
Abstract
Introduction:
Cervical ossification of the anterior longitudinal ligament (OALL) occasionally leads to dysphagia by the anterior osteophyte. A recent report explained that the dysphagia after an occipito-cervical fusion is caused by the narrowing of pharyngeal space due to the cranio-cervical malalignment. The purpose of this study was to evaluate the cranio-cervical alignment in patients with OALL complaining of the dysphagia.
Subjects and methods:
The subjects were 11 cases with complaining of dysphagia due to cervical OALL who underwent anterior cervical OALL resection and as control, age-matched 12 cases without dysphagia who have diffuse idiopathic skeletal hyperostosis in cervical spine. All subjects were male, and the mean age was 59.5 ± 9.1 years. The subjects were divided into two groups according to the symptoms of dysphagia (dysphagia, group A; control, group B). The O–C2 angle, C2–C7 angle, and the maximum thickness of OALL and the cranio-cervical alignment (pharyngeal inlet angle; PIA) and swallowing line (S-line) were measured before and after the operation on the lateral cervical radiogram at the sitting position.
Results:
Group A showed significantly large maximum thickness of OALL, small cervical range of motion, small O–C2 angle, large C2–C7 angle, and small PIA. The S-line crossed the anterior apex of cervical osteophyte in group A. After OALL resection, dysphagia had improved, PIA had increased, and the S-line uncrossed the apex of cervical vertebrae in all cases.
Conclusion:
The prevalence of dysphagia in patients with cervical OALL was influenced by the thickness of osteophyte, cervical mobility, and cranio-cervical alignment.
Keywords
Introduction
Ossification of the anterior longitudinal ligament (OALL) sometimes includes large anterior osteophytes in the cervical spine, which occasionally cause complications of compressing adjoining structures. 1,2 In rare cases, extensive OALL compresses the esophagus, which that can lead to dyspnea and dysphagia. 3 The dysphagia due to OALL was first described in 1950 by Forestier and Rotés-Querol. 1 It is also called ankylosing spinal hyperostosis and is considered a symptom of diffuse idiopathic skeletal hyperostosis (DISH). 4 Based on a radiological survey of the spine, the overall prevalence of DISH in the male population over age 50 years was 25% and that in the female population over age 50 years was 15%. 5 However, OALL progression affects spinal mobility and could compress the esophagus, resulting in laryngeal discomfort, that is, dysphagia. Strasser et al. reported that the occurrence of dysphagia increases with a 12- to 15-mm height of osteophytes. 6 It has also been reported that dysphagia was influenced by the level of osteophytes 7 or adhesion of the esophagus due to chronic inflammation. 8 A recent report explained that dysphagia after an occipito-cervical fusion is caused by narrowing of pharyngeal space due to cranio-cervical malalignment. 9 Kaneyama et al. 10,11 recently explained that the dysphagia after occipito-spinal fusion is caused by the narrowing of pharyngeal space due to cranio-cervical malalignment, which can be illustrated by the pharyngeal inlet angle (PIA) on lateral cervical X-ray images. 10,11
We hypothesized that the pathophysiology of dysphagia in patients with OALL would be similar to the condition after occipito-cervical fusion in terms of poor cervical mobility and malalignment. If that hypothesis is correct, we can suppose that the dysphagia due to OALL is caused by the narrowing of pharyngeal space due to the cranio-cervical malalignment. To date, there have been no reports on any investigation of the relationship between cranio-cervical sagittal alignment and dysphagia in patients with cervical OALL. The purpose of this study was to evaluate the relationship between cranio-cervical alignment and dysphagia in patients with OALL complaining of dysphagia.
Subjects and methods
This study was approved by the Institutional Review Board of our institution. The subjects were 11 cases (59.4 ± 9.0 years) with a complaint of dysphagia due to cervical OALL who underwent cervical OALL resection using the anterior cervical approach from 2010 to 2018 at our university hospital and related tertiary hospitals and as control, 12 age-matched cases without dysphagia who had OALL in the cervical spine (59.6 ± 9.0 years). Subjects who had undergone cervical operation, had previous neurological disease, or cervical trauma were excluded. All patients were male, and the mean age was 59.5 ± 9.1 years.
