
Abstract
Introduction:
Neglected Monteggia fracture dislocation in children leads to significant restriction of daily activities by causing decreased range of motion at elbow, stiffness, deformity, and neurological compromise. Various treatment strategies have been described in the literature and one of them is ulnar osteotomy combined with reduction of radial head and annular ligament reconstruction.
Aim:
The aim of this study was to evaluate the results of step-cut osteotomy without the use of bone grafting with reconstruction of annular ligament in the management of neglected Monteggia fracture dislocation in children.
Materials and Methods:
A retrospective study was conducted in six patients with neglected Monteggia fracture dislocation with a mean age of 8.83 years. The median interval between the original injury and the corrective surgery for 6 patients was 4.4 months (range 1–12 months). All children underwent step-cut osteotomy of ulna, open reduction of radial head, and annular ligament reconstruction. Mayo Elbow Performance Index (MEPI) score was used for evaluation.
Results:
The ulnar osteotomies healed uneventfully without the need for a bone graft. Elbow range of motion improved post-op along with improved elbow functioning as indicated by raised MEPI score. The MEPI score was excellent in 5 cases and fair in 1 case.
Conclusion:
Step-cut osteotomy alone without the use of bone grafting and reinforcement with annular ligament repair is a simple yet effective technique for treating neglected Monteggia fracture dislocation.
Monteggia fracture pattern involving the forearm and elbow was initially described by Giovanni Battisa Monteggia in 1814. 1 In this lesion, upper half of the ulna is fractured which leads to dislocation/subluxation of the proximal radioulnar joint. 2 It has been observed in the past that though ulnar fracture is clinically and radiologically easily apparent, dislocation of the radial head can be missed 3
Thirty-three percent of the original Monteggia injuries can be missed and upto 20% late loss of reduction has been seen following close reduction methods. 4 Patients usually seek treatment after many weeks to months after injury or mistreatment, especially in the developing and third world countries. Significant deformity and delayed presentation make it challenging for the orthopaedic surgeon to treat chronic Monteggia fracture dislocation. 5 Untreated Monteggia fracture dislocations can lead to complications that include premature arthritis, instability, decreased range of motion at elbow joint, and valgus deformity of elbow. 4 –6 There have been reports regarding tardy nerve palsy with long-standing chronic Monteggia injuries. 6
A review of literature illustrates various methods for the management of neglected Monteggia fracture dislocation, such as reconstruction of annular ligament, 7 osteotomy of ulna, 8 combination of osteotomy and annular ligament reconstruction, 9 or a combination of open reduction of radial head with osteotomy of ulna and a repair of annular ligament. 6 Distraction and angulation of ulna by lengthening devices/Ilizarov fixator have also been used to achieve close reduction of the radial head. 5
Single-bone fracture in the forearm should always be treated as a fracture dislocation until proved otherwise by adequate clinical/radiological survey. A series of six patients operated in 6 years (2014–2019) were retrospectively reviewed in our study.
Materials and methods
We have performed a retrospective study reviewing six patients of neglected Monteggia fracture dislocation treated from the year 2014 to 2019. The inclusion criteria included time interval between the injury and the surgical repair more than 3 weeks—which is the accepted definition of neglected Monteggia fracture dislocation. 10 All of our patients had a Bado type 1 injury pattern with anterior dislocation of the radial head and malunited fracture of the ulna. No patient had any other associated injury. There was no associated neurovascular injury in any of the cases. All patients were clinically and radiologically followed up for a mean period of 6 months. Mayo Elbow Performance Index (MEPI) consisting of 100 points was used in patient evaluation (Figure 2). This scoring system has four parameters: pain, elbow movement, elbow stability, and performance in daily activities. A patient with excellent result had a score of 90–100 points, a score of 75–89 is good, a score of 60–74 is fair, and a score of less than 60 is poor. 11

(a) Step-cut osteotomy of ulna with one longitudinal and two horizontal limbs is depicted. (b) Sagitally oriented osteotomy fixed with plate in a pictorial representation.
The surgery was performed under general anesthesia, and the posterolateral elbow approach was used utilizing Kocher’s interval. This extensile approach allowed us to combine the ulnar osteotomy, open reduction of the radial head, and annular ligament reconstruction in one incision. We performed step-cut osteotomy at the identified site and fixed it with five to eight hole reconstruction. A sagitally oriented Z-shaped osteotomy was performed with one longitudinal and two horizontal limbs with respect to the shaft of ulna. The osteotomy site was angulated anteriorly and lengthened which allowed anteriorly dislocated radial head to be fall back. Further, direct pressure was used to reduce the radial head. The site of osteotomy was identified from the coronoid process such that at least two screws could be inserted through the plate into the proximal fragment (Figure 1). The angulation at the ulnar osteotomy site was adjusted to obtain a stable reduction. The annular ligament was reconstructed before closing the incision. The reconstruction method was similar to modified Bell-Tawse procedure, wherein a central slip of triceps aponeurosis is taken while preserving its attachment at olecranon. This strip is passed around the radial neck and passed into the ulna through a drill hole. 7 The arm was immobilized in the above elbow plaster of paris slab in the mid-prone position, and intermittent mobilization was started after 2 weeks from the day of surgery. Range-of-motion exercises were gradually increased as the pain and swelling subsided.
Results
There were 6 patients (4 male and 2 female), median age at surgery was 8.83 years (range 5–14 years), and median interval between the original injury and the corrective surgery for 5 patients was 4.4 months (range 1–12 months). In a median follow-up of 6 months (range 3–9 months), all patients obtained stable reduction (Table 1) of the radial head and uneventful healing of ulnar osteotomy (depicted in figures 2, 3, 4 and 5). The ulnar osteotomy site healed at an average time of 9 weeks from surgery in all patients (range 2–4 months). No neurological or vascular complication was seen in all the six patients. One patient had low-grade wound infection which resolved with systemic antibiotics and regular dressings.

