
Abstract
Introduction:
The bone–implant junction is a potential site for aseptic loosening. Extracortical bone bridging at the bone–implant junction is advocated to improve implant fixation by forming a biological seal. We propose a novel technique with vascularised bone graft (VBG) to form an extracortical bone bridge at the bone–implant junction to enhance implant stability. We compared the clinical and radiological outcomes for tumour megaprostheses performed (1) with and without bone graft and (2) with non-vascularised versus VBG technique.
Methods:
Forty-six tumour megaprosthesis procedures from 1 June 2007 to 31 October 2017 were identified from hospital records. Twenty-eight operations incorporated bone graft at the bone–implant junction, and 18 did not. Of these 28 bone graft procedures, 13 involved VBG, and 15 did not (non-VBG). The VBG technique involves resecting a short segment of healthy bone beyond the oncological margin with its preserved blood supply, splitting it, then securing it over the junction. Clinical outcomes assessed included loosening, fracture and recurrence. Extracortical bone growth at the bone–implant junction was quantified radiologically at intervals 0–24 months post-operatively. The mean follow-up was 4.27 years.
Results:
There were five incidences (27.8%) of loosening in the non-bone graft group compared to zero in the bone graft group (p = 0.03). There was a higher radiological score of extracortical bone growth in the bone graft group compared to no bone graft at 3–24 months post-operatively (p < 0.05). Within the bone graft group, the VBG group fared superior at 6 and 12 months post-operatively compared to non-VBG (p < 0.05), as well as a lower rate of radiological junctional resorption (p = 0.04).
Conclusions:
We recommend bone grafting for its merits of less implant loosening. We propose the VBG technique to combat early aseptic loosening in megaprosthesis replacement as there was a higher radiological score compared to non-VBG.
Keywords
Introduction
The bone–implant junction is often a culprit site of aseptic loosening in endoprosthetic replacement. In a study of 230 patients with tumour endoprosthetic replacement, 47% required revision surgery for aseptic loosening. 1 Extracortical bone bridging at the bone–implant interface has been advocated to improve implant fixation by forming a biological seal from wear debris generated by the articulating surface. 2,3 The extracortical bone bridging also transfers stresses across the bone–implant junction for additional implant stability. 2 –7
Different techniques have been proposed to promote extracortical bone bridging with varying success. 2 –7 Femoral endoprostheses with incorporation of hydroxyapatite-coated collars have shown a low rate of revision due to aseptic loosening (8%). Histological analysis shows bone growth into the hydroxyapatite-coated collar. 6 There was also extracortical bone bridging reported with porous implants. 2,5,7 There is still controversy over the survivorship of cemented compared to cementless implants. One study shows the survival of cemented to cementless endoprostheses due to aseptic loosening at 60 months to be 94% and 96%, with no significant difference. 8 The implants used in our study were all cemented.
Bone grafting at the bone–implant junction can enhance extracortical bone bridging, commonly with the use of allograft or iliac crest autograft. 2,9,10 Vascularised bone grafts (VBGs) are used often in tumour surgery in the reconstruction of long segmental bone defects; 11 however, there are no current studies that utilize a VBG at the bone–implant junction to improve loosening rates.
We propose a novel technique of using a VBG to form an extracortical bone cuff at the bone–implant junction to improve implant stability. We aim to compare the clinical and radiological outcomes for patients with tumour endoprostheses performed with non-vascularised versus VBG technique. Our secondary objective is to compare megaprostheses performed with and without bone grafting, to show that the bone grafting technique itself is advantageous pertaining to the outcomes. This is to highlight that the VBG technique (primary objective) has additional benefits over conventional nonvascularised bone grafting when compared to no bone grafting.