Clinical evaluation
Dysphagia was screened by swallowing test, and diagnosed by fluoroscopic or endoscopic findings. Patients with collagen disease, otolaryngological disease, neuromuscular disorder, or mental disorder were excluded. The subjects (11 cases) and the control group (12 cases) were classified according to whether they had dysphagia (subjects, group A; control, group B). A postoperative rehabilitation protocol was not considered.
Radiological evaluation
Cervical OALL, cervical range of motion (ROM), O–C2 angle (angle between McGregor’s line and lower end plate of C2), C2–C7 (angle between lower end plate of C2 and lower end plate of C7), 12,13 region, length, maximum thickness of OALL, and PIA 10,11 were measured on a lateral cervical radiogram. Measurements of ROM of C2–C7 were performed as shown on the flexion and extension films with maximum effort of active motion. 14 PIA was defined as the angle between McGregor’s line and the line linking the center of the C1 anterior arch and the apex of the cervical sagittal curvature (Figure 1). 10,11

(a to c) PIA on the lateral cervical radiogram at follow-up. PIA is defined as the angle between McGregor’s line and the line that links the center of the C1 anterior arch and the apex of cervical sagittal curvature. PIA: pharyngeal inlet angle.
Statistical evaluation
Values were expressed as mean ± standard deviation. Statistical analyses were performed using JMP software package version 10.0 (SAS Institute Inc., Cary, NC, USA). Wilcoxon rank sum test was used to determine intergroup differences between group A and group B to evaluate the outcome measures of parameters, and the effect size (r) was calculated. Statistical differences were considered significant at p < 0.05.
Results
In the 11 subjects of group A and the 12 subjects of group B, preoperative radiographic measurements were as follows (group A/group B): maximum thickness of OALL (10.1 ± 3.2 mm/7.2 ± 4.4 mm, p = 0.03), cervical ROM (10.9 ± 5.0°/17.9 ± 8.7°, p = 0.001), O–C2 angle (14.0 ± 4.31/24.4 ± 10.8°, p = 0.01), C2–C7 angle (15.1 ± 10.6°/4.8 ± 5.7°, p = 0.04), PIA (87.6 ± 8.4°/94.4 ± 10.3°, p < 0.05) (Table 1). There were significant differences between all items. The numbers of cases with maximum ossification level were as follows: group A: C2/3, n = 5; C3/4, n = 1; C4/5, n = 4; C5/6, n = 2; group B: C2/3, n = 2; C3/4, n = 4; C4/5, n = 3; C5/6, n = 2. In group A, the S-line crossed the anterior apex of cervical osteophytes before the operation. However, following OALL resection, dysphagia had improved, PIA had increased to 97.0 ± 4.5°, and the S-line uncrossed the apex of cervical vertebrae in all cases. The mean follow-up period was 32.7 months, ranging from about 6 months to 7 years. In addition, there were no patients or control subjects with rheumatic disorders.
Mean and SD values of the measurements.
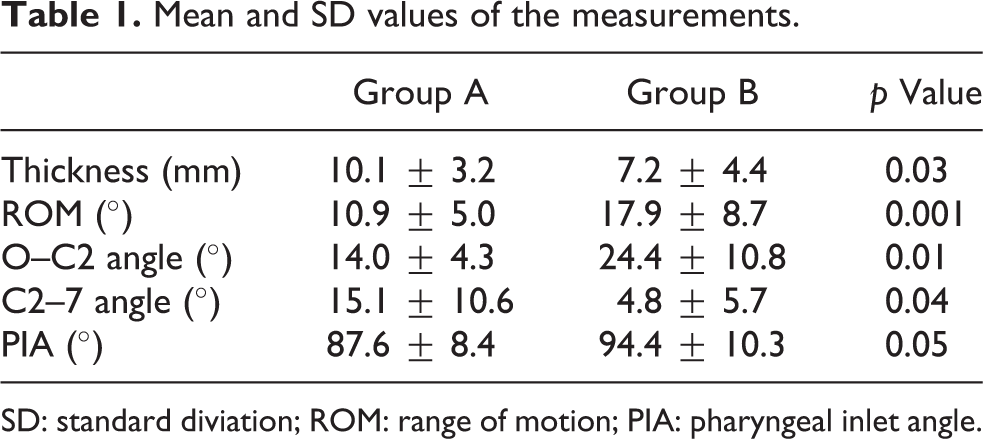
SD: standard diviation; ROM: range of motion; PIA: pharyngeal inlet angle.
