
Abstract
Objectives:
We aimed to compare functional outcomes of two common hip approaches for patients with severe hip dysplasia in total hip replacement (THR) surgery.
Materials and methods:
Seventy hips of 68 patients randomized into two groups with regard to hip approach as posterior (group I) and anterolateral (group II). All patients underwent THR surgery with femoral shortening osteotomy. The groups were compared for operation time, preoperative and 6 months after abductor muscle strengths (AMSs), gait disorders, union time of the osteotomied site and dislocation rates.
Results:
There were two early dislocations in group I, and two early and one late dislocations in group II. No significant difference was observed regarding hip dislocations. Mean union time of the osteotomied site was 113.9 ± 51 days in group I while 111.1 ± 29.3 days in group II (p = 0.774). Six months after surgery, group I had higher AMS than group II (p < 0.0001). More patients in group II had Trendelenburg gait pattern (p = 0.043), while no difference was observed regarding antalgic and deviated gait patterns between groups.
Conclusion:
THR surgery for patients with severe developmental dysplasia of hip is a challenging procedure, and posterior approach provides better functional outcomes regarding gait and AMSs.
Introduction
Total hip replacement (THR) is a challanging surgery for patients with Crowe type 4 developmental dysplasia of hip (DDH). Higher complications as dislocation, neurovascular injury, periprosthetic fractures, infection and permanent limping were reported before in comparison to primary THR surgery. 1 Dealing with these complications is also harder for patients with DDH. It is crucial to reduce the risk of complications for these patients and surgical approach may be a target to reduce complications. 2 Anterolateral (Watson-Jones) and posterior (modified Gibson) approaches are the most used ones for THR for patients with DDH in recent literature. 3,4
There are many reports comparing anterolateral and posterior approaches regarding advantages, disadvantages and the prevalence of choice in their own society for primary THR. 5 –8 Dislocation of the replaced joint for posterior approach is reported to be around 1–5% in primary THR surgery. 6,9,10 In anterolateral approach, the risk of dislocation is reduced by approximately 0.4–0.5%. 11 Insufficiency of the abductor muscles resulting in gait disorders is reported to be a common problem after anterolateral approach of the hip. 12 –14 When neurologic injuries are compared, superior gluteal nerve (2.2–42.5%) and femoral nerve (0.1–2.4%) injuries were reported for anterolateral incision, while sciatic nerve injury (1.3%) is reported for posterior incision. 6,15 –19 In United Kingdom, posterior incision is preferred by 61% of surgeons while anterolateral incision is preferred by only 33%. In Canada, anterolateral incision is preferred by about 60% and 53% in Norway. 20 –22
Although many reports compared hip approaches for primary THR, there is no report in the literature regarding hip approaches for THR surgery in patients with severe DDH. In this study, we aimed to compare the outcomes of anterolateral and posterior approaches for patients with severe DDH.
Materials and methods
Seventy-seven hips of 75 consecutive patients who were operated between August 2012 and December 2015 were included in this study. All patients underwent THR surgery due to the Crowe type 4 DDH. After the consent of the local ethical committee (05.06.2014/3234) patients were randomized into two groups with regard to the admittance order to the orthopaedic outpatient clinic. All patients were given a number, respectively, starting with 1, and surgical procedures were applied one by one by the following number: 1st: AL approach; 2nd: PL approach; 3rd: AL approach; 4th: PL approach; and so on. Seven patients lost to follow up and were excluded from the study. Finally, 35 hips of 34 patients were operated via modified Gibson (posterior) approach, and these patients were qualified as group I, and group II included 35 hips of 34 patients that were operated with a Watson-Jones approach (anterolateral).
