
Abstract
Background:
Readmission following total joint arthroplasty has become a closely watched metric for many hospitals in the United States due to financial penalties imposed by Centers for Medicare and Medicaid Services. The purpose of this study was to identify both preoperative and postoperative reasons for readmission within 30 days following primary total hip and total knee arthroplasty (TKA).
Methods:
Retrospective data were collected for patients who underwent elective primary total hip arthroplasty (THA; CPT code 27130) and TKA (27447) from 2008 to 2013 at our institution. The sample was separated into readmitted and nonreadmitted cohorts. Demography, comorbidities, Charlson comorbidity index (CCI), operative parameters, readmission rates, and causes of readmission were compared between the groups using univariate and multivariate regression analysis.
Results:
There were 42 (3.4%) and 28 (2.2%) readmissions within 30 days for THA and TKA, respectively. The most common cause of readmission within 30 days following total joint arthroplasty was infection. Trauma was the second most common reason for readmission of a THA while wound dehiscence was the second most common cause for readmission following TKA. With univariate regression, there were multiple associated factors for readmission among THA and TKA patients, including body mass index, metabolic equivalent (MET), and CCI. Multivariate regression revealed that hospital length of stay was significantly associated with 30-day readmission after THA and TKA.
Conclusion:
Patient comorbidities and preoperative functional capacity significantly affect 30-day readmission rate following total joint arthroplasty. Adjustments for these parameters should be considered and we recommend the use of CCI and METs in risk adjustment models that use 30-day readmission as a marker for quality of patient care.
Level of Evidence:
Level III/Retrospective cohort study
Keywords
Introduction
Lower extremity total joint arthroplasty ranks among the most common and effective surgical procedures, with nearly one million cases performed in the United States annually. 1 –3 However, surgical delay in patients undergoing total hip arthroplasty (THA) and total knee arthroplasty (TKA) may cause undue disruption in surgeon and hospital resource utilization. 4,5 In addition, readmission after elective total joint arthroplasty negatively impacts quality of treatment and hospital expense. Recently, several articles have identified the short-term readmission rates (ranging from 2.9% to 15.6%) after elective primary TKA and THA within 30 and 90 days. 6 –17 To our knowledge, most analyses utilized the dataset from American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP), which did not link readmissions with the primary diagnosis for readmission nor did the studies identify the correlation between comorbidities and readmission using the Charlson comorbidity index (CCI). 18,19
The aim of our study is to use our internal electronic database to (1) identify the incidence and risk factors for 30-day readmission in THA and TKA; (2) to identify any correlation of CCI in lower extremity total joint arthroplasty patients with readmission; and (3) to determine the primary cause of readmission in THA and TKA.
Methods
Data
After institutional review board approval, retrospective data were collected for patients who underwent elective primary THA and TKA between January 1, 2008, and December 31, 2013. Each author certifies that his institution has approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
A total of 2518 patients underwent total joint arthroplasty between 2008 and 2013 with ICD-9 procedure code 81.51 (THA) and 81.54 (TKA). Patients were excluded if (1) they were transferred to another hospital during their initial admission and (2) patients had an indisputably planned readmission (e.g. readmission for the second stage of a staged bilateral arthroplasty or another joint arthroplasty). After exclusion, there were 2481 patients (1225 THA and 1256 TKA) available for statistical analysis. All patients underwent THA or TKA by four adult hip and knee specialist surgeons in our institute.
We collected demographic and clinical data, including age, gender, body mass index (BMI), hospital length of stay (LOS), and the presence of medical comorbidities.
