
Abstract
Purpose:
Adjacent segment disease (ASD) constitutes a long-term complication of instrumented spinal fusion. Aim of this study is to analyze the utilization of percutaneous transforaminal endoscopic discectomy (PTED) for the treatment of symptomatic ASD, emphasizing basically in the postoperative course.
Methods:
A prospective study with 35 patients was designed. Patients enrolled in our study were distributed in two different groups. Group A constituted of 15 patients featuring ASD as a complication of a previously conducted lumbar spinal fusion. Group B was composed of 20 patients, presenting simple lumbar disc herniation (LDH). All patients were subjected to successful PTED for LDH. Patients were evaluated at regular intervals in 6-week and 3-, 6-, and 12-month postoperatively. Visual analog scale was utilized for leg (VAS-LP) and low back pain (VAS-BP) evaluation. Health-related quality of life was assessed with short-form 36 health survey questionnaire (SF-36).
Results:
VAS-BP scores were statistically significantly differentiated between the two groups in all intervals of follow-up. In contrast, VAS-LP scores demonstrated statistically significant differentiation in none of follow-up intervals, indicating similar results between the two groups. Maximal improvement was in both cases for all patients observed in 6-week postoperatively, with subsequent stabilization. SF-36 preoperative evaluation denoted a statistically significant differentiation in bodily pain and role emotional parameters, which was continually until the end of follow-up observed. The other SF-36 parameters featured similar values between the two groups preoperatively as well as during the follow-up intervals.
Conclusion:
PTED is capable of successfully dealing with LDH and furthermore with complications of fusion as ASD.
Introduction
Adjacent segment disease (ASD) constitutes a long-term complication of instrumented spinal fusion, appearing either in cervical or in lumbar spine. Incidence of lumbar symptomatic ASD features remarkable differentiation among the different studies, being overall reported from 5.2% to 18.5% per year. 1 ASD etiology is multifactorial, including adjacent level spondylosis, preoperative degenerative disc disease, as well as biomechanical forces alteration in adjacent segments. 2,3 ASD treatment is initially conservative. However, gradual emergence of neurological deficit dictates surgical intervention. Multilevel lumbar spinal fusion or posterior lumbar dynamic stabilization may be then recruited by the spine surgeon. 4
Percutaneous transforaminal endoscopic discectomy (PTED) constitutes a full-endoscopic increasingly selected therapeutic strategy for lumbar disc herniation (LDH) treatment. 5 Access to disc pathology is accomplished through the intervertebral foramen, enabling working into an anatomic triangle (safe zone). This triangle was first described by Kambin and Brager in 1987, being responsible for the rapid deployment of this surgical technique. 6 PTED is characterized by many advantages versus microdiscectomy, including preservation of anatomic structures, decreased hospital stays and perioperative morbidity, as well as shorter rehabilitation times. 7,8
To our best knowledge, utilization of PTED for treatment of adjacent segment radiculopathy has been only three times reported. 9 –11 However, PTED outcomes among patients with LDH and ASD have never been compared with these of patients with LDH and no other comorbidities.
Aim of this study is to analyze the utilization of PTED with Transforaminal Endoscopic Surgical System (TESSYS) technique for adjacent segment decompression in patients with radiculopathy as a result of LDH. Specific emphasis in the postoperative course is attributed. One-year follow-up was conducted, evaluating postoperative results with specific clinical scales. Comparison of postoperative results of patients with ASD versus patients without any comorbidities was also performed. PTED role in ASD treatment is, therefore, discussed.
Patients and methods
Study population
All patients recruited in this study were diagnosed with LDH, being suitable for discectomy according to the current indications. After detailed explanation of aims and scope of the study, all patients decided to participate, signing a fully informed written consent. Approval of institutional review board and ethics committee of the hospital was accomplished. Furthermore, all aspects of this study were in accordance with the principles set forth in the Helsinki Declaration.
