
Abstract
Purpose
The proximal femur is a region frequently affected by pathological fractures due to metastases. Partial head megaprostheses are among the surgical options that can be preferred for treating pathological fractures in this area. The aim of this study is to evaluate the impact of various factors on the functional outcomes and mortality of patients with actual proximal femoral fractures treated with a megaprosthesis.
Methods
The study included 28 patients. None of these patients had impending fractures; all of them had actual pathological fractures. Functional outcomes were assessed using VAS improvement, MSTS, and KPS scores, in relation to factors including age, cancer diagnosis before fracture, additional fracture, bone metastasis, visceral metastases, postoperative oncological treatment, preservation of the trochanter major, and type of cancer. These same factors were also considered in the survival analysis. The impact of knowing the cancer diagnosis prior to the fracture on time to surgery was also evaluated.
Results
Patients showed a mean VAS improvement of 5.8 ± 1.3, with median postoperative MSTS and KPS scores of 18 (range:12–23) and 65 (range:40–80), respectively. Younger patients had significantly better functional outcomes (p < 0.05). Other clinical factors had no significant effect on functions. Visceral metastases negatively impacted survival (p = 0.044), while younger age (p = 0.029), favorable cancer type (p < 0.001), and receiving postoperative oncological treatment improved survival (p = 0.049). Time to surgery was longer in patients without a prior cancer diagnosis (p < 0.001), though this did not affect survival (p = 0.888).
Conclusion
Megaprostheses in the treatment of actual metastatic fractures of the proximal femur provide excellent pain relief and satisfactory functional improvement. Functional outcomes were associated with age, while survival was influenced by age, cancer type, presence of visceral metastases, and whether postoperative oncological treatment was received. Although the preoperative time to surgery was longer in patients without a prior cancer diagnosis, survival was not affected by whether the diagnosis was known before the fracture.
Level of Evidence
IV.
Introduction
Metastatic diseases of the bone are more common than primary bone tumors. 1 One of the regions most affected by metastatic involvement in bone tissue is the proximal femur.2,3 The hip joint is subjected to different loads at various angles, experiencing significant biomechanical stress. The microstructure of the proximal femur can be disrupted by metastases or primary bone tumors. 4 Due to the effects on the bone structure and microarchitecture, the load-bearing capacity and resistance of the proximal femur to stress may be impaired. In such cases, impending pathological fractures may develop, or actual pathological fractures can occur even without severe trauma. 5
Fractures are injuries that can cause severe pain and functional loss even in normal patients. Cancer patients, considering the debility, pain, and functional losses caused by their primary disease, may struggle significantly when faced with an additional fracture injury. Hip fractures are known to have a high mortality rate. 6 Therefore, surgical treatments should be applied as early as possible in the management of hip fractures to enable early mobilization. By selecting appropriate surgical treatments, patients’ pain can be relieved, their function restored, and their survival improved. In cases of proximal femur fractures caused by metastasis, the primary objectives of treatment are pain management and promoting functional recovery. Successful surgical treatment of these fractures is believed to prevent the mortality associated with hip fractures themselves and allow patients to spend their remaining life, shortened by cancer, in relatively greater comfort. 7 One of the key treatments for pathological fractures of the proximal femur is the resection of the tumor-affected area and reconstruction of the joint with megaprostheses.
Numerous studies in the literature have investigated the treatment of proximal femoral pathological fractures with megaprostheses. However, in most of these studies, actual pathological fractures and impending fractures have been evaluated together.7–14 It is well established that interventions for impending fractures before the occurrence of an actual fracture are clinically valuable and beneficial to patients. Nevertheless, there are opinions suggesting that actual fractures have intraoperative and postoperative disadvantages compared to impending fractures. 15 In the present study, we examined patients with actual pathological fractures of the proximal femur caused by metastasis. The aim of this study was to evaluate the impact of various factors on the functional outcomes and mortality of patients with actual proximal femoral fractures treated with a megaprosthesis.
Materials and methods
Study design and setting
This study was a retrospective study. It was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the local ethics committee (XXX University, Date: 10.09.2024, Number: 2024/445). The study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The data were retrieved from the hospital’s electronic archives and the clinical archives, where detailed manual recordings of patient measurements were maintained. The study was conducted in the orthopedics department of a university hospital. Within this hospital, there is an orthopedic oncology council that includes an orthopedic surgeon, an oncologist, a radiation oncologist, a radiologist, and a pathologist, all dedicated to the treatment of orthopedic oncology patients. Treatment decisions are made by this council.