Preoperative comorbidities included obesity, smoking, alcohol use, use of an anticoagulant, corticosteroid use for a chronic condition, diabetes mellitus with or without end-stage organ failure, asthma, chronic obstructive pulmonary disease, hypertension, congestive heart failure, previous myocardial infarction, previous cardiac surgery, peripheral vascular disease, chronic kidney disease, malignancy, and connective tissue disease (SLE; Systemic lupus erythematosus22, rheumatoid arthritis). CCI was applied to identify the correlation of preoperative comorbidities and readmissions. Metabolic equivalents (METs) were utilized as an indicator of preoperative physical activity capability and exercise tolerance. 20 METs were stratified as follows: (1) 1–4 (low intensity), (2) 5–7 (moderate intensity), and (3) ≥8 (high/vigorous intensity). Causes of osteoarthritis (OA) were stratified into three groups: (1) primary OA (defined as an idiopathic condition developing in previously undamaged joints in the absence of an obvious causative mechanism), (2) secondary OA (defined as the presence of an obvious causative mechanism—not including traumatic cause), and (3) post-traumatic OA (OA caused by previous trauma or fracture). The American Society of Anesthesiologists (ASA) class was used as an indicator for preoperative burden of comorbidities. 21,22 ASA class I defines as healthy patients; ASA class 2 is mild-to-moderate systemic disease caused by a surgical condition or by other pathological processes, and medically well controlled; ASA class 3 is a severe disease process, which limits activity but is not incapacitating; ASA class 4 is a severe incapacitating disease that is a constant threat to life; ASA class 5 defines as moribund patients; and ASA class 6 is declared as a brain-dead patient. Operative variables included total operative time, operative blood loss, and days from operation to discharge (hospital LOS).
All patients readmitted within 30 days of discharge following a primary total joint arthroplasty were identified. Unplanned readmission was divided into two etiological categories: (1) Surgical factor associated with readmission and (2) medical factor associated with readmission. The proportion of readmission due to each cause was reported with a focus on the top 10 causes, as defined by Centers for Medicare and Medicaid Services (CMS).
Statistical analysis