Inclusion and exclusion criteria
Inclusion criteria were (i) radiculopathy, (ii) positive nerve root tension sign, (iii) sensory or motor neurologic lesion on clinical examination, (iv) hernia confirmed by magnetic resonance imaging (MRI) of the lumbar spine, in compliance with clinical findings, and (v) failure of 12-week conservative treatment.
Exclusion criteria were (i) noncontaminated disc hernia exceeding the one-third of the spinal canal on the sagittal MRI scans, (ii) sequestration of the disc, (iii) central or lateral recess spinal stenosis, (iv) recurrent herniated disc or previous surgery at the affected level, (iii) segmental instability or spondylolisthesis, (iv) spinal tumor or infection, and (v) vertebral fracture.
Methods
A prospective study with 35 patients was designed and conducted. Patients enrolled in our study were distributed in two different groups. Group A (ASD group) constituted of 15 patients featuring ASD, as a complication of a previously conducted posterolateral fusion (PLF; Figure 1). Clinical symptomatology of ASD emerged 5 years after PLF in all patients. Group B (control group) was composed of 20 patients, presenting simple LDH, not as a result of ASD (Figure 2). All patients were subjected to successful PTED for LDH in 2015–2016. Patients were evaluated at regular intervals in 6-week and 3-, 6-, and 12-month postoperatively. Postoperative assessment was conducted recruiting well-established uniform clinical scales. Visual analog scale (VAS score) was used for leg (VAS for leg pain—VAS-LP) and low back pain (VAS for back pain—VAS-BP) evaluation. Health-related quality of life (HRQoL) was, respectively, assessed with the short-form 36 health survey questionnaire (SF-36).

(a) Sagittal and (b) axial preoperative T2-weighted MRI of a patient in the ASD group. MRI: magnetic resonance imaging; ASD: adjacent segment disease.

(a) Sagittal and (b) axial preoperative T2-weighted MRI of a patient in the control group. MRI: magnetic resonance imaging.
Surgical technique
All patients participated in this study underwent full-endoscopic PTED with TESSYS technique by the same experienced spine surgeon in the same hospital. This technique was performed under local anesthesia and mild sedation. Patients monitoring in terms of pulse rate, blood pressure, oxygen saturation, and electrocardiographic signals was uninterruptedly transacted. Patients were initially placed at the lateral decubitus position, lying down on the opposite side. Lesion was thus confronted upwards. After surgical field disinfection, local anesthesia at the needle entry point was conducted. This point was anatomically about 11 cm off-midline defined. Transforaminal promotion of the needle through the anatomic triangle of Kambin (safe zone) was subsequently performed. 6 Mild sedation and anesthesia (fentanyle ampule) were administered after fluoroscopic verification of the operated level (Figure 3). Sequential transforaminal passage of three different size reamers (5.5, 6.5, and 7.5 mm) constituted the next step (Figure 4). The cannula and endoscope were afterwards carefully inserted, to ensure nerve root preservation. Removal of herniated disc material was finally with graspers utilization accomplished (Figure 5). Patients were transferred to the monitoring chamber for the following hour, being subsequently mobilized. They were hospitalized during the day of surgery and discharged in the first postoperative day. Follow-up was performed at the regular intervals of 6-week and 3-, 6-, and 12-month postoperatively. No perioperative complications were recorded in either group.
Fluoroscopic verification of the operated level.

Sequential transforaminal passage of different size reamers.

Removal of herniated disc material with graspers.
