
Abstract
Background:
Cementless femoral reconstruction is challenging in hip dysplasia due to deformity of the proximal femur causing insufficient stem fixation and/or inadequate neck anteversion. Strategies to address these problems include the use of a modular stem or a distal fixation stem, but both stems have some characteristic disadvantages.
Methods:
We studied the postoperative clinical outcomes in primary total hip arthroplasty in 257 hips using the flat tapered wedge short femoral stem for hip dysplasia in an Asian population (postoperative follow-up period: 2 years to 6 years and 11 months; mean 4 years and 5 months). We took advantage of the characteristic of high flexibility in stem placement because of its low volume, positioning it while performing some varus/valgus and rotational alignment adjustments.
Results:
Favorable clinical functional outcomes were obtained, including the radiographic outcome of biological fixation achieved in all stems. Regarding complications, there was no case of split fracture of the femoral calcar region during stem insertion, and the rate of postoperative dislocation was also low at 0.4% (1 case). In the pre- and postoperative computed tomography measurements, the variability in stem anteversion postoperatively was significantly reduced compared to preoperative anatomical anteversion.
Conclusion:
This flat-shaped short low-volume stem likely has high flexibility in positioning in cases of hip dysplasia and can be easily positioned to avoid fractures while still achieving secure fixation.
Introduction
Total hip arthroplasty (THA) for secondary osteoarthritis (OA) (hereinafter, hip dysplasia) due to developmental dysplasia of the hip (DDH) is a relatively challenging procedure, 1 –3 mainly due to the consequent deformity of the proximal femur. 4 –7 Specifically, cementless femoral reconstruction is significantly affected by the shape of the femur, and so either the stem does not fit the shape of the femoral canal or the stem neck often displays an abnormal rotational alignment in cases of hip dysplasia. Strategies to address these deformities of the proximal femur in hip dysplasia include the use of a modular stem available for rotational deformity 8 –12 and the use of distal fixation stems, 13,14 with which relatively good outcomes have been reported. The authors have reported on favorable outcomes of cementless femoral reconstruction in hip dysplasia using the S-ROM stem modified for Asians 10 and the AML stem 13 (both DePuy Synthes, Warsaw, Indiana, USA). However, these systems have the characteristic disadvantages of stress shielding due to distal fixation and metal-related complications seen in modular prosthesis; thus, studies on stems with less risks are necessary.
The Taperloc stem (Zimmer Biomet, Warsaw, Indiana, USA) has a long history among titanium alloy flat tapered wedge design cementless stems, and since its launch in 1983, there have been several reports on favorable long-term outcomes. 15 –19 The Taperloc Complete system developed in 2011 has a reduced distal design with a gradual reduction in stem width distal to the level of the porous coating. And in 2012, the Taperloc Complete Microplasty stem (TCM stem; Figure 1) with the distal stem length shortened by 35 mm became available for use. The stem is extremely low volume with a flat design, small anterior–posterior (AP) diameter, and further reduced stem length. These features, which on the one hand raise concerns about adequate initial mechanical fixation, may on the other hand be advantageous in offering more flexibility for positioning within the canal. Little time has passed since the launch of the TCM stem, so reports on clinical outcomes are few. 20 Furthermore, to our knowledge there are no reports on the use of this stem in cementless femoral fixation for hip dysplasia.

TCM stem: (a) anterior view and (b) lateral view. The entire stem is extremely low volume due to its flat shape with the small AP diameter; the distal stem further shortened 35 mm less than standard length. TCM: Taperloc Complete Microplasty; AP: anterior–posterior.
The authors have actively used the TCM system for primary THA since January 2012. Utilizing its characteristic of high flexibility in positioning due to its low volume, we performed a somewhat deliberate alignment control for varus, valgus, and rotation in terms of stem positioning. The aim of this study was to investigate the postoperative outcomes in primary THA performed in hip dysplasia patients using the TCM system and to elucidate clinical functional outcomes and radiographic X-ray outcomes. Specifically, we elucidate the quality of fixation on the deformed femur, complications such as fracture and dislocation, and discuss the advantages and limitations of flat tapered wedge short stems in hip dysplasia.
