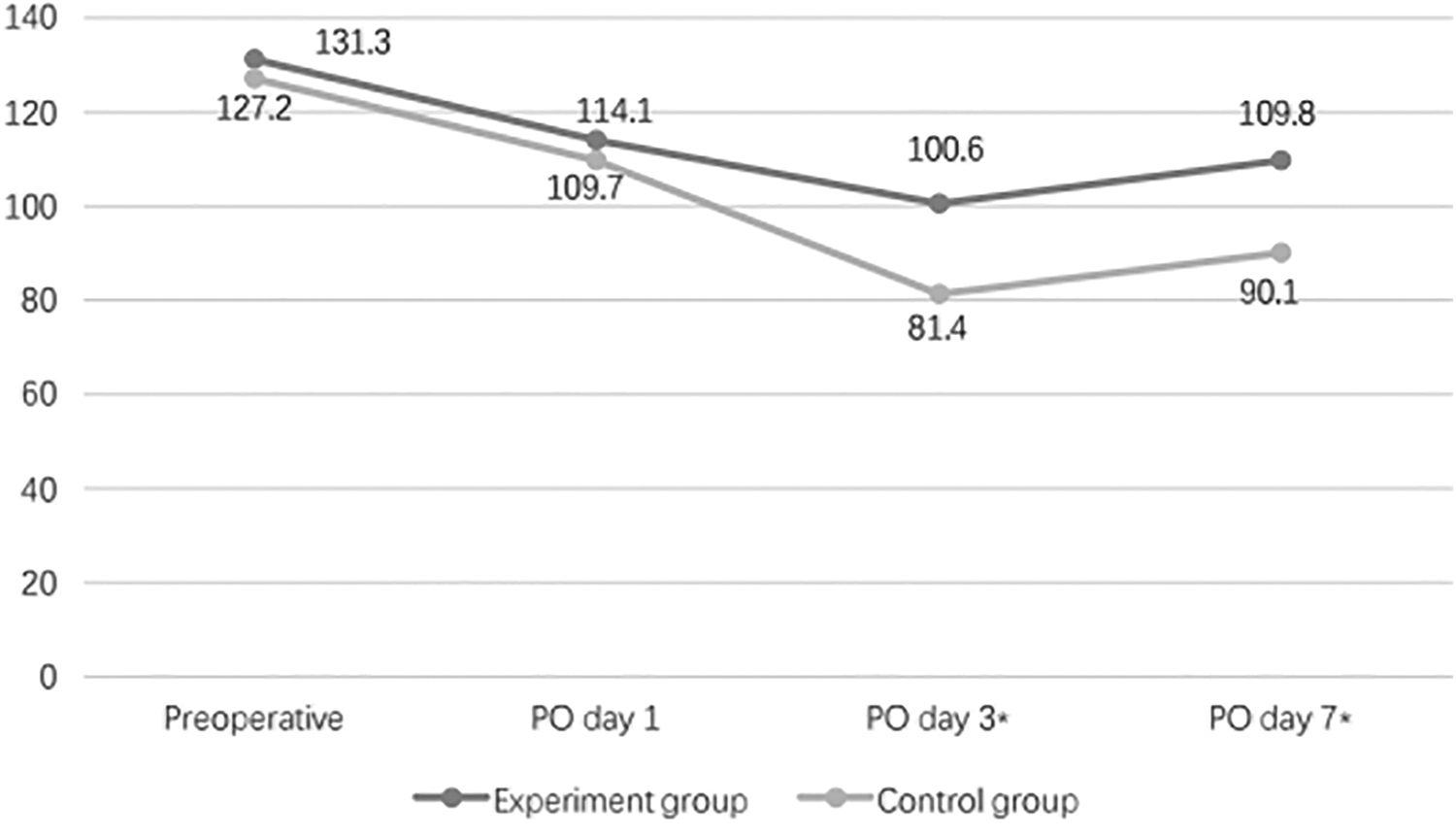
The postoperative Hb level of each group. Hb: hemoglobin.
Postoperative anemia is defined by the Hb level. Before surgery, all patients had normal Hb levels. On postoperative day 3, normal Hb level and mild anemia rates were significantly higher in the experimental group than in the control group (Table 2). At the same time point, two patients in the experimental group and six patients in the control group became severely anemic and required blood transfusion.
Patients managed to start walking on the first day after surgery. It took 3.1 days after surgery for patients in the control group to walk 50 m at a time, while in the experimental group it took only 2.3 days.
Safety
The average follow-up time is 3 years. In the 1- and 3-month follow-ups, none of the patient has shown signs of prosthesis progressive subsidence or periprosthetic osteolysis. In the 6-month follow-ups, all patients have reached osseous fixation. Harris score was 91.1 ± 6.2 for the experimental group and 89.0 ± 7.9 for the control group (p = 0.192). In the 3-year follow-ups, there were no records of postoperative infection, thigh pain, and hip dislocation. Two patients in the experimental group and three in the control group showed symptomatic deep vein thrombosis (p = 0.678). None of the patients in either of the groups developed a pulmonary embolism. Postoperative radiographic evaluation showed no stem loosening in both groups.
Discussion
In this study, our novel MCH technique was combined with TXA application. As a powerful inhibitor of fibrinolysis, TXA has been widely used in surgical hemostasis, especially in the hip and knee replacement.