Patients
Between 2011 and 2024, 47 patients with actual pathological fractures of the proximal femur due to metastasis were identified from clinical archives. All of these patients presented with actual pathological fractures, and none of them had impending fractures. Three patients who died before surgery due to general health deterioration, seven patients treated with intramedullary nail (IMN), and nine patients who received prostheses with acetabular components were excluded from the study. The remaining 28 patients, who had been treated with a megaprosthesis with a bipolar head, were included in the study. Of these patients, 15 were male and 13 were female, with an average age of 65.4 ± 12.6 years. Among those with pathological fractures in the proximal femur, four fractures were located in the femoral neck, six in the intertrochanteric region, and 18 in the subtrochanteric region. In four patients, another bone fracture accompanied the proximal femur fracture (three patients had humerus fractures, and one had a rib fracture). The primary cancer diagnoses were as follows: breast cancer in seven patients, lung cancer in seven, renal cell carcinoma in six, prostate cancer in three, hepatocellular carcinoma in one, neuroendocrine tumor in one, uterine cancer in one, bladder cancer in one, and pancreatic cancer in one patient. Sixteen patients were known to have a previous cancer diagnosis at the time of the fracture, while 12 were diagnosed after the fracture. Twenty-three patients had multiple bone metastases, while five had solitary bone metastasis. Visceral metastases were present in 13 patients.
Treatment plan, surgery and follow-up
All patients were discussed in the tumor council preoperatively to determine their treatment plan. In 17 patients, a biopsy was taken for pathological examination before the megaprosthesis was applied. In all patients, the tumor-affected area was resected, and a modular megaprosthesis with a bipolar head was implanted. In 16 patients, the greater trochanter was osteotomized and preserved due to the absence of trochanteric invasion, and it was subsequently reattached. In the remaining 12 patients, the presence of trochanteric invasion necessitated the resection of the mass along with the greater trochanter, and the gluteus medius was sutured to the surrounding soft tissue. The average resection length of the pathological area was 186 ± 45 cm. Tissue samples taken during surgery were sent for pathological examination to confirm the diagnosis.
As of October 2024, when the study data were analyzed, only six patients were still alive. The average follow-up period for the study’s patients was 16.9 ± 17.4 months. Four patients in the study died within the first 2 weeks postoperatively. Seven patients experienced serohemorrhagic discharge, and one patient developed a minimal sacral decubitus ulcer, which was treated with wound care and multiple dressings. One patient developed an infection within 2 weeks after surgery and underwent reoperation for debridement. Another patient developed deep vein thrombosis and was treated with low-molecular-weight heparin. Aside from these complications, no other issues, including dislocations, were observed. In addition to the megaprosthesis surgery, four patients underwent additional orthopedic procedures; three of these were for fractures in other areas, and one was for debridement due to infection. All patients participated in a gradual mobilization program as tolerated. Generally, bed mobility and sitting exercises began within the first 2–3 days post-surgery, and in the following days, patients were encouraged to bear partial weight with the help of a walker. Full weight-bearing was typically achieved by weeks 3–4. Postoperative follow-ups were conducted every 2 weeks during the first month, with monthly follow-ups performed during the first year. For patients who survived beyond 1 year, follow-ups continued every 3 months. During their postoperative follow-up, nineteen patients were noted to have received oncological treatment as determined by the oncology council. Trendelenburg gait was observed in 15 patients postoperatively.
Evaluations
Pain assessment was performed using the Visual Analog Scale (VAS) during both preoperative and postoperative periods. On this scale, patients rate their pain from 0 to 10, with higher scores indicating more severe pain. To assess pain relief, the difference between the patients’ preoperative and postoperative VAS scores was calculated and referred to as “VAS improvement”. Postoperative functional assessment was conducted using the Musculoskeletal Tumor Society (MSTS) score and the Karnofsky Performance Status (KPS) score. The MSTS score ranges from 0 to 30, with higher scores indicating better function. Similarly, the KPS score is evaluated on a scale of 0 to 100, with higher scores indicating better functionality. Pain and functional assessments were conducted in 24 patients, as four patients died in the early period. In addition, the relationships between the pain-functional scores and various factors such as age, cancer diagnosis before fracture, presence of additional fractures, multiple bone metastases, visceral metastases, postoperative oncological treatment, preservation of the greater trochanter, and cancer type were investigated.