Materials and methods
From January 2012 to November 2016, 434 patients (461 hips) underwent primary THA via the posterior approach in our department. We reviewed the medical history and preoperative bilateral hip AP X-rays, and 311 hips were diagnosed as having secondary OA (hip dysplasia) due to DDH. In total, 46 patients had been treated for DDH in childhood, and for those with no history of treatment, OA due to DDH was diagnosed when a clear trend in superolateral subluxation of the femoral head was noted on the preoperative X-ray. Post-traumatic OA, primary OA, OA due to femoroacetabular impingement, and OA of the elderly related to pelvic retroversion due to lumbar deformity or osteoporosis (including subchondral insufficiency fracture or rapidly destructive coxarthrosis) were excluded. Stems used for femoral reconstruction for these 311 hips were the TCM stem for 264 hips, standard length Taperloc Complete stem for 7 hips, other cementless stem for 36 hips, and cemented stems for 4 hips. Of the cases where the TCM stem was used, two patients died postoperatively from causes unrelated to the surgery, and five patients could not be examined due to reasons such as worsening of overall health and difficulty with office visits due to traveling distance. For these seven patients (seven hips), we were able to confirm via phone interviews that they had not undergone a revision arthroplasty of the existing stem. Thus, the patients in this study were the 235 patients (257 hips) for whom primary THA was performed for hip dysplasia using the TCM stem, and a direct physical examination along with plain X-rays was possible at 2 or more years after surgery. There were 201 female patients (221 hips) and 34 male patients (36 hips), and age at the time of surgery was 41–86 (mean 63) years. Postoperative follow-up period ranged from 2 years to 6 years and 11 months (mean 4 years and 5 months).
All surgeries were performed via the posterior approach. The authors’ perspectives and techniques regarding TCM stem positioning are as follows: The initial mechanical fixation of the stem is mainly achieved at the tapered portion in the distal half of the porous area. At this portion, secure direct contact between both the lateral and medial cortices and the stem is achieved. From the standpoint of preventing fractures, it is important to avoid direct contact between the cortex and the stem in the calcar region in the medial proximal end of the femur, thus leaving a slight amount of cancellous bone in that region (Figure 2). We attempt to initially achieve neutral alignment by approaching the estimated size using a broach for standard length stems. With the last 1–2 sizes, broaching is performed for the Microplasty stem. Because there is higher flexibility in positioning a shorter broach, the abovementioned avoidance of direct contact at the uppermost medial region is achieved by lateralization of the broach or, when necessary, by adding slight valgus. When a larger femoral head offset is required, broaching is performed with somewhat of a varus, but in this situation too, we attempt to avoid tight direct contact with the calcar region. We measure the anatomical anteversion of the femoral neck using a goniometer intraoperatively (relative to the axis of the lower leg with the knee joint at 90° flexion), and if anteversion is large, positioning is performed with decreased anteversion up to 10°, and when anteversion is low, increasing version up to 20°. We observe the basic principle of the initial step 1 (above) even when rotational control of the stem is performed.

Initial/mechanical fixation of the stem is achieved at the distal half of the porous area in the tapered portion. Direct contact between the cortex and the stem is securely achieved both laterally and medially in this portion (white arrow heads). From the standpoint of preventing fractures, direct contact between the cortex and the stem was avoided at the calcar region in the medial proximal femur, and a small amount of cancellous bone remains (white arrows).
Cementless fixation was performed for the acetabular side in all cases, and the implants used were the Ringloc cup (51%), Regenerex cup (22%), and the G7 cup (27%) (all Zimmer Biomet); in all cases, a vitamin E-infused highly cross-linked polyethylene liner was used.
Either a CoCr or delta ceramic head with diameters 28 mm (9%), 32 mm (78%), or 36 mm (13%) was used.
For postoperative therapy, patients were out of bed the day after surgery and then practiced ambulation as tolerated without weight-bearing restrictions. Almost all patients achieved ambulation using a T-top cane within 1 week after surgery. We evaluated the following in these patients:
Implant size and neck variation
Stem sizes were 4–20, with a choice of three possible neck types of standard offset neck, high offset neck, and XR 123° neck (Figure 3). We investigated the frequency of use of each type.