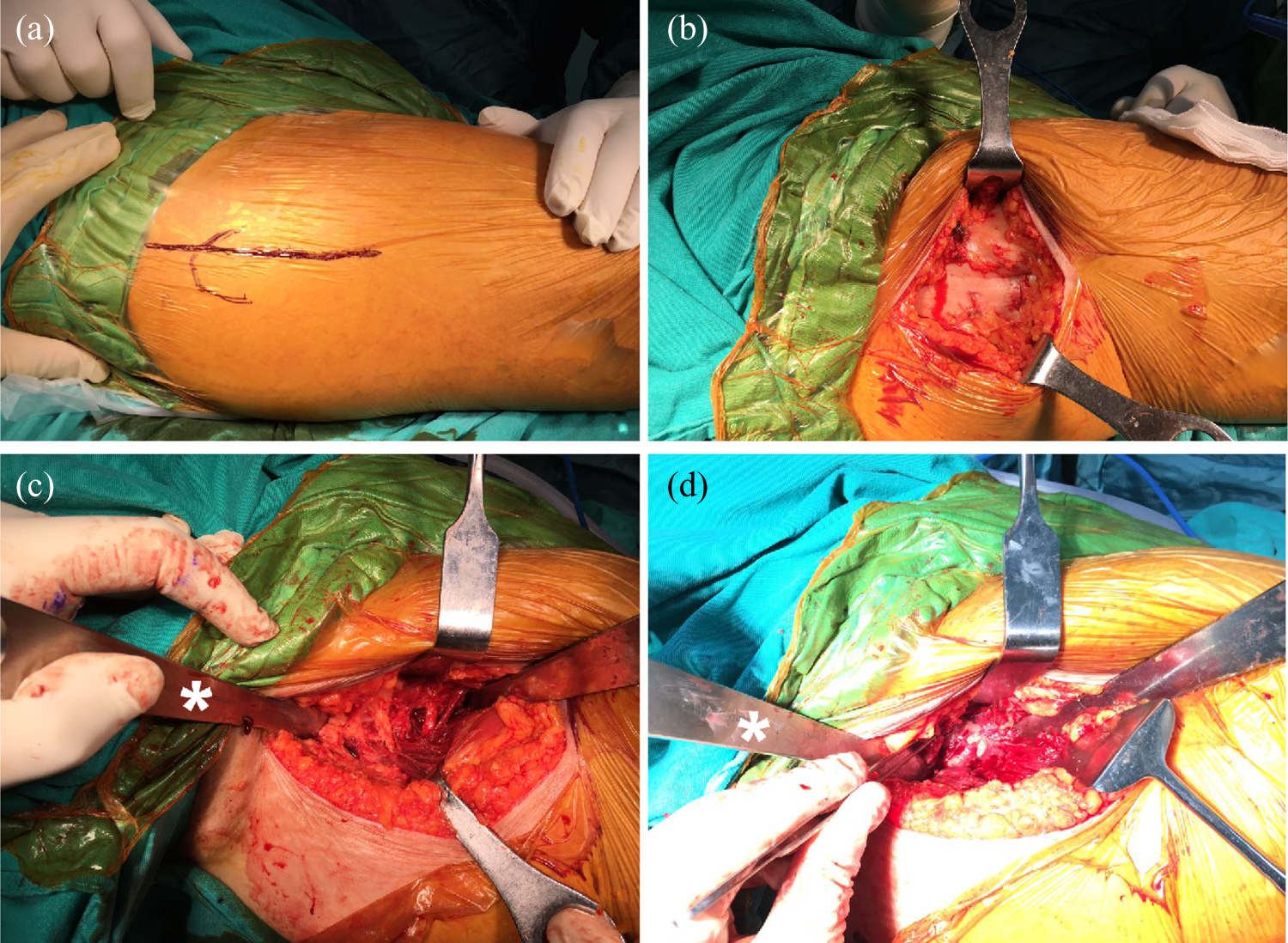
All the surgical procedures were done under general anaesthesia. In group I, the posterior approach was familiar with modification of the Gibson–Moore approach. After a posterior curve skin incision (Figure 1), external rotator muscles and tendons were revealed and hanged with a suture (Figure 2). Elongated joint capsule was exposed and femoral head was revealed with external rotation of the femur. In group II, after an anterolateral incision, the space between tensor fascia and gluteus medius muscles was used to reach joint capsule and femoral head. Femoral head was removed and femur was reamed in each group. Femur was rasped with proper size. A transverse osteotomy 1–2 cm distal to the minor trochanter was applied and proximal part of the femur was retracted, by following the prolonged joint capsule the real acetabulum was identified. Hydroxyapatite (HA)-coated cementless acetabular cup placed with 10–20° of anteversion and 35–45° of inclination after reaming the real acetabulum. Amount of shortening was determined by moving the proximal part of the femur distally and overlapping part of distal femur was osteotomied. The osteotomied part was used as a strut bone graft by splitting into two parts and fixing over the osteotomied site with cables. Distal split and proximal HA-coated femoral stem (Secur-Fit; Stryker Orthopaedics, Mahwah, New Jersey, USA) were used for all patients.