In this study, we chose a rather active approach of TXA to minimize the blood loss in elderly patients. We combined both preoperative IV and postoperative topic injection together. However, even under this enhanced application of TXA, elder patients in the control group still demonstrated a significant reduction of Hb. The average Hb level on postoperative day 3 has dropped to 81.4 g/L from preoperative level of 127.2 g/L. In a total of 88 controlled group patients, 23.3% patients have demonstrated mild anemia, 64.8% patients reached moderate anemia, and 6 patients reached severe anemia and consequently received transfusion. The ratio of mild-to-moderate anemia is 0.44. The average TBL of the control group was as high as 1232 mL.
Our findings were consistent with previous reports. Konig et al. studied the topical application of TXA in THA and reported that even with the application of TXA, the average TBL of 91 patients is 1384 mL and Hb drop was 3.7 g/dL. 19 In the randomized controlled trial conducted by Martin et al., 25 patients who received 2 g of topical use of TXA suffer an average of 4.10 g/dL drop of Hb level and another 25 patients who received placebo as control presented a even worse drop of Hb as 4.71 g/dL. 3
These results indicate that even under an active application of TXA, elder THA patients still suffer from significant perioperative blood loss and face the threat of anemia. Drug application alone is not sufficient to control the Hb reduction in elder THA patients. Medullary hemorrhage is a large part of blood loss and is difficult to decrease. Alternative methods were needed to change this phenomenon.
In the experimental group, MCH technique and TXA were applied. The same TXA application was used singularly in the control group. Under the circumstance that two groups shared no demographic difference, the experimental group showed a significant influence on blood salvage. Two groups had similar intraoperative blood loss, but the experimental group showed a statistically better result in average drainage (112 mL vs. 147 mL), HBL (728 mL vs. 1053 mL), and TBL (931 mL vs. 1232 mL) than the control group. The reduction of Hb was shown in Figure 2. The average Hb level is also higher in the experimental group on postoperative day 3 (100.6 g/L vs. 81.4 g/L) and day 7 (109.8 g/L vs. 90.1 g/L). As a consequence, more patients in the experimental group were salvaged from moderate anemia. More than 70% of patients successfully remained in mild anemia. The ratio of mild-to-moderate anemia was reversed from 0.44 in the control group to 2.58 in the experimental group. The effectiveness of MCH in preventing postoperative anemia was prominent.
The objective of MCH was to strengthen the hemostasis on the basis of TXA, which may be unnecessary in some special situations, especially in young patients or patients with less comorbidities. Although postoperative Hb reduction is common, even with a 4-g/L Hb reduction, young patients could still be intact from serious bleeding-related disorder. However, in elder patients with displaced femoral neck fracture, sometimes we do have to perform THA for them even if their general status was less ideal. In this circumstance, every effort to reduce blood loss is meaningful for the patient’s recovery. The MCH would shine in these cases.
Hemostatic powder used in this study is microporous polysaccharide hemospheres (MPHs), which can be rapidly cleared within 24–48 h in the human body. MPH particles (diameter of 30–100 m) could concentrate platelets and promote the fibrin clot to form. MPH is hypoallergenic and shares no inherent risk of disease transmission since it is derived from potato starch, compared with other biomaterials derived from animal sources. 20 Previous studies have demonstrated that MPH could be safely used in many surgeries such as micrographic surgery, nephrectomy, and presented positive results in hemostasis. 20 –22 In basic studies, Ereth et al. have proved that MPH would not inhabit bone healing compared to bone wax or microfibrillar collagen. 23
In this study, none of the acute allergy reaction was recorded. For the long-term follow-ups, we used Engh et al. standard and Harris score in our follow-ups to evaluate the implant statutes. In the average 3 years of follow up, all patients reached osseous fixation on the sixth month. No sign of prosthesis progressive subsidence or periprosthetic osteolysis has been observed in any patient in any of thefollow-ups. There were no records of postoperative infection, thigh pain, hip dislocation, and stem loosening in both groups. Two patients in the experimental group and three in the control group showed symptomatic deep vein thrombosis (p = 0.678). According to these results, MCH is a safe technique in elder THA patients.
The mechanism of MHT required further investigation. The inspiration of this technique is based on the previous studies that suggested the bleeding in third space (including medullary cavity) may greatly contribute to the postoperative reduction of Hb. Further study is needed to fully elaborate the mechanism of MHT.
The limitations of this study are also important to be noted. This is a nonrandomized, nonblinded retrospective study. However, a rather large sample size of 176 patients and the minimal follow-up time of 3 years, which is the time that most of the prosthesis-related adverse events would occur, might reduce the potential bias. The intake of rivaroxaban is equal for each patient in this study, whereas TXA administration is personalized according to the weight of the patient. This may result in small variation in blood loss volume. Future studies should note that whether patients with higher preoperative Hb would benefit from MCH.
Conclusion
The application of TXA alone is not sufficient to prevent postoperative moderate anemia in patients over 70 years old. Combination of TXA and MCH is an effective and safe way to reduce the postoperative blood loss and alleviate the severity of postoperative anemia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by research grants from the Chongqing Science and Technology Commission social and people’s livelihood project (cstc2017shmsA130049 and cstc2018jscx-msybX0088).