Survival analysis was conducted based on patients’ age, cancer diagnosis before fracture, presence of additional fractures, multiple bone metastases, visceral metastases, postoperative oncological treatment, and cancer type. Survival analysis based on cancer types was performed by categorizing the cancers into three groups -slow, moderate, and rapid growing-according to the classification outlined by Katagiri et al. 16 For the analysis of the effect of receiving oncological treatment on survival, four patients who died early and did not have the opportunity to receive oncological treatment were excluded, leaving 24 patients for this analysis. All patients in the study were included in the other survival analyses. In the age-related survival analysis, patients were categorized into two groups: those under 65 and those aged 65 years or older, based on the World Health Organization’s classification of individuals aged 65 and above as “elderly”. The impact of knowing the cancer diagnosis prior to the fracture on the time to surgery was also evaluated.
Statistics
Assumptions of normality were evaluated using the Kolmogorov-Smirnov and Levene tests. For group comparisons, the independent samples t test and one-way ANOVA were used when the assumptions of normality and homogeneity of variance were met. In cases where these assumptions were violated, non-parametric alternatives such as the Mann-Whitney U test and the Kruskal-Wallis test were employed. Associations between categorical variables were analyzed using the Chi-square test. Survival curves were generated using the Kaplan-Meier method, and the log-rank test was used to compare survival rates. A p-value of ≤0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Pain relief and functional outcomes of patients.

Data presented as Mean ± SD or Median (IQR).
aSignificance levels were set at p ≤ 0.05.
SD: standart deviation; IQR: interquartile range; VAS: visual analog scale; MSTS: musculoskeletal tumor society score; KPS: Karnofsky performance status.
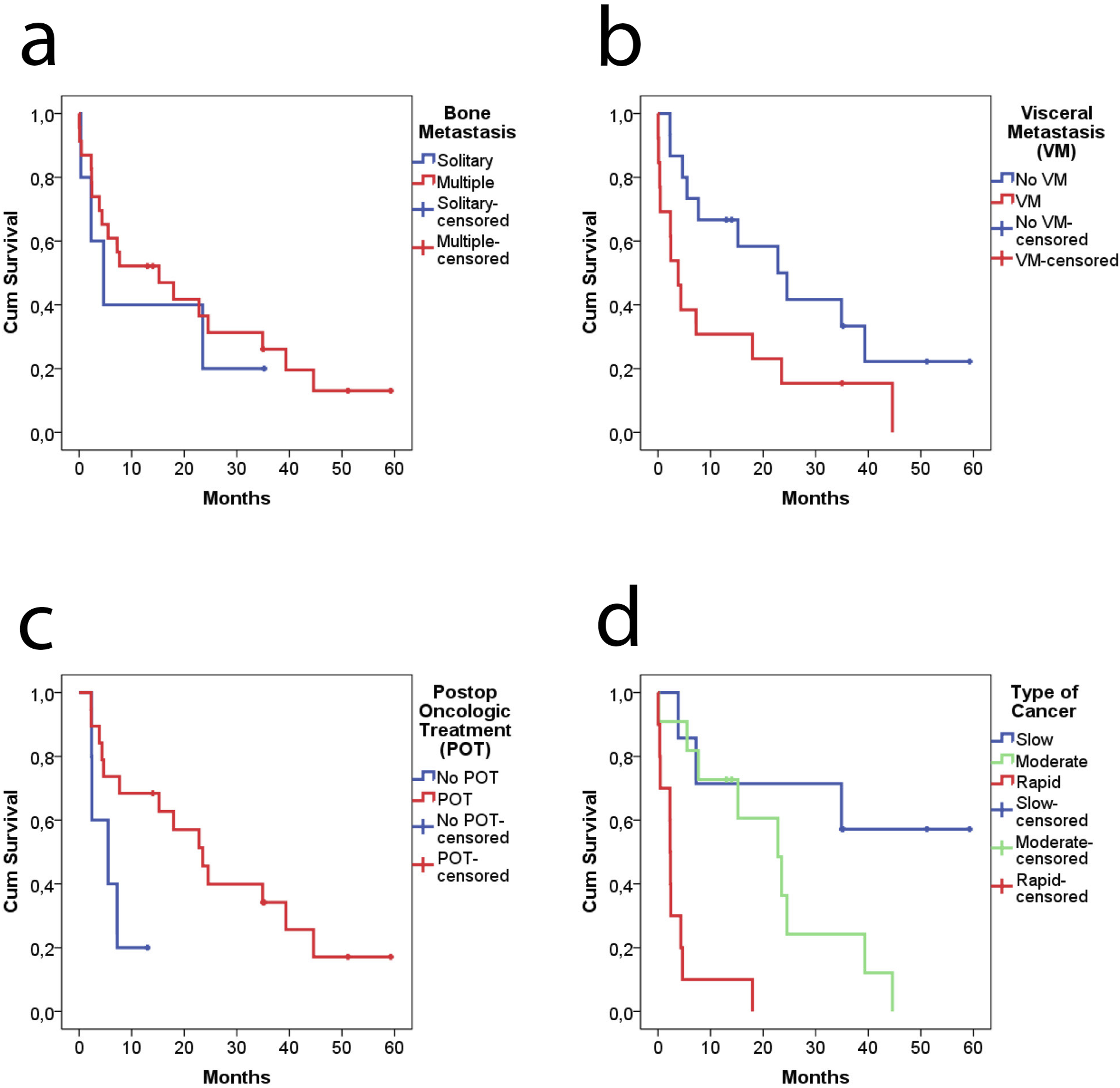
The overall survival of patients after receiving a megaprosthesis was 50% at 1 year, 33% at 2 years, and 25% at 3 years. Patients under the age of 65 years had better survival compared to those aged 65 years or older (p = 0.029) (Figure 1(a)). Whether or not the primary cancer was known before fracture development did not affect survival (p = 0.888) (Figure 1(b)). The presence of fractures in other regions did not influence survival (p = 0.613) (Figure 1(c)). While multiple bone metastases had no effect on survival (p = 0.616) (Figure 2(a)), visceral metastases were found to reduce survival (p = 0.044) (Figure 2(b)). Patients who received oncological treatment after megaprosthesis for the fracture had better survival