
Abstract
Purpose:
The results of reamed bipolar hemiarthroplasty (BHA) in patients with hip osteoarthritis (OA) are reported to be unfavorable. Acetabular reaming for sufficient bony coverage caused bipolar head migration into the superomedial direction, and most patients required revision surgeries. Several methods are applicable to treat decreased bone stock. This study aimed to investigate the midterm results of revision surgeries using the cementless cup with the rim-fit technique.
Methods:
Between 1996 and 2014, acetabular revision surgeries using the cementless cup with the rim-fit technique were performed in 86 hips (74 patients). We evaluated radiographic outcomes, including positional change of the rotation center of the artificial femoral head, presence of implant loosening, and filling of the initial gap. We also evaluated clinical outcomes, including the Harris hip score (HHS), and postoperative complications.
Results:
The average positional changes from BHA to prerevision surgeries were 8.0 mm superiorly and 4.1 mm medially. The average changes from prerevision to postrevision surgeries were 3.7 mm inferiorly and 2.4 mm laterally. No implant loosening was found in all cases; the initial gap between the acetabular host bone and the acetabular cup was filled in 53 (93%) among 57 hips. The average HHS improved from 65.9 before revision surgeries to 83.8 in the latest follow-up. Dislocation and postoperative periprosthetic fracture occurred in two and five hips, respectively; no cases required rerevision surgeries.
Conclusion:
There were favorable midterm results of the revision total hip arthroplasty for migrated BHA in patients with hip OA using cementless cup with the rim-fit technique.
Introduction
The long-term results of reamed bipolar hemiarthroplasty (BHA) for patients with osteoarthritis (OA) of the hip joints are reported to be unfavorable. 1 –3 In almost all cases, the reason for unfavorable results was the superomedial migration of the bipolar head due to a sufficient centripetal position after superomedial reaming; most patients required revision total hip arthroplasty (THA). Because of the location of the migrated bipolar cup and the considerable amount of bony loss of the acetabulum, several methods have been introduced in revision THA to achieve acetabular reconstruction, including bulk structural allograft augmentation, 4 use of the bilobed and customized prosthesis, 5,6 high hip center implantation, 7,8 or cementless cup implantation using the rim-fit technique. 9,10 These methods have several merits and demerits; however, there is a paucity of published data focusing on the results of the cementless cup implantation using the rim-fit technique to the acetabulum of large bony defect.
Applications of the cementless cup to the acetabulum with large bony defect often pose several concerns, including the initial stability of the acetabular component, the location of the femoral head center, the initial gap occurred between the acetabular host bone and the acetabular component, clinical outcomes, and other postoperative complications. The aims of the present study were to investigate the midterm results of the acetabular revision THA using cementless cup with the rim-fit technique, 9 including the stability of the acetabular component, the extent of the positional change of the artificial femoral head center pre- and postoperatively, the existence or nonexistence of initial bony gap filling, other postoperative complications, and clinical results.
Materials and methods
Patients
Between January 1996 and December 2014, 74 patients (71 females, 3 males; 86 hips) underwent revision THA using cementless cup with the rim-fit technique at our department. The institutional review board of the University of Tokyo Hospital provided ethical approval (number 2674-(3)), and informed consent was obtained from all participants before the study commenced. The preBHA diagnoses were OA of the hip joint secondary due to acetabular dysplasia in all patients. The mean age at revision THA, period between BHA and revision THA, and duration of postoperative follow-up were 66.3 (range 49–80), 12.0 (range 3–22), and 10.4 (range 1–20) years, respectively.
The indications for revision THA were as follows: (1) hip pain with prosthesis migration and (2) no hip pain with progressive prosthesis migration. In cases of no hip pain with prosthesis migration, we considered the extent of the migration, not to progress to the type Ⅳ of the American Academy of Orthopedic Surgeons (AAOS) classification, 11 because other complicated methods had to be employed in such cases. Therefore, we recommended revision THA to patients before the acetabular bony defect progressed to type Ⅳ of the AAOS classification.