Methods
From 1 June 2007 to 31 October 2017, 46 tumour endoprosthesis replacement procedures were identified from hospital records at a single institution. Twenty-eight of the operations incorporated the use of bone graft at the implant–bone junction, and 18 had no bone graft. Of these 28 bone graft procedures, 13 incorporated VBG, and 15 of the patients had a non-VBG at the bone–implant junction (Figure 1). In the non-VBG group, all bone graft used was autogenous, originating from either the iliac crest or part of the resected bone free of tumour. The baseline characteristics were comparable between the groups (no bone graft vs. bone graft and non-VBG vs. VBG), including gender, age, malignant nature of the tumour, surgical site and implant type (p > 0.05), shown in Tables 1 and 2, respectively. The implants used were all cemented. The materials of the implant stem varied with the majority of stems being titanium or cobalt chrome alloy. The mean follow-up time was 4.27 years.
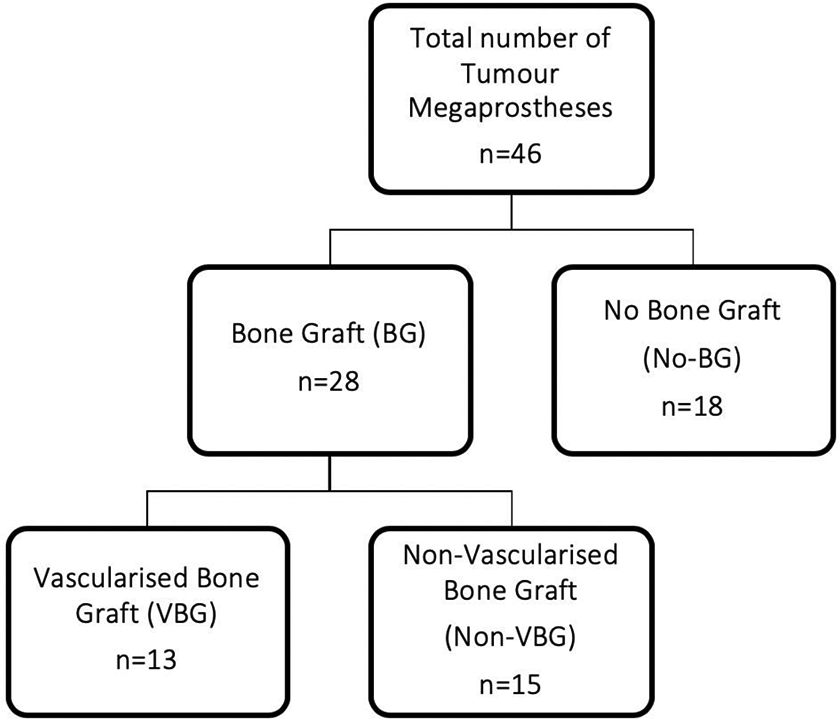
Study groups.
Baseline characteristics: no bone graft versus bone graft at the bone–implant junction.

HA: hydroxyapatite.
Baseline characteristics: non-vascularised versus VBG at the bone–implant junction.