Discussion
The present study showed that dysphagia due to OALL was influenced by the thickness of OALL, O–C2 angle, C2–C7 angle, cervical ROM, level of OALL, and PIA. PIA can show the relationship between sagittal cranial alignment and the anterior apex of cervical vertebrae. The results of this study revealed that cranio-cervical alignment is related to dysphagia in patients with cervical OALL.
Cranio-cervical malalignment is known to cause dysphagia after occipital–cervical fusion. Dysphagia after occipital–cervical fusion due to the narrowing of oropharyngeal space that causes the posterior pharyngeal wall bulge at the mid-lower cervical level. 10,11,15 However, Tian and Yu reported that 12.8% of anterior cervical spine surgery and 9.8% of posterior cervical spine surgery caused dysphasia due to an increase in the C2–C7 angle postsurgery. 15 Kaneyama et al. 10 used radiological evaluation of cranio-cervical alignment to show PIA in patients with occipito-cervical fusion. It was mentioned that when PIA is less than 90°, the pharyngeal space becomes narrow. Based on these findings, it is possible that not only the O–C2 angle and C2–C7 angle but also the positional relation between the cranium and the cervical spine are related to the incidence of dysphasia due to cervical OALL. It can be considered that dysphagia in patients with cervical OALL occurs by the narrowing of the pharyngeal space due to cranio-cervical malalignment, similar to dysphagia after occipital–cervical fusion.
In this study, the PIA in group A was statistically small compared to group B before the operation. After the OALL resection, PIA increased to 97.0 ± 4.5°, resulting in an improvement in dysphagia. PIA is a useful landmark in choosing OALL resection as a treatment for cervical OALL.
The cervical ROM of OALL is generally reduced due to intervertebral ossification. The standard cervical ROM of men in their 70s has been reported as 41.7 ± 9.7°. 16 Cervical ROM prior to surgery in group A was 10.9 ± 5.0°. The loss of cervical mobility in group A could induce poor pharyngeal movement. Although cervical ROM had not improved after the operation, dysphagia had improved. From these results, our hypothesis that the pathophysiology of dysphagia in patients with OALL would be similar to the condition after occipito-cervical fusion has become more convincing. Therefore, regarding the onset of dysphagia in patients with OALL, cervical and cranio-cervical sagittal alignment as well as the thickness of osteophytes need to be carefully examined. To the best of our knowledge, there have been no studies regarding dysphagia in patients with OALL in terms of cervical sagittal alignment.
This study has the following limitations. First, the number of subjects was small due to the rarity of cases, 17 although the effect size was acceptable according to the r value (Table 1). 18,19 Second, the cause of dysphagia is multifactorial and analysis of all factors including physiological pharyngeal reflex, muscle condition, and so on was not possible. Despite these limitations, the data regarding cranio-cervical alignment in the patients with dysphagia due to OALL may be of particular value.
Conclusion
This study showed that the prevalence of dysphagia in patients with cervical OALL was influenced by the thickness of osteophytes, cervical mobility, and cranio-cervical alignment. In fact, in cervical OALL patients with dysphagia, dysphagia improved after OALL resection when PIA was more than 90°. This result suggests that the mechanism causing dysphagia in patients with cervical OALL is due to cranio-cervical malalignment and that OALL resection is effective for patients with cervical OALL who have dysphagia.
Footnotes
Acknowledgments
We are indebted to the Department of International Medical Communications of Tokyo Medical University for the editorial review of the English manuscript. The authors would also like to thank Ms Yuri Amamizu of the Department of Orthopedic Surgery for assistance with preparing the initial English manuscript. We’d like to express our gratitude to Mr Arndt Gerz for the editorial review of the revised manuscript.
Hirosuke Nishimura, Kenji Endo, Takato Aihara, Kazuma Murata, Hidekazu Suzuki, Yuji Matsuoka, Taichiro Takamatsu, Asato Maekawa, Yasunobu Sawaji, Hanako Tsuji and Kengo Yamamoto
Author contributions
Conception and design: KE, HN, and TA contributed to the conception and design of the study; HN and KM were involved in data acquisition; KE, HS, and YS helped in analyses and interpretation of data; KE, AM, TA, and HT drafted the manuscript; YS, YM, HN, and TT analyzed the data; and KY supervised the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.