We stratified patient data into readmitted and nonreadmitted cohorts and compared demographic variables, preoperative comorbidities, including CCI, 18,19 preoperative activity level measured by METs, 20 etiology of OA (primary, secondary, and posttraumatic), operative characteristics, and hospital LOS. The Pearson’s χ 2 test and the Fisher’s exact test, when appropriate, were applied to compare differences in categorical variables. Differences in continuous variables were evaluated with the Student’s t-test.
Univariate logistic regression was used to identify predictors of THA (Table 1) and TKA (Table 2) readmission, which were analyzed separately. To assess the simultaneous effects of the predictors of readmission, we further applied a multivariate logistic regression model (Table 4). Variables with chart completion rates of less than 80% were excluded to avoid model skewing. Results were reported as odds ratios (ORs) and its 95% confidence intervals (CIs). Model performance was evaluated through the c-statistic and Hosmer–Lemeshow model calibration statistic. 23 Statistical analysis was performed using SAS 9.3 (SAS Institute, Cary, NC, USA) with statistical significance set to p <0.05.
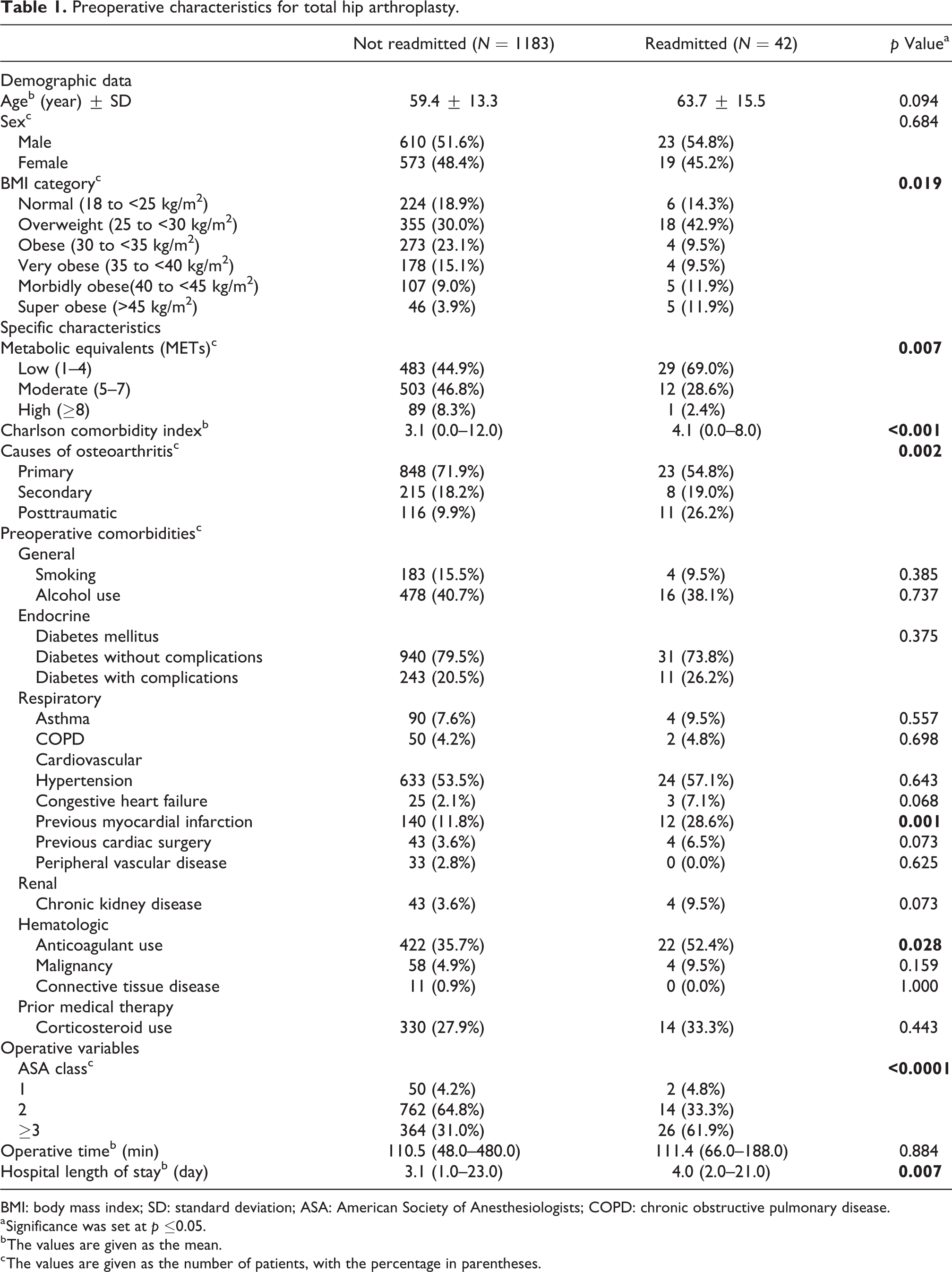
Preoperative characteristics for total hip arthroplasty.
BMI: body mass index; SD: standard deviation; ASA: American Society of Anesthesiologists; COPD: chronic obstructive pulmonary disease.
a Significance was set at p ≤0.05.
b The values are given as the mean.
c The values are given as the number of patients, with the percentage in parentheses.
Preoperative characteristics for total knee arthroplasty.

BMI: body mass index; SD: standard deviation; ASA: American Society of Anesthesiologists; COPD: chronic obstructive pulmonary disease.
a Significance was set at p ≤0.05.
b The values are given as the mean.
c The values are given as the number of patients, with the percentage in parentheses.
Results
Demographic characteristics, specific characteristics, and preoperative comorbidities
This study identified 2481 patients who underwent THA and TKA from our hospital database. There were 42 patients (3.4%) after THA and 28 patients (2.2%) after TKA who were unexpectedly readmitted within 30 days of their initial discharge. Demographic characteristics, specific characteristics (cause of OA, MET, and CCI), preoperative comorbidities, and operative characteristics of THA and TKA are listed in Tables 1 and 2, respectively. Univariate analysis of demographics demonstrated that a higher BMI was significantly associated with readmission in THA (p = 0.019) and TKA (p = 0.04). Female sex was significantly associated with readmission only for TKA (p = 0.029).