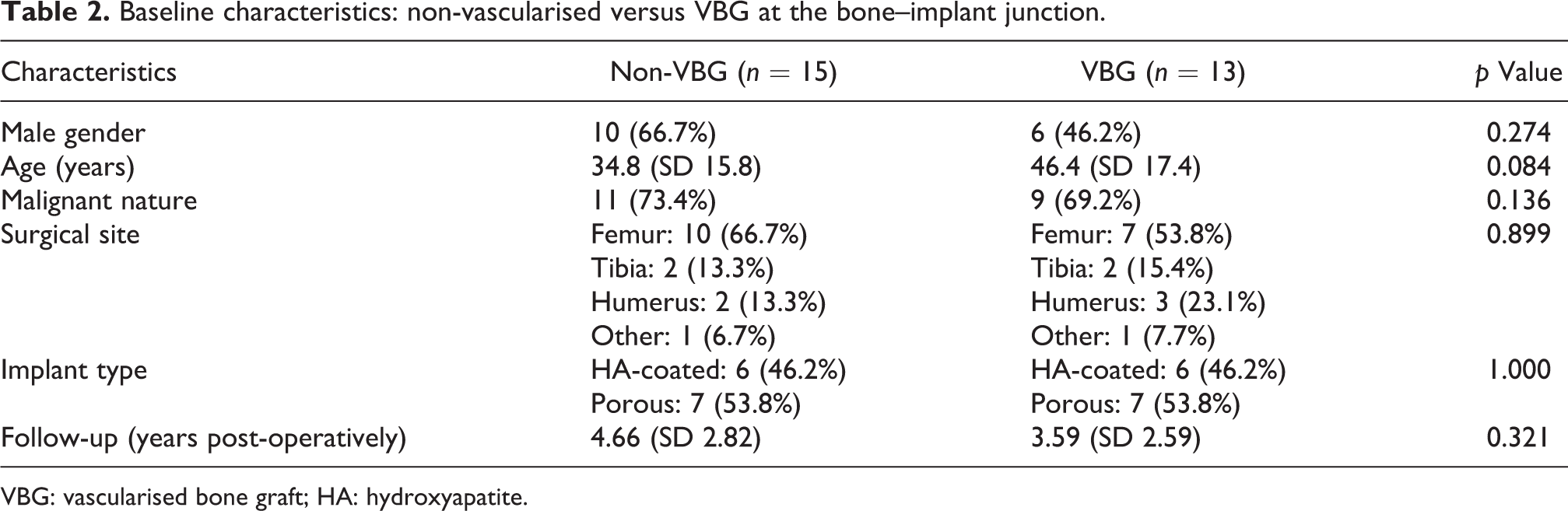
VBG: vascularised bone graft; HA: hydroxyapatite.
The VBG technique involves resecting a short segment of healthy bone beyond the oncological margin with its preserved blood supply, splitting it into thirds longitudinally, then securing it over the junction with the use of cables (Figures 2 and 3).

The VBG technique. VBG: vascularised bone graft.

Intraoperative photo of the VBG technique at the bone–implant junction. VBG: vascularised bone graft.
Clinical outcomes were assessed including the rate of loosening, fracture and recurrence. Extracortical bone growth at the implant–bone junction was quantified radiologically at intervals from 0 months to 24 months post-operatively according to the scoring by Coathup et al. 6 A score of 1 represents extracortical bone in contact with the implant surface in any one of the four (anteroposterior and mediolateral) zones in anteroposterior and lateral radiographs, with a maximum score of 4. Junctional resorption of bone at the bone–implant junction was also assessed (Figure 6).
Statistical analysis was performed using SPSS Statistics version 24 (IBM Corp., Armonk, New York, USA). The χ 2 test was used for categorical variables, the independent samples t-test for continuous variables and Mann–Whitney U test for ordinal variables. Significance level was set at p < 0.05.
Results
No bone graft versus bone graft
There were five incidences (27.8%) of loosening in the non-bone graft group compared to zero in the bone graft group (p = 0.003). There were no significant differences in other surgical complications including neurovascular injury, fracture or local recurrence (Table 3). There was a higher score of extracortical bone growth in the bone graft group compared to the non-bone graft group at 3, 6, 12 and 24 months post-operatively (p < 0.05) (Figure 4). There was no significant difference in the score at 0 months.
A comparison of complication rates.

VBG: vascularised bone graft.
a Significant at p < 0.05. Non-VBG versus VBG.

Radiological scoring for extracortical bone bridging at the bone–implant junction in the post-operative period for non-bone graft versus bone graft groups: (a) 3 months, (b) 6 months, (c) 12 months and (d) 24 months (*significance at p < 0.05).