Visual analog scale for leg and low back pain
VASs constitute a well-established, simple, and illustrative method of various parameters assessment, including pain. In this study, a unipolar horizontal line (100 mm length) was utilized. Patients were encouraged to indicate with a pen the level of pain, according to their subjective perception. This scale was completed two times for each individual (for leg and low back pain, respectively), in each regular interval follow-up. Score of individuals was then in mm measured, recruiting a one decimal place approach. Radicular symptomatology was thus objectively evaluated. Level of the minimal clinically significant alteration was defined at 9 mm. Parameters as gender, age, and pain etiology were not separately considered. 12
Short-form 36 health survey questionnaire
SF-36 constitutes a widely utilized method for HRQoL evaluation in spine surgery. 13 This multiscaled questionnaire consists of 36 items, representing 8 discrete parameters of patients general health; physical function (PF), role-physical (RP), bodily pain (BP), general health (GH), energy, fatigue and vitality (V), social function (SF), role-emotional (RE) and mental health (MH). Patients were asked to complete this questionnaire at the regular follow-up intervals. Results from each individual were then collected, being transformed into a percentage scale. Higher scores in these eight dimensions are associated with enhanced quality of life. Minimal percentage of completed entries was determined at 50%. Questionnaires were considered invalid if less than half of form entries were completed.
Statistical analysis
Statistical process of the data was conducted with the statistical package SPSS, version 23.00 (SPSS Inc, Chicago, Illinois, USA). Continuous variables (age, VAS scores, and SF-36 scores) were expressed as mean ± standard deviation and categorical variables as percentages. Student t-test for independent samples was utilized for the statistical comparison of the continuous parameters (VAS and SF-36 scores), provided that normal distribution was present. Otherwise, Mann–Whitney test was recruited. The level of statistical significance was defined at p = 0.05. VAS scores for leg and low back pain and SF-36 scores were measured for each individual in the two groups in 6-week and 3-, 6-, and 12-month postoperatively. Possible differentiation of parameter values throughout the follow-up intervals was initially investigated in each group. Subsequently, each parameter was compared between the two groups for the potential finding of statistically significant difference.
Results
Patients were divided into two groups, Group A (ASD group) and Group B (non-ASD, control group), presenting in general similar baseline demographic characteristics. Preoperative evaluation revealed a statistically significant differentiation in parameters VAS-BP (VAS evaluation) and BP and RE (SF-36 evaluation; Tables 1 and 2).
Demographic characteristics of enrolled patients.

VAS-LP: visual analog scale for leg pain; VAS-BP: visual analog scale for back pain.
* Statistically significant p-values are highlighted in bold. Level of significance was determined at p-value = 0.05.
Baseline preoperative values of SF-36 parameters in the two groups.

PF: physical functioning; RP: role physical; BP: bodily pain; GH: general health; V: vitality; SF: social functioning; RE: role emotional; MH: mental health; SF-36: short-form 36 health survey questionnaire.
* Statistically significant p-values are highlighted
Values of all indexes featured the maximal improvement in 6-week postoperatively among total population. Stabilization and minimal further improvement were identified afterwards, during the next follow-up intervals. Regarding the statistical course of indexes in each group during the various follow-up checkpoints, improvement of all studied indexes at 6 weeks was statistically significant when compared with preoperative values in each patient in either group. Subsequently, all parameters featured stabilization with minimal quantitative improvement, featuring thus no statistical significance when compared with values of previous follow-up interval (Figure 6).

Values of all indexes.
Regarding the comparison of studied indexes between the two groups, VAS-BP scores were statistically significantly differentiated between the two groups in all intervals of follow-up (Table 3). In contrast, VAS-LP scores demonstrated statistically significant differentiation in none of follow-up intervals, indicating similar results between the two groups (Figure 7). Maximal improvement was in both cases for all patients observed in 6-week postoperatively, with subsequent stabilization. VAS values were in general equally decreased between the two groups during follow-up periods, presenting almost no statistically significant differentiation (Table 3, Figure 7).
VAS-BP values alteration during regular follow-up intervals at 6 weeks and 3-, 6- and 12-month postoperatively.