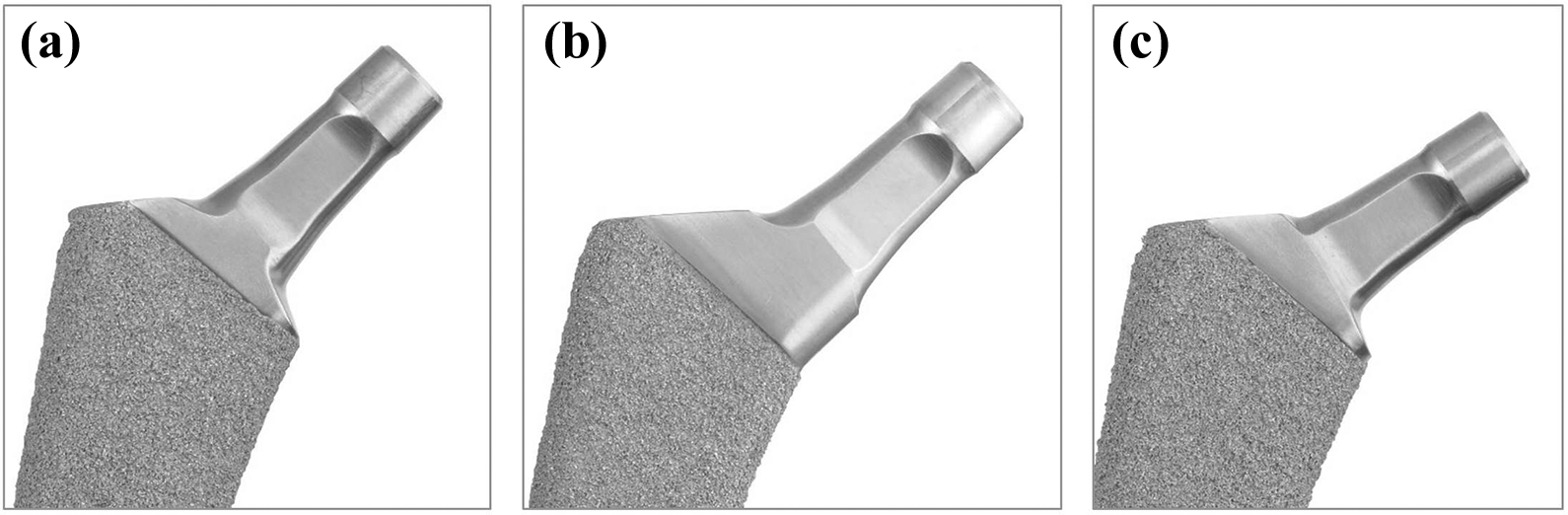
TCM stem neck variation: (a) standard neck, (b) high offset neck, and (c) XR 123° neck. TCM: Taperloc Complete Microplasty.
Clinical outcomes
Functional outcomes of the hip joint were evaluated using the Japanese Orthopaedic Association scoring system (JOA score). This system evaluates hip joint function with a maximum of 100 points, comprising 40 points for pain, 20 points for range of motion (ROM), 20 points for ambulatory ability, and 20 points for activities of daily living (ADL). 21 Evaluated complications were deep infection, dislocation, intraoperative and postoperative periprosthetic fracture, symptomatic venous thromboembolism, and presence of neuroparalysis. The presence of revision arthroplasty for the affected hip was also evaluated.
X-ray analysis
By comparing the immediate postoperative plain X-ray with the X-ray taken at the end of the follow-up period, we evaluated the status of stem insertion, stem subsidence, changes in alignment, and adequacy of biological fixation. Also, for evidence of femoral remodeling, we examined the degree of stress shielding, spot welds, areas of cortical hypertrophy, and rate of occurrence.
The status of stem insertion was evaluated in patients noted to have greater than or equal to 3° of stem axis deviation from the femoral axis by the degree of varus and valgus on AP view and by the degree of flexion and extension on lateral view. Stem subsidence was defined as migration greater than or equal to 2 mm, and change in alignment was defined as any change greater than or equal to 3°. For stress shielding, evaluation was based on methods described by Engh et al., 22,23 and stem length was divided into four equal parts on AP view of the femur; then the region with decreased density was evaluated and scored on a scale of 0–4. Cortical hypertrophy was defined as the presence of an over 2-mm increase in cortical thickness compared to preoperative images. Biological fixation of the stem was determined using methods described by Engh et al. 22,23 using plain AP X-rays.