Surgical principles
All patients underwent primary BHA with acetabular reaming and revision THA to rectify superomedial migration of the bipolar head (Figure 1(a) and (b)). In all patients, there was no evidence of stem loosening (Bi-metric®, Biomet Inc., Warsaw, Indiana, USA); therefore, stem removal was not performed during revision THA. After dislocation of the bipolar head, the bipolar and inner heads were removed from the stem neck. Treatment of the soft tissue, including joint capsule and labrum, could explore the entire periphery of the acetabulum. Acetabular reaming was initiated from a size of 4 mm smaller than the removed bipolar head, and final reaming was performed with a size of 2 or 4 mm larger than the removed bipolar head. After the acetabular component trial was placed and the stability between the acetabular host bone and the component trial was confirmed, the acetabular component (Mallory Head®, Biomet Inc.) was implanted. The component was a porous-coated (plasma-sprayed) titanium alloy component with four peripheral fins and three screw holes (Figure 1(c)). We used one or two screws in all cases, despite whether an initial fixation between the acetabular component and the host bone was obtained. In eight cases, because of the residual cavity between the acetabular host bone and the acetabular component, the bone chip obtained through acetabular reaming was transplanted to the cavity; however, no allograft transplantation was necessary. In all cases, ambulation and full weight bearing were allowed 1 day after the revision surgery.

Plain radiographs of the hip joint: (a) postBHA, (b) prerevision THA, and (c) postrevision THA. BHA: bipolar hemiarthroplasty; THA: total hip arthroplasty.
Radiographic evaluation
To investigate the extent of the femoral head migration from BHA to revision THA, and that of the correction of the femoral head migration, the locations of the femoral head center in postBHA, prerevision THA, and postrevision THA were measured. Additionally, the distances between postBHA and prerevision THA and those between prerevision and postrevision THA in the vertical and horizontal directions were calculated (Figure 2(a) and (b)). The horizontal reference was a line connecting the bilateral teardrop of the acetabulum, and the vertical reference was the middle point of the teardrop. To investigate the presence of implant loosening, cup inclination and anteversion were measured. The cup inclination was measured as the angle between the line connecting the bilateral teardrop of the acetabulum and the line connecting acetabular component rim. The cup anteversion was calculated using the following equation:

where S and TL were the length of the short axis and the total length of the projected cup cross-section, respectively. 12

The positional changes of the artificial femoral head were measured between postBHA and prerevision THA and between prerevision and postrevision THA in the vertical (a) and in the horizontal direction (b). BHA: bipolar hemiarthroplasty; THA: total hip arthroplasty.
Moreover, the presence of the initial gap filling between the acetabular host bone and the acetabular component (Figure 3) was evaluated.

Filling of the initial gap between the acetabular host bone and the acetabular component was observed in the plain radiographs of the hip joint: (a) postrevision THA and (b) 1 year after revision THA. THA: total hip arthroplasty.
Clinical evaluation
To enable clinical evaluation, demographic data, clinical scores, and intraoperative or postoperative complications were retrospectively reviewed using medical records. Clinical performance was evaluated before revision THA and at the time of final follow-up using the evaluation chart of hip joint function presented by the Japanese Orthopaedic Association (JOA score).
13
The JOA score consists of the following four categories: pain (40 points), range of motion (20 points), gait (20 points), and activities of daily living (20 points). The sum of the points can be used as an approximate estimate of hip function, with a total score of 100 points indicating a perfect score, which is considered normal. Fujisawa et al. reported an excellent correlation between the JOA and Harris hip scores (HHS) (coefficient of correlation = 0.843).
14
Therefore, we calculated the equivalent HHS using the following regression formula:
Statistical analysis
Statistical analyses were conducted using the paired t-test (version 2.00; Excel statistics, SSRI Co., Ltd, Tokyo, Japan). In all analyses, a p value <0.05 was considered statistically significant.