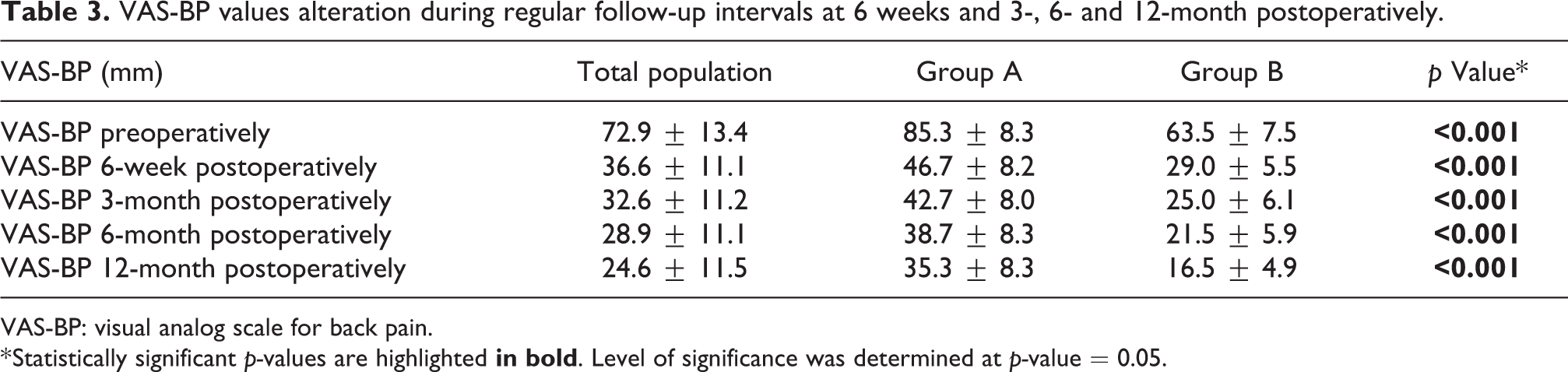
VAS-BP: visual analog scale for back pain.
* Statistically significant p-values are highlighted

VAS-LP scores. VAS-LP: visual analog scale for leg pain.
SF-36 preoperative evaluation denoted a statistically significant differentiation in BP and RE parameters (p < 0.001). This differentiation was constantly maintained until the end of follow-up (Figure 8). p Value was steadily p < 0.001 in all follow-up intervals, indicating a strong statistical differentiation for these two parameters between the two groups.

SF-36 evaluation, RE parameter. SF-36: short-form 36 health survey questionnaire; RE: role emotional.
The other SF-36 parameters featured similar values between the two groups preoperatively as well as during the follow-up intervals. Statistically significant correlation was not detected. Stabilization of the improvement was accomplished after 6 weeks, demonstrating equal enhancement among the two groups (Figure 6).
Discussion
Spinal fusion constitutes an increasingly conducted technique in recent years, being particularly popular in the field of spine surgery for the treatment of selected symptomatic patients with degenerative disorders. 1 The rapid expansion of this technique is associated with the analogous increment of ASD incidence. 14
ASD is identified as the deployed degeneration of the mobile segments located above and below from a fused spinal segment. ASD is a wide descriptive term that may contain different pathological correlations as a result of spinal fusion; disc degeneration, spondylolisthesis, arthritis of the hyperthopic facet joint, stenosis, herniated nucleus pulposus, as well as instability may all be defined as ASD.