Evaluation of stem anteversion adjustment
Evaluation of stem anteversion adjustment was performed in a fraction of patients for whom both pre- and postoperative computed tomography (CT) scans were available. Preoperative CT scans including full-length femur scans were performed for operative planning in all patients, but were not performed postoperatively. Therefore, we investigated the 44 hips where CT scans including the full-length femur were performed for evaluation of venous thromboembolism risk, implant positional alignment, and periprosthetic fracture. Measurement was performed on axial images 15 mm proximal to the center of the lesser trochanter, with the posterior condylar line as the reference on axial view of the femoral condyles. Anatomical femoral neck anteversion was measured preoperatively, and stem anteversion was measured postoperatively (Figure 4).
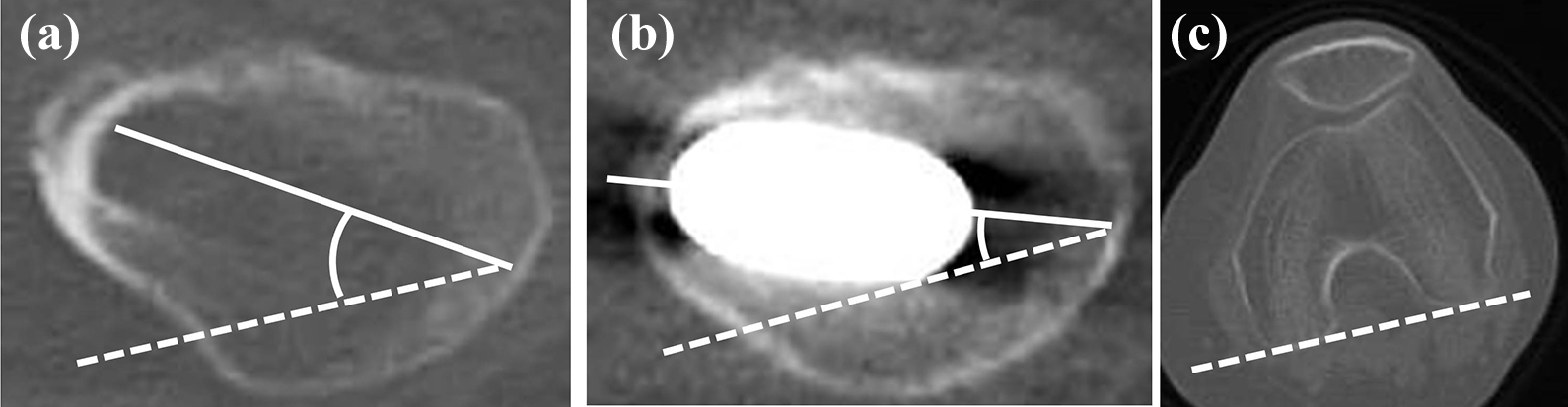
Preoperative anatomical femoral neck anteversion and postoperative stem anteversion. Using an axial cut image 15 mm proximal to the lesser trochanter, with the posterior condylar line on an axial cut with the femoral condyles as reference (c), anatomical anteversion was measured preoperatively (a), and stem anteversion was measured postoperatively (b).
The current study was approved by our institutional review board and was also implemented in observance of the ethical consideration based on the Helsinki Declaration.
Results
Implant size and neck variation
The sizes and frequency of use of each stem are shown in Figure 5. The stem with the most frequent use was the size 11 stem, which was used in 17% of all patients, and the mean ± SD of the stem size was 11.5 ± 1.6.

Frequency of use of stem sizes. Most frequently used was size 11 in 17% of all cases. The mean ± SD of stem sizes was 11.5 ± 1.6; the four sizes with the most frequent use were sizes 9–12, accounting for 54% of all cases.
The four sizes with the most frequent use (sizes 9–12) included 54% of all patients.
Frequency of neck variation was 39% for standard offset, 48% for high offset, and 13% for XR 123°.
Clinical outcomes
The JOA score (pain/ROM/ambulation/ADL), which reflects hip function, improved from mean 13/11/12/13 preoperatively with a total of 49 points to 39/16/18/16 with a total of 89 points, at the end of the study.