Specific characteristics were identified between the readmitted and nonreadmitted cohorts. Those who were readmitted in THA (69% vs. 44.9%; p = 0.007) and TKA (66.7% vs. 41.9; p = 0.026) had low preoperative physical activity (METs 1–4). Higher CCI was significantly correlated with readmissions within 30 days after both THA (4.1 vs. 3.1; p
There were several significant associations between patient comorbidities and 30-day readmission following THA and TKA. Readmission after THA had significantly higher rates of previous myocardial infarction (28.6% vs. 11.8%; p = 0.001) and anticoagulant use (52.4% vs. 35.7%; p = 0.028) while readmission after TKA had significantly higher rate of diabetes mellitus with complications (53.6% vs. 31.2%, p = 0.012) and hypertension (89.3% vs. 64.7%; p = 0.008).
With regard to the operative variables, readmission after THA (61.9% vs. 31.0%; p < 0.0001) and TKA (57.1% vs. 36.0%; p = 0.008) had significantly higher rates of patients with ASA class 3, while the majority of the nonreadmitted patients were ASA class 2 both after THA (64.8% vs. 33.3%; p < 0.0001) and TKA (61.9% vs. 35.7%; p = 0.008). Longer hospital LOS correlated with readmission (4.2 days vs. 3.1 days; p = 0.007 for THA and 4.2 days vs. 2.9 days; p = 0.015 for TKA).
Incidences and postoperative causes of 30-day readmissions
Incidences of 30-day readmission (Table 3) were 3.4% and 2.2% for THA and TKA, respectively. The most common cause of readmission within 30 days following total joint arthroplasty in lower extremity was infection. Trauma was the second most common readmission for THA while wound dehiscence was the second most common readmission for TKA. There were comparable rates of surgical causes for readmission in THA and TKA (78.6% vs. 78.6%) as well as medical causes for readmission (21.4% vs. 21.4%) in THA and TKA.
Causes of readmission within 30 days.

THA: total hip arthroplasty; TKA: total knee arthroplasty; PPF: Periprosthetic fracture; GI: Gastrointestinal disease.
Adjusted OR
Multivariate regression analysis was applied to control for confounders due to multiple predictive factors of readmission, as given in Table 4. The calculated c-statistic was 0.786 for THA and 0.833 for TKA, denoting high predictive value. Patients with post-traumatic OA of the hip had approximately 2.6 times higher likelihood of readmission than those with primary OA. Longer hospital LOS was independently associated with a higher likelihood of readmission both after THA (OR 1.125; 95% CI 1.003–1.262; p = 0.044) and TKA (OR 1.399; 95% CI 1.184–1.652; p < 0.0001).
Multivariate regression of readmission after total hip and total knee arthroplasty.

THA: total hip arthroplasty; OA: osteoarthritis; TKA: total knee arthroplasty; BMI: body mass index; SD: standard deviation; ASA: American Society of Anesthesiologists; COPD: chronic obstructive pulmonary disease; PTOA: Post-traumatic osteoarthritis.
a The values are given as the odds ratio with 95% confidence intervals in parentheses.
b Significance was set at p <0.05.
c Odds ratio for continuous variables represent increases in likelihood per unit change with a c-statistic of 0.786 for THA and 0.833 for TKA.