outcomes (p = 0.049) (Figure 2(c)). The type of cancer significantly affected survival (p < 0.001) (Figure 2(d)). Kaplan-Meier survival curves showing the impact of age (a), cancer diagnosis before fracture (b), and additional fracture (c) in patients treated with megaprostheses for proximal femur pathological fractures. Kaplan-Meier survival curves showing the impact of bone metastasis (a), visceral metastasis (b), postop oncologic treatment (c), and type of cancer (d) in patients treated with megaprostheses for proximal femur pathological fractures.
The mean duration from the day of fracture to the megaprosthesis surgery was found to be 8.8 ± 2.1 days in cancer patients whose primary diagnosis was unknown at the time of the fracture. In patients with a known cancer diagnosis, this duration was 4.9 ± 2.3 days. A significant difference was observed between the two groups regarding the time from fracture to prosthesis surgery (p < 0.001). The mean hospital stay after the megaprosthesis surgery was 8.6 ± 7.5 days for patients with an unknown diagnosis, compared to 6.4 ± 4.2 days for those with a known diagnosis prior to the fracture. No significant difference was found between these two groups regarding the hospital stay duration after surgery (p = 0.873).
Discussion
With advancements in cancer treatments leading to improved survival rates, complications related to bone metastases, including pathological fractures, have also increased. 17 Bone metastases from cancers cause changes in bone structure, reducing their biomechanical strength. This leads to the development of pathological fractures, which can cause severe pain and significantly limit patients’ functionality. 18 Additionally, hip fractures, whether pathological or not, are injuries with high mortality rates and require early surgical intervention. This study aimed to identify the factors affecting functional outcomes and mortality in patients with actual pathological proximal femoral fractures managed with megaprosthesis. Additionally, the impact of knowing the cancer diagnosis prior to the fracture on the time to surgery was examined. The results of the study demonstrated that satisfactory functional outcomes were achieved with megaprostheses, and that patients younger than 65 years had better functional results compared to older patients. In terms of survival, it was observed that younger patients, those without visceral metastases, those who received postoperative oncological treatment, and patients with more favorable cancer types had lower mortality rates. Additionally, although the time from fracture to megaprosthesis surgery was longer in patients without a known cancer diagnosis prior to the fracture, it was observed that knowing the diagnosis beforehand did not affect survival.