Regarding complications, a transverse fracture of the greater trochanter in one hip, which was not noted intraoperatively or on immediate postoperative X-ray, was seen after ambulation on X-ray and was treated by additional open reduction and internal fixation. There was no case of split fracture at the calcar. An acute infection developed in one hip (0.4%) and was treated early with irrigation and debridement without recurrence. Postoperative dislocation occurred in one hip (0.4%), but early repair of posterior tissues with adjustment of cup alignment was performed, and there was no recurrence. No symptomatic venous thromboembolism or neuroparalysis was noted in any of the patients (Table 1). No patients required revision arthroplasty during the follow-up period, and while this is a short period of 4.4 years, stem survival was 100%.
Clinical complications.

X-ray analysis
For status of stem insertion, 246 hips (96%) had neutral insertion, 0 hips (0%) were in varus, and 11 hips (4%) were in valgus on AP view. Also, 204 hips (79%) had neutral insertion, 54 hips (21%) were in flexion, and 1 hip (0.4%) was inserted in extension on lateral view (Table 2). Postoperatively, none were noted to have stem subsidence, alignment change, or loosening, and according to X-ray evaluation for fixation as described by Engh et al., 257 hips (100%) were determined to have bone ingrown fixation. For stress shielding, some degree of atrophic change was noted in all patients in the femur around the stem, and 177 hips (69%) were grade 1 and 80 hips (31%) were grade 2, according to the classification by Engh et al. There were no hips that were grade 3 or grade 4. Spot welds were noted on AP view in 30 hips (12%) in zones 2 and 6, and on lateral view 228 hips (89%) in zones 9 and 13. Cortical hypertrophy was observed in 24 hips (11%) in zones 3 and 5 (Table 2).
Results of radiographic evaluations

Evaluation of stem anteversion adjustment
Preoperative anatomical anteversion of the femoral neck was 13–58° (mean 34°), and postoperative stem anteversion was 17–46° (mean 31°); variability was significantly reduced for postoperative anteversion (p = 0.0023, F-test). In 12 cases (27%), the stem was positioned with anteversion that was within ±5° of the anatomical anteversion, and the remaining 73% had either decreased or increased version above 5°. In total, 15 cases (34%) had 5–16° of decreased version performed, and 17 cases (39%) had 5–12° of increased version performed (Figure 6).

Anatomical anteversion of the femoral neck preoperatively and postoperative stem anteversion. Anatomical anteversion of the femoral neck preoperatively was 13–58°; postoperative stem anteversion was 17–46°, with significantly reduced variability in postoperative anteversion (p = 0.0023).
Discussion
There are numerous reports of high rates of secondary OA due to DDH in primary THA in the Asian population, specifically in the Japanese population, in addition to reports of patients with hip dysplasia comprising 78–92.6% cases of primary THA. 11,12,24 Furthermore, in 15 institutions from five regions in Japan, a report on 485 cases of new ambulatory patients stated that 81% of OA in Japanese patients is due to DDH. 25 From this background, the need for a cementless system that can be used appropriately in Asian patients with hip dysplasia and small frames is considered to be high. For the 257 dysplastic hips in an Asian population in this study, postoperative evaluation at 2 years or more (mean 4 years and 5 months) revealed clinically favorable functional outcomes with primary THA performed using a flat tapered wedge short stem. Biological fixation of the stems was also achieved with favorable radiological outcomes in all patients. Regarding complications, there were no cases of split fracture of the calcar at the time of stem insertion, with a low rate of dislocation at 0.4% (1 case).
Stem size and neck variation
The stem sizes used in the 275 hips with dysplasia in this Asian population centered around sizes 9–12. The smallest size available was size 4, and no problems with size variations were noted. Choice of neck type may be affected by planning for reconstruction, but resulted in 39% for standard neck, 48% for high offset, and 13% for XR 123° neck. The high frequency of high offset necks could likely be to improve bone coverage of the cup in cases of acetabular dysplasia, as in some cases the cup had to be positioned somewhat medially. Although the femoral head is often subluxated a bit laterally in hip dysplasia, the global offset of the femur is planned so as not to decrease greatly from the standpoint of preventing dislocation.