Within the bone graft group, the VBG group fared significantly better at 6 months and 12 months post-operatively compared to the non-VBG group in terms of radiological scoring (p < 0.05) (Figure 5). There was a significantly lower rate of radiological junctional resorption in the VBG group compared to the non-VBG group (p = 0.04), although the significance of radiological junctional resorption on loosening remains to be elucidated (Figure 6). There were no significant differences in surgical complications including loosening rates, neurovascular injury, fracture or local recurrence between these groups (Table 3).

Radiological scoring for extracortical bone bridging at the bone–implant junction in the post-operative period for VBG versus non-VBG groups: (a) 3 months, (b) 6 months, (c) 12 months and (d) 24 months (*significance at p < 0.05). VBG: vascularised bone graft.

Radiological junctional bone resorption at the bone–implant junction (white arrow).
Discussion
The use of bone graft at the bone–implant junction shows significantly lower rates of loosening (0%) compared to the megaprostheses without bone grafting (27.8%). This is supported in literature by other studies illustrating the advantages of bone grafting at the bone–implant junction. Tanzer et al. showed that autogenous bone grafting of the bone–implant junction of a tumour endoprosthesis consistently results in the formation of extracortical bone radiologically in all 20 of their patients at a mean of 28 months post-operatively. 9 In canine models, bone grafting at the bone–implant junction showed a significantly greater callus area radiologically and increased mechanical strength compared to ungrafted models. 10
The common sources for bone graft are autograft from the iliac crest or allograft. However, there have been reported complications with iliac crest bone graft with reported morbidity rates of up to 49%. 12 In particular, patients may complain of post-operative chronic pain, thigh numbness or haematoma formation. 13 With allografts, transmission of disease or infection is a risk. These complications may be avoided with the use of the VBG technique, as the bone graft is fashioned with just an extra segment of bone just beyond the usual osteotomy site, with no additional donor site morbidity or functional impairment. From this study, there were no significant complications including neurovascular injury, recurrence or fracture in the VBG group when compared to the non-VBG group.
Vascularised bone grafting has been used extensively in tumour surgery, especially in the reconstruction of cases with large segmental bone defects. 11 In contrast to non-vascularized bone graft, VBG does not undergo creeping substitution, thus can maintain their structural integrity. The use of a VBG has the advantages of improved blood supply for an optimal environment for bone growth. The VBG technique involves the preservation of a soft tissue cuff for vascular supply to the bone graft and can be performed without the technical challenges of microsurgical anastomosis used in larger free VBGs. There is no additional protected weight bearing required in contrast to the larger VBGs. The advantages of VBG may be reflected in the significantly higher radiological score compared to non-VBG from 6 months up to the first year post-operatively. Figure 7 shows excellent incorporation of the VBG at 6 months post-operatively. The VBG group also shows a significantly lower junctional resorption rate. There are limited studies looking into radiological junctional resorption. Whether this is a possible precursor or a risk factor to loosening may be further investigated.