Posterior modified Gibson approach. (a) Skin incision. (b) Superficial dissection. (c) Approach to the femoral medullary canal (white arrows show the gluteal muscles during reaming the medullary canal). (d) Elongated joint capsule is used to determine real acetabulum.
Anterolateral Watson-Jones approach. (a)Skin incision. (b) Superficial dissection. (c) Dissection between gluteus medius and tensor fascia. (d) Revealing the joint capsule. * Shows the retraction of the gluteal muscles during the surgery.
Based on their toleration level, all patients were allowed weight bearing the day after surgery with two crutches . Patients were discharged after tolerating mobilization within few days of surgery. Patients were followed up on 15th day, 1 month and 6 months after surgery. Anteroposterior and lateral X-rays were obtained for all patients on last follow-up. Union of the osteotomied site was evaluated as identified by Whalen et al. 23 Patients who has lack of union after 6 months of surgery were categorized as non-union of the osteotomied site. 24 Patients with non-union were re-operated and the osteotomied site was grafted.
Operation time was obtained from the anaesthesia records of the patients. Harris hip scores, abductor muscle strengths (AMSs) and gait patterns were evaluated before the surgery and on the last follow-up 6 months after surgery. AMSs were evaluated by asking the patient to elevate his/her lower limb while lying on lateral position on the examination couch using ‘Medical Research Council grading of power scale’ and graded 0–5 points. Any other surgery-related complications like neurological injuries and heterotrophic ossification were recorded. Walking patterns of the patients were examined by a physical therapist who doesn’t know the surgical procedure of the patient. Trendelenburg gait, antalgic gait and deviation of walking were evaluated and recorded.
The groups were compared for early-late dislocation rates, non-unions, Harris hip scores, AMSs and gait patterns. All patients were evaluated for their preoperative and follow-up muscle strengths. Statistical analysis was assessed with MedCalc version 10.1.6. Groups were compared with Student’s t test and categorical variables were compared with χ2. Any p value less than 0.05 was considered as significant.
Results
This study consisted of 70 hips of 68 patients that were operated for Crowe type 4 hip dysplasia with THR surgery and femoral shortening osteotomy. Sixty-one (89.7%) of 68 patients were female, while 7 (10.3%) of them were male. Mean age at the time of surgery was 51.1 ± 9.4 years (26–69). Left hip was operated in 29, right hip in 37 and bilateral hips were operated in 2 patients. Thirty-four of 68 patients constituted group I and were operated with a posterior modified Gibson hip approach and the remaining 34 were operated with anterolateral Watson-Jones approach and these patients constituted group II.
Early dislocation of the hip occurred in two of 34 patients in group I. One of these patients was re-operated due to the excessive anteversion of the acetabular component and the other was treated with closed reduction under general anaesthesia. No late dislocation was observed in this group during follow-up. In group II, there were two early hip dislocations and one patient had hip dislocation 3 months after surgery. Early dislocated hips were treated with closed reduction under general anaesthesia and the patient with late hip dislocation had rotation of the osteotomied site and underwent a revision surgery. No re-dislocation observed in any patients that were treated for dislocation.
Mean union time was 113.9 ± 51 days (45–180) in group I, while 111.1 ± 29.3 days (60–180) in group II. No significant difference was observed between groups regarding the union time of the osteotomied site (p = 0.774). One patient required bone grafting surgery due to the non-union of the osteotomied site in group I. No non-unions were observed in group II.