Discussion
Readmission after elective surgery has received increasing national attention as a result of recent changes to the CMS readmission reduction program. 24 –26 The goal of our study was to analyze our hospital patient database to determine the incidence, risk factors, and primary etiology of 30-day readmission after elective THA and TKA at our institution. Our findings corroborate a previous large-scale ACS-NSQIP study regarding 30-day readmission following THA and TKA in which Pugely et al. identified multiple comorbidities, which are associated with readmission. 11 Using our own hospital electronic patient database, we built upon previous literature by reporting our experience with THA and TKA readmission with respect to etiology. In this regard, surgical factors accounted for roughly four times higher readmission rates for both THA and TKA. The most common surgical cause for readmission was infection for both THA and TKA, while the second most common diagnosis among total hip readmissions was trauma (nine posterior hip dislocations, two periprosthetic femoral fractures, and one distal tibial fracture), and for total knee readmission, wound complication. Overall, our 30-day readmission rates were lower than those reported previously. 7 –12
Univariate analysis identified that high BMI was associated with increasing 30-day readmission rates both in THA (p = 0.019) and TKA (p = 0.040). For THA, morbid obesity (40 to <45 kg/m2) and super obesity (>45 kg/m2) were a significant risk factor for readmission within 30 days while very obese (35 to <40 kg/m2) and super obese (>45 kg/m2) were a predictor for readmission in TKA. Our findings were consistent with several previous studies, which showed that obesity was a predictor of readmission of total joint arthroplasty within 30 and 90 days. 27 –30 Our multivariate regression model demonstrated that morbid obesity (OR 2.2; CI 0.601–8.155) and super obesity (OR 3.5; CI 0.922–13.505) were significantly associated only with readmission after THA. This finding was in agreement with a previous study by Mednick et al., who found that the BMI of ≥40 kg/m2 is an independent risk factor for readmission following THA. 30 As obesity in the American population is increasing, the present data are helpful for counseling patients and for risk adjustment when evaluating readmission as a quality metric.
The ASA classification has been widely accepted as a reliable prognosticator for perioperative morbidity. 31 Traditionally, this parameter is used to understand and predict a patient’s ability to tolerate the stress of surgery and to compensate physiologically during and after general anesthesia. Patients with higher ASA class have been shown to have higher complication rates after multiple orthopedic procedures. 32,33 Analysis of our hospital database showed that similar to previously reported national data, patients readmitted to the hospital within 30 days of an elective THA or TKA had a higher ASA class. 8,11 Surgeons and care providers should exercise caution and thoroughly counsel when offering elective total joint arthroplasty to patients with a greater burden of systemic illness.
MET or exercise tolerance is a surrogate marker for functional capacity or physical activity level, defined by Jetté et al. 20 We hypothesized that this parameter may be relevant in the postoperative period in TJA as patients begin the rehabilitation process. To our knowledge, no current literature has sought to define the relationship between MET and readmission rates following total joint arthroplasty. Our study found that low METs were strongly associated with readmission after THA (p = 0.0007) and TKA (p = 0.026). This finding is useful for patient counseling, as those with low levels of preoperative physical activity tend to have a higher risk of hospital readmission.
Patient systemic illness, documented by patient comorbidities, has been shown to affect readmission after TJA. 11,12,15,16 Our results establish that a higher CCI is an independent risk factor for readmission. Our data is in keeping with previous analyses of CCI, which demonstrate that higher CCI is associated with higher health care costs 34 and higher incidence of postoperative complication. 35 Prior authors have found that CCI >1 is associated with increased 2 years mortality risk after proximal femur fractures. 36 Others have identified CCI ≥2 as a predictor of surgical site infection following total joint arthroplasty. 37 The utility of the CCI rests in the fact that it serves as a marker for the summation of systemic illness in a particular patient. Our study demonstrated that this simple-to-calculate parameter is a strong predictor of readmission after elective TJA.
Our study possesses several limitations. First, there is a limitation to quality of data, which are collected while providing care. For example, comorbidities documented are at the discretion of the treating physician so information regarding patient systemic illness may be incomplete. This would affect our calculation of the CCI for patients. Also, the retrospective nature of the study imposes the inherent limitation that patient data are not obtained according to a standard protocol. Second, we sampled only a portion of the THA and TKA patients in the time period of interest for convenience of data collection. Therefore, although sampling was random, we cannot entirely exclude a selection bias in our sample. Third, our sample size was modest compared with large national studies, so we may have failed to detect subtle statistically significant differences in the multiple parameters analyzed.
Conclusion
Patient comorbidities and preoperative functional capacity significantly affect 30-day readmission rates following total joint arthroplasty. Adjustments for these parameters should be considered and we recommend the use of CCI and METs in risk adjustment models that use 30-day readmission as a marker for quality of patient care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.