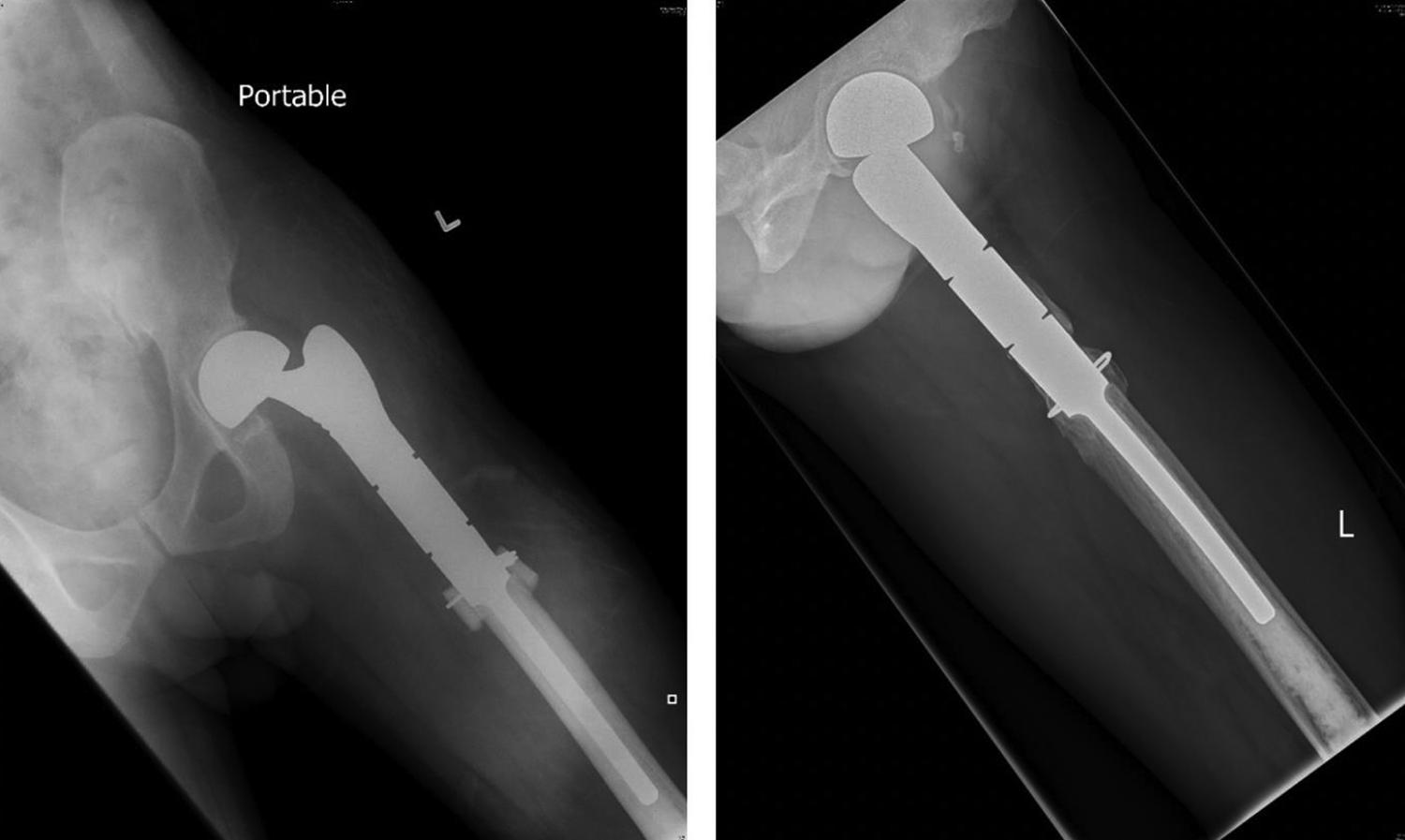
Post-operative radiographs of left proximal femur megaprosthesis show good incorporation of the VBG at the bone–implant junction at 6 months post-operatively (right) compared to 0 months post-operatively (left). VBG: vascularised bone graft.
There are some limitations to our study. It is a retrospective study with data collected over 10 years. Regarding the technique, our method is used to enhance the bone–implant junction and is not suitable for large bone defects or reconstructive purposes.
Despite the radiological advantages of the VBG technique, our study has failed to show a difference in the loosening rate compared to non-vascularised bone grafting. The rate of megaprosthesis loosening ranges from 5% to 10% and also depends on the location of the reconstruction, with the distal femur having the highest rates of loosening. 14 Our small study group size was a limitation to the study. Perhaps with a larger sample size, we will be able to detect more loosening. However, overall the results are very promising and further studies on this technique should be pursued.
Conclusions
Bone grafting was associated with a lower rate of loosening. There was significantly more radiological extracortical bone bridging in the VBG technique compared to non-VBG from 6 months up to the first year post-operatively. We propose the VBG technique as a simple and effective technique to combat early aseptic loosening in endoprosthetic replacement without additional complications or donor-site morbidity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.