Several factors have been described as potential risk factors for ASD progression. Wang et al. indicated that higher BMI, preoperative disc degeneration at adjacent segment, and intraoperative superior facet joint violation are risk factors for ASD. 15 Alentado et al. noted several predictors of developing ASD including antidepressant use, diagnosis of degenerative scoliosis, fusion of L4-S1, having no decompressions adjacent to the fusion, and low sacral slope. 16 In another study, Yamasaki et al. reported that patients with preoperative sagittal imbalance had a statistically significant increased risk of ASD, especially for those subjects with preoperative pelvic tilt of more than 22.5°. 17 Furthermore, Kim et al. concluded that the occurrence of radiological ASD is multifactorial and associated with a higher BMI, preoperative facet, and disc degeneration on preoperative examination and a smaller preoperative paraspinal muscle area preoperatively. 2
Regarding the biomechanics, reductions of the lumbar intervertebral foramina dimensions, which have been observed at the adjacent and the involved levels of patients with degenerative disc disease imply that similar changes occur at the ASD despite the lack of radiographic evidence of degeneration. 18 Additionally, adjacent segment intervertebral joint loads have been linked to the degree of lordosis that is surgically imposed during vertebral fusion, indicating that an artificial decrease in lumbar lordosis caused by an L4/5 fusion lead to adverse loading conditions for the adjacent levels. 19
To prevent ASD, it is believed that motion-preservation procedures present an advantage on reducing the prevalence of adjacent segment degeneration-disease and the reoperation rate due to the adjacent segment degeneration compared with the lumbar fusion. 20 It is suggested that total disc replacement may be an effective technique for the treatment of selected patients with lumbar degenerative disc disease and is at least equal to lumbar fusion in the short term; however, disadvantages may appear after years. 21 Circumferential lumbar fusion provides favorable clinical results at short-term follow-up. Nevertheless, the high rate of ASD and reintervention procedures questions the reliability of this technique for lumbar fusion. 22 It has been mentioned that preserving the posterior complex during decompression can be effective on preventing ASD following posterior lumbar interbody fusion surgeries. 23 Moreover, the use of posterior lumbar dynamic stabilization may offer as an alternative to multilevel arthrodesis or the management of patients who develop ASD. 4
Although fusion has evolved over the last years, it certainly presents several disadvantages in comparison with PTED. The length of the incision and the application of screws and plates increase trauma extent and the possibility of blood loss, inflammation, and eventually scar tissue. Several complications have been reported including motor femoral nerve injury, retroperitoneal hematoma, fractures, abdominal hernia, mobilization and inadequate fusion, radiculopathy, sympathectomy, and even bowel perforation. 24,25 Thus, fusion surgery for patients with ASD increases the level of difficulty because there is a need for readjustment of plates and screws or even for the extension of fusion increasing the possibility of complications. All the above can be prevented with the use of endoscopy.
PTED is a minimally invasive full-endoscopic spine surgical procedure performed principally for the treatment of LDH. 26 It has several advantages in treating recurrent LDH, such as avoiding from the old scar tissue, decreasing operation-related complications, shortening operation time, reducing trauma, and obtaining rapid postoperative recovery. 27 The technique combines the benefits of endoscopy (direct visualization, reduced traumatization, hospital stay, and postsurgical morbidity) with optimal exposure of the intervertebral space and preservation of the dorsal musculature, the vertebrae, and the ligamentous structures. 28 PTED has been associated with less blood loss, faster rehabilitation, and less scarring of tissue than conventional open microdiscectomy. 7 PTED appears to be a safe and effective intervention for LDH and has similar clinical outcomes compared with conventional open microdiscectomy. 29
Until now, recruitment of PTED for treatment of adjacent segment radiculopathy has been only three times reported. Telfeian studied a consecutive series of nine patients who underwent transforaminal endoscopic treatment for lumbar radiculopathy adjacent to an instrumented spinal fusion. Three patients required revision to fusion at 2-, 13-, and 19-month postoperatively. The mean visual analog scale score for radicular pain improved from an average pain score before surgery of 8.4 to 1.3 1 year after surgery and the mean visual analog scale for back pain improved from an average pain score before surgery of 8.0 to 4.7 1 year after surgery. However, the 2-year failure rate presented was 33%. 10 Ba et al. studied 64 patients diagnosed with single-level ASD and accepted revision surgery. Thirty-three patients were treated with percutaneous endoscopic transforaminal procedure and 31 underwent PLF. The improvement rate was 82.75% in the first group and 86.28% in the second. The satisfactory clinical outcomes were similar in both groups with no recurrence in all cases, but the endoscopic procedure was less invasive and could shorten hospitalization time. 9