This study specifically addresses a key gap in the existing literature: the majority of previous research has evaluated both actual pathological fractures and impending lesions of the proximal femur together,7–14 despite their differences. Surgical intervention for impending fractures is indeed clinically valuable, as it can prevent fracture related complications.19,20 However, once an actual pathological fracture occurs, an urgent intervention process is triggered, and the natural course of the affected extremity changes, partly due to hematoma formation and the potential invasion of healthy surrounding tissues. Previous studies have shown that treatment of actual fractures is associated with greater blood loss, increased transfusion requirements, longer anesthesia times, higher reoperation rates, and lower survival compared to impending fractures. 15 Furthermore, for patients presenting with a true fracture, the surgical procedure, resection, preoperative medical treatment, and preparation may be less comprehensive compared to patients undergoing surgery due to fracture risk. By focusing exclusively on patients with complete actual pathological fractures of the proximal femur treated with megaprostheses, our study ensures a homogeneous fracture type and directly evaluates various factors influencing functional and mortality outcomes that have not been comprehensively examined in this specific group before.
According to the results of this study, patients with actual pathological femoral fractures treated with megaprostheses achieved highly satisfactory outcomes in terms of both pain relief and functional scores. Additionally, this research systematically examined several factors believed to influence functional outcomes, yielding notably important results. While patients under the age of 65 demonstrated better functional outcomes, worse results were observed in older patients, which may be attributed to the natural decline in functionality associated with aging. Additionally, no significant impact of other factors on functional outcomes was found. These findings suggest that other commonly presumed prognostic factors may not have a meaningful impact on functional recovery in patients with actual pathological fractures. Therefore, in the context of treatment planning, these factors may hold limited value in predicting functional outcomes. Reviewing previous studies shows that the survival rates associated with proximal femur prostheses are quite favorable.7,9,10 However, the surgical technique and its success alone are not sufficient for the overall survival rate. In metastatic bone disease, factors contributing to poor prognosis include the presence of a primary malignancy with aggressive growth characteristics, abnormal and unfavorable laboratory findings (C-reactive protein, lactate dehydrogenase, serum albumin, serum calcium corrected for albumin level, platelet count, total bilirubin etc.), poor overall condition and performance status of the patient, the presence of visceral metastasis, and the absence of postoperative oncological treatment.8,16,21–23 In this study, consistent with previous literature, patients aged 65 years and older, those with visceral metastases, and those who did not receive oncological treatment after surgery were found to have poorer survival rates. Moreover, cancer type was significantly associated with survival.
It can be assumed that patients without a known cancer diagnosis prior to the fracture may experience longer waiting times for prosthesis surgery due to the diagnostic process. One reasonable hypothesis is that the time needed for these diagnostic steps could delay hip surgery and potentially increase mortality. Conversely, it could also be suggested that patients without a prior cancer diagnosis may have milder symptoms, making them clinically more stable and less frail. Therefore, it is possible that their mortality risk could be lower. In our analysis, the time to megaprosthesis surgery was indeed longer for patients without a known diagnosis compared to those with a known diagnosis. However, contrary to both hypotheses, whether the diagnosis was known or not did not have a significant impact on survival. When these results are considered together, it can be concluded that in the treatment of a patient with a proximal femur pathological fracture, it is crucial to avoid hasty decisions that could lead to errors. Instead, adhering to the diagnostic and treatment algorithms of orthopedic oncology and ensuring proper preoperative preparation to perform the surgery under optimal conditions are essential. Indeed, there are also views in the literature that support our findings. In a study by Varady et al., which included 2627 patients with pathologic hip fractures, they demonstrated that taking time to medically optimize patients before surgery did not adversely affect postoperative outcomes in terms of surgical complications and perioperative mortality. However, they have shown that the presence of disseminated disease is associated with increased morbidity and mortality. The authors also emphasized that surgery should not be delayed unnecessarily; but if the surgeon believes that additional time could benefit the patient, the operation should not be rushed. 24