Initial/mechanical fixation of the flat tapered wedge short stem
The main concern regarding flat and short stems with low volume may be whether adequate initial/mechanical fixation can be achieved. Specifically, in hip dysplasia which results in deformity of the proximal femur, there are concerns of inadequate stem fit. However, the current clinical outcomes show that there was no obvious subsidence, no alignment changes were noted in the postoperative stem, and bone ingrown fixation was achieved in all cases. This could be attributed to the fact that the flat tapered wedge stem originally depended mostly on tapered fixation in the distal half of the porous area and does not pursue an overall fit in the canal. And in our current study, achieving secure tapered fixation in this region while maximally preventing the occurrence of intraoperative calcar split fracture might have led to successful fixation in 100% of the cases. Schilcher et al. performed a prospective comparison trial of the Taperloc standard stem and the Taperloc Microplasty stem and reported no difference in Harris Hip Score and survival in both groups. 26 In addition, Schilcher et al. reported that no statistically significant difference was observed in stem migration and fixation in the standard stem and the Microplasty stem according to radiostereometric analysis on measurements up to 2 years postoperatively. 27 As such, even with the Microplasty stem with a reduced stem length of 35 mm, with appropriate application, initial/mechanical fixation equivalent to standard length stem can be anticipated.
AP and rotational stem alignments in the medullary canal
A low-volume flat short stem can assume a variety of alignments within the canal. While this can pose some risk of unfavorable outcomes such as stem malalignment, there is potential of being advantageous for the surgeon by allowing more flexibility in positioning. In our evaluation of stem alignment using AP and lateral X-rays, valgus was seen in 4% on AP view, flexion was seen in 21% on lateral view, and extension was seen in 0.4%. There was no malalignment that could lead to fracture or loosening. As noted in the surgical technique section, from the standpoint of preventing fracture, we meticulously ensured avoiding direct contact between the stem and the calcar region in the medial proximal end of the femur. In other words, while broaching, if the stem approaches the calcar region, broaching is guided with more lateralization or in a slightly valgus direction; the short stem had high flexibility and ease of control for performing these maneuvers. Thus, these characteristics of the stem and surgical techniques may have contributed to achieving primary fixation and prevention of split fracture of the calcar region.
In contrast, rotational alignment of the stem is a crucial problem that relates to neck anteversion. Because Fit and Fill stems, with high filling of the metaphyseal canal, are positioned by lining and assuming the shape of the canal, adjusting the rotational alignment is fundamentally difficult. In other types of cementless stems, changing the rotational alignment from the anatomic configuration could possibly compromise fixation and therefore has not been actively performed. In the current study, rotational control was actively performed with about 10° for decreased version and 20° for increased version as the standard, and in postoperative CT evaluation, decreased version of 5–16° and increased version of 5–12° were noted. Postoperatively, the number of patients with extremely small or large neck anteversion decreased, and variability was significantly reduced compared with before surgery; this may be considered to contribute to the low incidence of postoperative dislocation (0.4%). In those cases where anteversion adjustment was performed, there were no cases where problems arose in postoperative stem fixation. We hypothesize that this is because the tapered fixation achieved at the distal half of the porous area can probably be equally achieved even when positioned with some rotation. From our findings, there is a high possibility of performing adjustment of rotational alignment in the tapered wedge short stem, but the safety of this procedure needs to be further evaluated with more patients. Also, adequate attention is necessary, particularly because of the potential increased risk of split fracture in the calcar when the stem is in direct contact with the cortex, in the posterior aspect of the calcar region with decreased version, and in the anterior aspect of the calcar with increased version.
A limitation to this study is its retrospective case-series design, which did not include a comparator group. Therefore, the results may be strongly affected by variations in the patients and in the treatment procedures performed. All patients were cases of hip dysplasia in an Asian population, and the treatment was primary THA performed via the posterior approach using a flat tapered wedge short stem. The interpretation of stem concepts and the standardization of the type of technique for positioning based on the concept interpretation are thus vital issues, and we attempted to elucidate these points in detail here.
Conclusions
The postoperative functional outcomes of primary THA performed in 257 hips in patients with hip dysplasia in an Asian population using flat tapered wedge short stems were favorable with bone ingrown fixation achieved in 100% of the cases. This flat short low-volume stem has high flexibility in positioning and, for the surgeon, offers the possibility of easy control of the stem position to avoid fracture while achieving secure fixation. This may possibly allow for some control in the rotational alignment of the stem, and so further studies are necessary to clarify methods for safely performing this procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Takuya Otani receives royalties from Zimmer Biomet Company.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.