More recently, Gu et al. attempted to evaluate the clinical outcomes of implementation of PTED in elderly patients with ASD post lumbar fusion surgery. For this purpose, 25 consecutive elderly individuals were retrospectively assessed for a mean follow-up of 37.14 ± 11.60 months. Multiple clinical scores as MacNab classification, VAS, Oswestry disability index (ODI), Japanese orthopedic association score, as well as SF-36 were recruited. Results indicated that all studied indexes featured a statistically and clinically significant amelioration directly postoperatively at first day, which was preserved during the next follow-up checkpoints at 3 months and 1 year until the end of follow-up. Patients (84%) futured excellent or good clinical outcomes according to MacNab criteria, whereas 12% and 4% experienced fair and poor outcomes, respectively. VAS score was distinctly assessed for low back and lower limb pain and all patients demonstrated statistically significant improvement of these parameters directly postoperatively with subsequent maintenance of this improvement. Furthermore, all aspects of SF-36 were significantly improved at the end of follow-up when compared with the preoperative baseline values. Authors concluded that PTED represents a beneficial alternative concerning efficacy and safety in surgical treatment of ASD after lumbar fusion in elderly patients. 11
In our study, values of all indexes featured maximal improvement among both groups. SF-36 parameters featured in general similar values between the two groups preoperatively and during the follow-up intervals, with stabilization of the improvement accomplished after 6-week postoperatively. Also, VAS values were equally decreased between the two groups during follow-up periods. However, VAS-BP scores were differentiated between the two groups in all intervals of follow-up and SF-36 preoperative evaluation presented a statistically significant differentiation in BP and RE parameters, which was also continually postoperatively recorded. These statistic results indicate that patients with ASD present persistent BP (especially low back pain) due to the instrumented fusion, something which affects their emotional role as well. However, these patients also benefit from PTED, since all studied indexes in this group were statistically significantly improved in all sections of follow-up when compared with preoperative baseline values, which is consistent with the findings of Gu et al. and the other relative above-discussed studies. 9 –11
As regards to the study design, we have not included the widely used ODI and Macnab criteria, because we theorized that concurrent implementation of SF-36 with VAS represents a multiscaled and more multifaceted combination, evaluating pain as well as physical, social, and emotional factors of patients’ life. It is important to mention that it would increase the significance of our study results if we considered designing one more year follow-up to achieve 2 years. The exact pathogenetic mechanisms of ASD remain unclear. Hence, PTED implementation may represent a purely symptom-relieving treatment in ASD, since the potential underlying degeneration process may lead in subsequent requirement of further therapeutic interventions. 30,31 On this thesis, a more extensive follow-up assessment would provide further information about the exact contribution of PTED in ASD clinical progression. A greater number of patients could be also enrolled. All these did not happen because we aimed to present the early clinical findings of our work.
For the first time in the literature, the quality of life after PTED for LDH is studied between patients with ASD and patients with no other comorbidities. Despite the different pathogenesis in these distinct entities, the favorable postoperative clinical outcomes in patients with ASD enforced us to hypothesize that the influence of PTED in clinical condition of patients with ASD might be enough beneficial, so that the postoperative clinical course of these patients would be similar to those with simple LDH and no additional comorbidities. Hence, this particular patients’ classification sought to demonstrate the pure clinical effect of PTED in ASD clinical progression. Indeed, both groups featured almost equal amelioration, with the first group presenting slightly less improvement. Patients with ASD present persistent BP due to fusion, something which affects their emotional and physical status. PTED is capable of successfully dealing with LDH and additionally with the complications of fusion such as ASD. Minimally invasive spine surgery is gaining popularity over the last years with PTED appearing to be a promising alternative surgical choice for patients with ASD. Finally, the general condition of patient leads us to choose between conventional and minimally invasive spine surgery.
Conclusion
PTED was demonstrated to have a beneficial impact in quality of life of patients with LDH only as well as in the frame of ASD, as a complication of a previously performed spinal fusion. Patients with ASD denote slightly lesser enhancement rates in regards to quality of life evaluation, especially due to the chronic BP as a result of the spinal fusion. Nevertheless, outcomes of PTED conduction in these patients were found to be favorable. Additional studies with larger population sizes and potentially longer-term quality of life assessment are required, to better elucidate the punctual impact of PTED in this particular patient subcategory.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.