Preoperative AP (a) and lateral (b) radiographs of patient with neglected Montaeggia fracture dislocation. AP: anteroposterior.

(a and b) AP and lateral radiographs in immediate post-op period after step-cut osteotomy and radial head relocation procedure. AP: anteroposterior.

(a and b) AP and lateral radiographs of healed osteotomy in the same child. AP: anteroposterior.
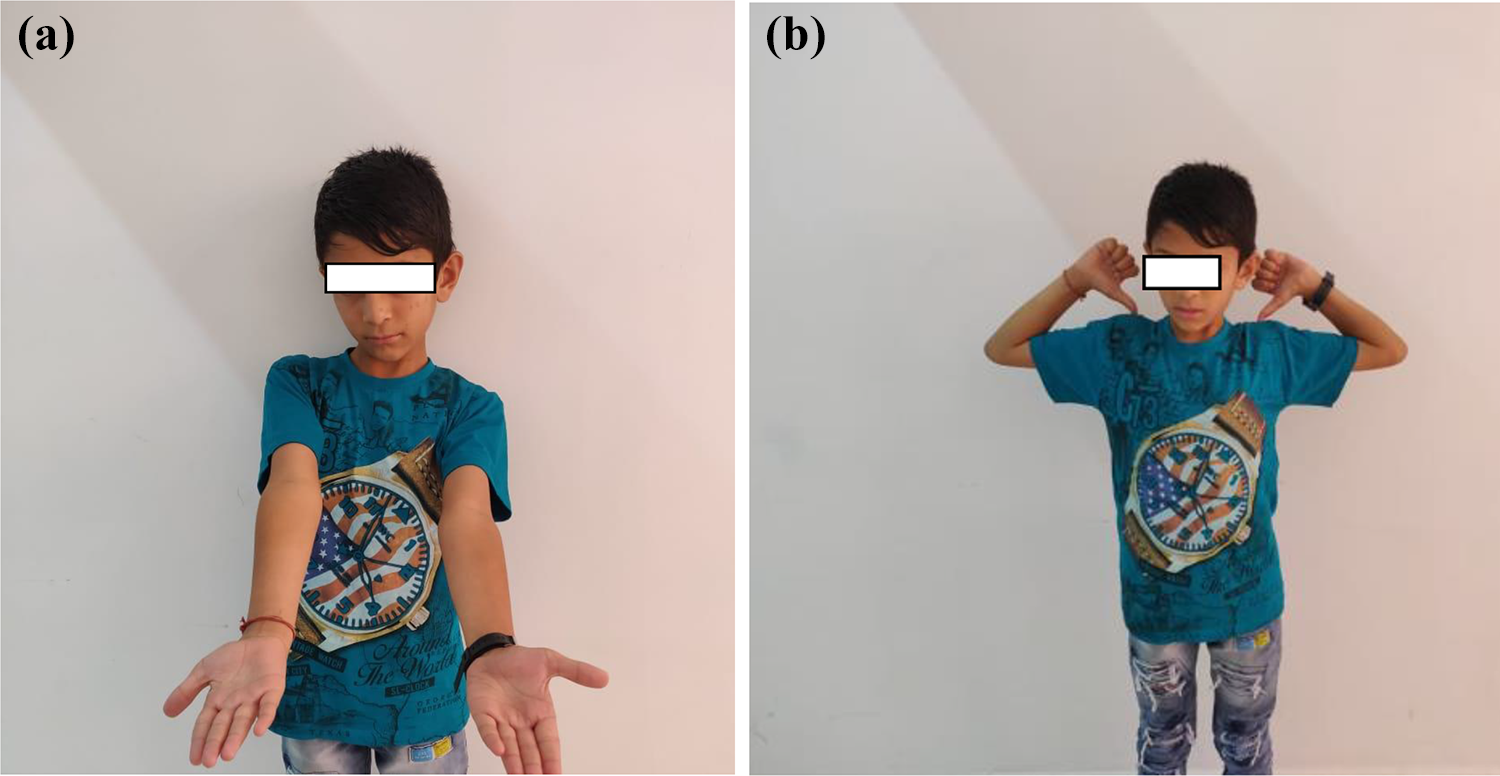
Range of motion achieved at the time of union of osteotomy.
Range of motion achieved based on neutral zero method 12 and MEPI scores.