Results
Radiographic evaluation
The mean migration distances of the femoral head center between postBHA and prerevision THA were 8.0 (range 2–17) mm superiorly and 4.1 (range 1–8) mm medially. Meanwhile, the mean positional changes of the femoral head center between prerevision and postrevision THA were 3.7 (range 0–15) mm inferiorly and 2.4 (range 0–9) mm laterally (Table 1).
The mean positional changes of the artificial femoral head between postBHA and prerevision THA and between prerevision and postrevision THA.
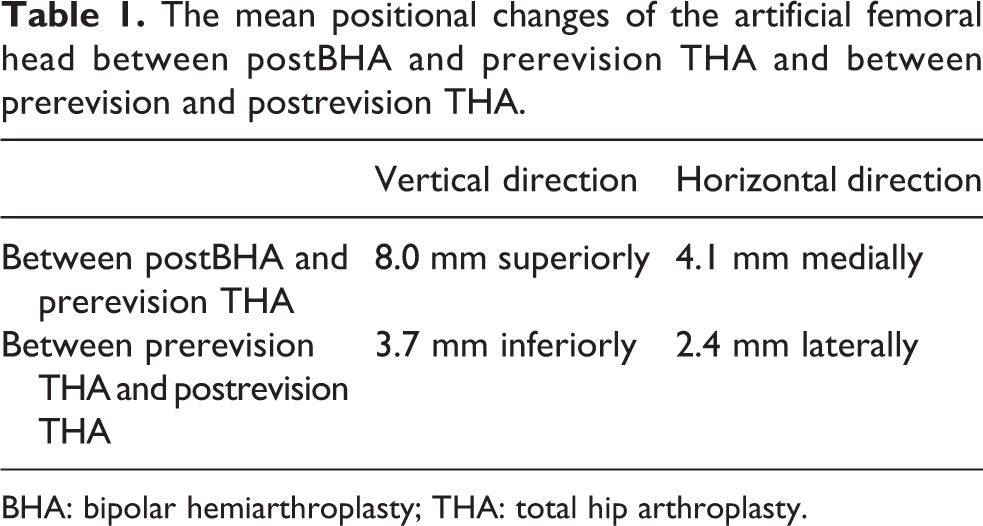
BHA: bipolar hemiarthroplasty; THA: total hip arthroplasty.
Regarding the presence of revised acetabular component loosening, there was no evidence of component migration and changes in the indexes of the component position, including cup inclination and anteversion between the postrevision THA and the time of the final follow-up; therefore, all components were judged to be stable.
An initial gap between the acetabular host bone and the acetabular component was found in 57 hips. However, 53 (93%) hips showed filling of the initial gap (Figure 3) within 12 months.
Clinical evaluation
The mean JOA score improved significantly from 62.9 at prerevision THA to 81.1 at the final follow-up (p < 0.01). In addition, the scores obtained from all four components of the JOA score at the final follow-up (pain, range of motion, gait, and activities of daily living) were better than those at prerevision THA (p < 0.01 in all components). In particular, the pain score showed high improvement (from 25.2 points at prerevision THA to 37.0 points at the final follow-up). According to Fujisawa’s regression formula, 14 the mean preoperative JOA scores and those at the final follow-up corresponded with HHSs of 65.9 ± 15.7 and 83.8 ± 13.2 points, respectively (Table 2).
Pre- and postoperative JOA and HHSs.

THA: total hip arthroplasty; JOA: Japanese Orthopedic Association; HHS; Harris hip score.
Interestingly, no intraoperative complications occurred in all cases. Meanwhile, postoperative complications occurred in seven hips. Posterior dislocations occurred in two hips, however, no cases suffered from recurrent dislocation. Postoperative periprosthetic fractures caused by fall in five hips, which were treated by open reduction and internal fixation without removal of THA components. No surgical site infections occurred, and no rerevision surgeries of acetabular component or femoral stem were required in any of the cases for any reason.