AMS of all patients was significantly higher at the last follow-up. AMSs of all patients were 1.26 ± 0.4 days (1–2) and 2.47 ± 0.9 days (1–4) preoperatively and at final follow-up, respectively. Group I means AMS at the final follow-up was 3 while group II mean AMS was 1.8 and group I had significantly higher mean AMS at the final follow-up (p < 0.0001). Mean operation time was 98.1 ± 13.1 min for group I, while 94.4 ± 15.1 min for group II (p = 0.603). No significant difference was observed between groups regarding Harris hip scores, hip dislocation rates, deviated and antalgic gait patterns by the final follow-up, but group II had more patients with a Trendelenburg gait (p = 0.043; Table 1).
Clinical findings of patients between the groups.

SD: standard deviation; Preop.: preoperative; Postop.: postoperative.
Discussion
THR surgery for dysplastic hips is a challenging surgery, with higher complications and technically demanding procedure compared to primary THR. 25 –27 Thus, all the potential factors and technical tricks should be considered for these patients. Most important finding of this study was that the surgical approach used in THR for patients with severe dysplasia affects the AMS. The study demonstrated that posterior approach ensures better clinical outcomes and better AMS when compared to anterolateral approach for patients with severe hip dysplasia.
The anterolateral Watson-Jones approach is reported to be associated with AMS loss in many reports before. 12 –14 While performing a THR via anterolateral approach, hip abductor muscles need to be retracted to reach the medullary canal of the femur and sometimes anterior fibres of the gluteus medius muscles are needed to detach from the greater trochanter. However, the medullary canal is usually approachable behind the abductor muscles and tendons without any injury to these structures in posterior approach. The AMS is also crucial for the stability of the THR beside proper gait. Patients with severe hip dysplasia have shortened and weaker abductor muscles vis-à-vis normal patients and any afford should be spent to preserve these muscles to ensure the stability of the replaced hip and normal gait.
Watson-Jones and modified Gibson approaches were compared in many reports before for primary THR surgery. 28 –30 Many authors have related modified Gibson approach with increased risk of dislocation due to the weakening of the posterior soft tissues as external rotator muscles and the joint capsule. 31,32 Elongated hip capsule is totally resected in patients with severe dysplasia either in Watson-Jones or in modified Gibson approach; therefore, the advantage of preserving the joint capsule via Watson-Jones approach is diminished in patients with severe dysplasia. When the crucial role of the abductor muscles for hip stability is considered, higher dislocation rates may be expected in Watson-Jones approach for patients with severe hip dysplasia. Although we observed more dislocations in Watson-Jones group, the difference was not significant. Future studies with more patients and further follow-up periods may point this difference. These are the primary limitations of our study.
Downing et al. reported no difference regarding AMSs after primary THR surgery among two approaches. 33 A healthy patient with adequate muscle volume may tolerate the effect of the approaches on AMSs, but this study demonstrated that patients with DDH cannot tolerate any more loss of AMS. In recent literature, there is no article regarding AMSs of patients with DDH after a THR surgery. Patients with Crowe type 4 DDH are prone to have a Trendelenburg gait posture with slopping to the affected side due to the shortened abductor muscles. 34 Recovery of the gait posture is expected after THR surgery in patients with DDH. AMSs of patients were significantly better after bone union when compared to preoperative evaluation and patient’s gait was recovered. Trendelenburg gait was observed in more patients who were operated using Watson-Jones approach. We believe that the difference was due to the injured abductor muscles during the surgery.
We observed no significant difference regarding operation time between the Watson-Jones and the modified Gibson approaches. Operation time has been reported to be similar for primary THR surgery. 35 Altered anatomical structures of patients with DDH extended the time needed for a THR and similar surgical duration was observed between different approaches. The operation time was about 2 h for each approach in this study, and it was longer than the time needed for a primary THR reported in the literature previously. 35
In conclusion, THR for patients with DDH has promising outcomes, and a posterior approach instead of anterolateral approach may provide a better gait pattern with adequate AMS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.