In the management of pathological fractures, particularly in patients with an unknown primary tumor, inappropriate surgical interventions may result in irreversible consequences. 25 When a malignant bone lesion is identified, the possibility of a primary bone tumor must always be considered. A multidisciplinary approach is essential in the evaluation of such cases. In patients without a prior history of malignancy, the diagnostic work-up should include thoracic, abdominal, and pelvic CT imaging, PET-CT, laboratory investigations, and tumor marker analysis to identify the primary site. In patients with a known malignancy, a solitary bone lesion should be confirmed histologically via biopsy. However, in those with multiple lesions and a high likelihood of metastasis, further histological confirmation is generally unnecessary. 26 During the treatment planning phase, the patient’s overall medical condition and performance status should be thoroughly evaluated. The choice of surgical intervention should be tailored according to the anatomical location of the fracture. 27 Fixation methods and prosthetic options are prominent treatments for proximal femur pathological fractures. Hip fractures in normal patients can be successfully treated with intramedullary IMNs. However, when treating femoral metastatic pathological fractures with IMNs, the expectation of non-union is quite high. Therefore, in patients treated with IMNs, the risk of implant failure increases, especially due to the progression of osteolytic lesions.28,29 There is still ongoing debate regarding the method used; while some studies have demonstrated the superiority of megaprostheses,14,29,30 others have considered intramedullary IMNs to be a reasonable option.12,31,32 In our cohort, however, only patients who underwent megaprosthesis implantation were examined. Megaprostheses are a more invasive, more expensive, and complication-prone type of prosthesis compared to conventional prostheses. Additionally, the risk of dislocation is higher due to the resection of the gluteal muscles.33,34 In our study, none of the patients experienced dislocation. We believe this is due to the implementation of trochanter-preserving surgeries in patients without trochanteric involvement, as well as the suturing of the gluteal muscles in patients with trochanteric involvement. Indeed, previous studies have also reported series with no or very few instances of dislocation.7,35,36 However, a Trendelenburg gait was observed in 15 of the patients we treated, and it was found to be more prevalent in those who did not undergo trochanter-preserving surgery. Despite this, the Trendelenburg gait did not become a significant complaint for the patients, and no differences were observed in functional scores among patients without preservation of the greater trochanter. Patients were able to manage their daily functions despite this gait. Another common complication of megaprostheses is wound infections.36–39 Factors contributing to this issue may include the nature of the surgical procedures involving large areas, the relatively large size of the metallic implant, the formation of dead spaces, prolonged wound drainage, the inability to perform necessary pathogen screening due to the urgency of the surgery, and the weakened immunity associated with malignancy. In our study, a significant portion of the complications was due to prolonged wound drainage. Good wound monitoring and care were effective in overcoming these complications.
The main limitation of this study is its retrospective design and the relatively small sample size. This is largely due to the study’s focus on actual fractures rather than including impending fractures. Another limitation of this study is the heterogeneity observed in the pathological diagnoses of the included paitents. Differences in gender, age groups, medical treatments received, and survival rates are evident among the patients based on their pathological diagnoses. Therefore, future studies that focus on groups with the same primary cancer diagnosis may yield more valuable findings. Another important limitation is the absence of a comparative treatment group, such as patients treated with intramedullary nailing. Additionally, the retrospective design of the study and the fact that the study was conducted at a single center are also significant limitations.
Conclusion
This study examined the outcomes of partial modular megaprostheses in the treatment of metastatic proximal femur pathological fractures at a university hospital where orthopedic pathological fractures are referred. According to the results of the study, treating proximal femur pathological fractures with megaprostheses yielded highly satisfactory outcomes in terms of pain relief and functionality. Younger age was found to be the most significant factor positively influencing functional results, while other expected such as having a cancer diagnosis prior to fracture, presence of additional fractures, multiple bone metastases, visceral metastases, receiving postoperative oncological treatment, preservation of the trochanter major and cancer type showed no meaningful effect on functional outcomes. In terms of survival, favorable outcomes were observed in younger patients, those without visceral metastases, those who received postoperative oncological treatment, and those with more favorable cancer types. Although the time from fracture to megaprosthesis surgery was longer for patients without a known cancer diagnosis prior to the fracture, it was observed that whether the diagnosis was known beforehand did not affect survival.
Footnotes
Consent to participate
The Ethics Committee waived the requirement for informed consent, as the study was retrospective and used previously collected data. Therefore, obtaining informed consent from participants was not necessary according to national regulations.
Authors contributions
E.E. (first and corresponding author) Conceptualization, Methodology, Formal analysis, Writing - Original Draft, Writing - Review & Editing, Project administration
A.G. Validation, Investigation, Methodology, Writing - Original Draft
F.D. Data Curation, Formal analysis, Writing - Original Draft
S.Y Methodology, Formal analysis, Writing - Original Draft
B.K.A Writing - Original Draft, Writing - Review & Editing, Supervision. All authors have read and approved the final submitted manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received partial financial support from Selcuk University for the Article Processing Charge (APC).
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the local ethics committee. (Selcuk University, Date: 10.09.2024, Number: 2024/445).
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to the fact that they involve patient-related information obtained from the hospital but are available from the corresponding author on reasonable request.