Discussion
Reasonable results have been reported in BHA in patients with femoral neck fractures 15,16 or osteonecrosis of the femoral head. 17,18 However, several studies pointed out unfavorable outcomes in BHA with acetabular reaming in patients with OA of the hip joint. 1 –3 Most failures were related to a considerable degree of bipolar cup migration into the central and/or superior direction, which caused considerable bony defect of the acetabulum at the time of acetabular revision surgery.
In cases of acetabular revision surgery against the acetabulum with an extensive bony defect, several reconstructive methods have been introduced. Usage of the reinforcement ring with bone grafting with bulk structural allograft combined with or without autograft or artificial bone was reported to obtain favorable outcomes. 4 The bilobed and customized prostheses with or without bone grafting are also reported to achieve favorable results. 5,6 In contrast, the results of cementless cup implantation by the rim-fit technique without bone grafting are also fairly favorable. 9,10 However, cementless hemispherical cup implantation without bone grafting poses concerns regarding postoperative issues, including high hip center positioning, which may lead to joint instability or unnatural biomechanical condition, poor initial stability of the acetabular component, and residual gap between the acetabular host bone and the acetabular component.
In contrast, cementless hemispherical cup fixation with the rim-fit technique provides some advantages, especially when the aforementioned issues are resolved. The advantages are as follows: First, problems related to bone grafting, especially those that are technically demanding such as a relatively higher rate of acetabular component loosening and rerevision THA, and concerns regarding long-term results without proper bone grafting 19,20 can be avoided, while proper grafting technique provides good long-term results in revision surgery 19,21 ; second, we are accustomed to the usage of the cementless monoblock components and the surgical procedures are simple. Hence, we aimed to evaluate the midterm radiographic and clinical results of the cementless cup implantation to the migrated BHA in patients with OA of the hip joint.
Regarding the position of the hip center, the present study revealed that the bipolar cup migrated superiorly and medially to a considerable extent. The average migration distances were 8.0 mm in the vertical and 4.1 mm in the horizontal direction. However, implantation of the cementless cups using the rim-fit technique shifted the femoral head center inferiorly and laterally. The average positional changes were 3.7 mm in the vertical and 2.4 mm in the horizontal direction. These results suggested that the usage of the cementless cup with the rim-fit technique was one of the procedures that could be performed to restore the migrated hip center, although the distance of the positional change may be insufficient.
Meanwhile, one of the concerns regarding the cementless cup implantation using the rim-fit technique was the stability of the acetabular component against the acetabular host bone. The present study revealed no positional change of the revised acetabular component at the final follow-up, thus, demonstrating the stability of the revised cup. Another concern was the residual bony gap between the host bone and the acetabular component. The present study showed that in 93% of the hip joints where the initial gap was observed, the gaps were filled within 12 months. Therefore, we can deduce that the residual gap has little clinical importance when the stability of the acetabular component is obtained. Additionally, in our study, the rates of intraoperative and postoperative complications were 0% and 8.3%, respectively, which were relatively low compared with the corresponding in other works of revision THA. In line, the rate of dislocation was 2.4%, which was also relatively low compared with the corresponding in other studies. 22 –24 Therefore, cementless cup implantation using the rim-fit technique seems to be a reasonable revision method in patients with migrated BHA.
The present study had several limitations. First, it was a retrospective study and not a randomized controlled trial. Second, the study did not compare the obtained results with those of other acetabular revision methods. Third, the assessment performed in 84 hip joints and the average 10.4-year postoperative follow-up period may not be sufficient to evaluate this revision method. Thus, further investigations with a larger number of cases and longer follow-up periods are necessary to confirm our findings. Fourth, the clinical outcomes were evaluated using only the JOA scores 13 and not evaluated using the patient-reported outcomes, including the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 25 the Oxford hip score, 26 SF-36, 27 and the Japanese Orthopaedic Association Hip-Disease Evaluation Questionnaire. 28 Despite these limitations, the present study provided helpful information regarding the revision THA for migrated BHA with large bony defects in patients with OA of the hip joint.
Conclusion
Midterm results of the revision THA for migrated BHA in patients with hip OA using cementless jumbo cup with the rim-fit technique were favorable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.