MEPI: Mayo Elbow Performance Index.
Summary of results.

ROM: range of motion; MEPI: Mayo Elbow Performance Index.
Follow-up radiographs showed that the length of ulna was maintained and ulnar osteotomy united in good position. Radial head was also found to be well located with respect to capitellum in all patients. Based on MEPI, mean increase in MEPI at the final follow-up were 16.6. Mean flexion–extension arc pre-op was 90.83°, while mean supination–pronation arc pre-op was 126.66°. Mean range of motion post-op was 113.3° and supination–pronation arc increased to 140° with supination more restricted than pronation (Tables 1 and 2).
Discussion
The problems associated with neglected Monteggia fractures in children includes a decrease in supination–pronation arc, cubitus valgus, instability of elbow, pain on activity, cosmetic deformity, subluxation of distal radio ulnar joint, and late neuropathy. 13
In case of neglected Monteggia fracture, as time progresses, the radio-capitellar articulation undergoes progressive dysplastic changes whereby a radial head which originally has concave articulating surface with capitellum flattens out. As radial head migrates anterior to the capitellum, the interosseous membrane loses its tension, allows re-dislocation of the radial head 14 even if we attempt a closed reduction. To re-tension it, we need to distract it which is possible by lengthening ulna.
The opinion regarding the maximum age at which treating such cases may be successful varies in the literature. Freedman et al. reported a case of where he could achieve a successful surgical correction after 6 years of original dislocation. 15 Ladermann et al concluded that even after several years of duration from the original insult restoration of joint congruency can be achieved by proximal ulnar osteotomy. 14 Hirayama et al. and Stoll et al. reported that up to 4 years after initial injury, reconstruction could be successfully achieved in children up to 10 years of age. 8 Horii et al. recommended reduction of the radial head in patients under the age of 12 years. 4 Excellent results can be achieved in children younger than 12 years of age because of the potential of remodeling and have flexible soft tissue, so post-op joint stiffness is not a problem. 13,16 However, the interval between traumatic dislocation and reconstructive procedure could affect the outcome due to dysplastic changes.
In very first case of our series, results were fair by MEPI criteria. Mean range of motion decreased after surgical procedure in this case. This could be attributed, in retrospect, to chronicity of dislocation of radial head leading to deformed shape which was not congruent to the capitellum. There were no features suggestive of congenital radial head dislocation in this case like bilateral involvement or a hypoplastic capitellum.
The surgery we performed has been previously described with the primary problem being malunion of ulna preventing reduction of radial head. 4,6,8 The surgical technique consists of ulnar step-cut osteotomy with distraction and angulation. Distraction helps in achieving reduction, while angulation creates an overcorrection maintaining reduction. 14 The principle followed in our procedure is based on the study of Hasler et al. 17 who stated that the only repositioned radial head is “capable of defining the appropriate position for ulnar realignment.” 17 A study published in Egypt in 2017 shows V-shaped corrective ulnar osteotomy used to produce lengthening and angulation of ulna. 4 We did a variation of that procedure by a step-cut osteotomy of the ulna which produced excellent lengthening and angulation at the ulnar osteotomy site. The stability of osteotomy was increased by using internal fixation. The osteotomy site was fixed at the desired length and angulation, once stable reduction of radial head was achieved. Step-cut osteotomy increases the surface area between the two cut end of bones which provides both stability and good union rates.
Annular ligament reconstruction is also a controversial point with some authors favoring it while others disregarding it completely. Annular ligament reconstruction was done in all our cases, though it did not seem necessary as the radial head was stable without its reconstruction. Nakamura et al. 18 and Devnani 19 had differing views on annular ligament reconstruction. Former advocated it in all cases while later ignored annular reconstruction in all cases. Bhaskar advocated an intra-op decision based on the stability of reduction. Annular ligament reconstruction also requires additional dissection which might lead to stiffness of elbow, avascular necrosis of radial head, heterotrophic ossification or synostosis between the radius and the ulna. 20 Redislocation can be attributed to lack of ulnar angulation rather than annular ligament reconstruction. We consider reconstituted annular ligament as an additional check in preventing redislocation.
A preliminary report was published in 2014 by S Rajasekran and K Venkatadass on this novel technique for treating missed Monteggia fracture dislocation and they showed that all their patients had a good outcome. Our study gives support and strength to their preliminary report. 21
Advantages of step-cut osteotomy: Simple surgical technique. Increased surface area of bone–bone contact leading to faster union. A bigger contact area also leads to increased stability. Ability to angulate. No need for a bone graft.
Limitations of the study were less number of patients which can be considered because of rarity of the injury pattern. Most of our patients had Bado type I lesions. We would like to have patients with other type of neglected Monteggia fracture dislocation to be included in this group. One more limitation is lack of longer follow-up. We might consider reviewing long-term results of our follow-up patients to further enlighten us about what future holds for these patients.
Conclusion
Step-cut osteotomy alone without the use of bone grafting and reenforcement with annular ligament repair is a simple yet effective technique of treating neglected Monteggia fracture dislocation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.