
Abstract
Introduction:
The use of bipolar prosthesis in the management of displaced fracture neck of femur has remained controversial. There has been a lack of long-term studies in its results and survivorship, especially in acetabular erosion.
Methods:
We retrospectively reviewed 108 single design bipolar hemiarthroplasties (105 patients) performed in a single centre between 1999 and 2008, with a mean follow-up of 7.4 years (range: 2.2–18.3 years). General indications of surgery include displaced fracture with age less than 75, narrow femoral canals not permitting the use of a monoblock implant or as salvage procedure for failed internal fixation.
Results:
Six hips (5%) required further surgery – two patients had debridement for infection and four patients required revision to total hip arthroplasty (THA) due to infection or aseptic loosening. There was no dislocation. No revision was required for acetabulum erosion. Kaplan–Meier analysis showed a 15-year survival free of revision due to any reason to be 93.1% and due to aseptic loosening to be 97.1%.
Discussion:
Our centre has shown excellent clinical results and low revision rate with the cemented bipolar system. In the context of displaced fracture neck of femur, the long-term results can be compared with THA which is associated with higher perioperative morbidity.
Introduction
Geriatric hip fracture causes significant morbidity and mortality to the elderly population. With the projected increase in the incidence of geriatric hip fractures in Hong Kong due to aging population, 1 it places an increasing burden to our healthcare system.
The best treatment for displaced fracture neck of femur is still inconclusive. 2 Management should be tailored to suit individual patient’s need. Studies have shown internal fixation to be inferior to arthroplasty for the treatment of displaced femoral neck fractures in terms of mobility, functional outcome and risk of reoperation. 3,4 Total hip arthroplasty (THA), on the other hand, is regarded as the option providing superior pain relief and functional outcome. 5 –7 However, the higher magnitude of surgery with increased operative time and blood loss 5,8 deemed THA risky for the frail elderly. There is also an increased risk of dislocation, 9 –11 and revision surgery for THA would be much more challenging. Data are also conflicting, with recent studies demonstrating similar functional outcome between THA and hemiarthroplasty. 9,11
Due to the above-mentioned reasons, hemiarthroplasty is most frequently performed for displaced femoral neck fractures in our locality. Considerable debate still exists in the choice between unipolar and bipolar designs. The design of the bipolar implant allows for interprosthetic movement between the inner and outer head. This theoretical mechanical advantage results in minimal acetabular erosion without risking dislocation, ideal for the younger and active patients. Indeed, some studies have shown a later onset of acetabular erosion 12,13 and greater hip range of movement, 14,15 in patients with bipolar implants. However, some studies have not demonstrated superior functional outcome of bipolar hemiarthroplasty compared with their unipolar counterparts. 12,16 –22
There are also downsides of the bipolar system. The cost of the bipolar prosthesis is generally higher than unipolar implants. Also, in the case of dislocation, closed reduction of the bipolar prosthesis may fail, requiring open reduction. Another potential disadvantage is that the bearing surface may generate wear particles leading to osteolysis. The purpose of this study is to review the long-term results of cemented bipolar hemiarthroplasties in our population.
Patients and methods
Our hospital performed bipolar hemiarthroplasty selectively for patients suffering from intracapsular fracture neck of femur. The general selection criteria include patients aged under 75 and with good premorbid function. The decision for a bipolar implant will also be made preoperatively or intraoperatively in patients with narrow femoral canals not permitting a monoblock implant stem. Bipolar hemiarthroplasty will also be done as a salvage procedure after failed initial internal fixation. These cases include screw protrusion, avascular necrosis, non-union or refracture.
A retrospective review from 1999 to 2008 showed a total of 120 bipolar hemiarthroplasties performed on 117 patients. Cases were retrieved from the Clinical Data Analysis and Reporting System of the Hospital Authority, Hong Kong, and their outpatient records were analysed individually. Surgeon’s experience ranged from trainees with specialist supervision (78 hips (65%)) to specialist (32 hips (35%)). Patients were positioned laterally, and the hip was approached posteriorly. Gluteus maximus was split with blunt dissection, and short rotators were divided with the hip in an internally rotated position. The joint was entered by T-capsulotomy, which was repaired in all cases. Repair of piriformis was performed selectively according to surgeon’s preference. The implant employed was the Omnifit cemented modular stem with UHR Universal head (Osteonics, Allendale, New Jersey, USA). Third generation cementation technique with distal cement plug, pulsatile lavage, vacuum mixing, retrograde filling with cement gun and proximal pressurization was used in all cases. Perioperative antibiotics were used routinely according to a standard protocol. Intravenous cefazolin was administered to all patients on induction and two further doses every 8 h after operation. For patients with penicillin allergy, intravenous vancomycin was administered. Ambulation with weight-bearing was usually initiated on the first or second day after operation, initially starting with a walking frame and then progressed to a quadripod or a stick as tolerated.
Clinical and radiographical information on all patients was collected prospectively as routine follow-up monitoring. They were carefully reviewed retrospectively for pain according to the Harris hip score for pain (out of 44), ambulatory status at 1 year and at latest follow up and any post-operative complications and reoperations. X-ray films were evaluated for the presence of any loosening or acetabular erosion. Acetabular wear was evaluated according to the criteria of Baker et al., 6 who classified acetabular erosion based on radiographic appearance: grade 0 (no erosion), grade 1 (cartilage erosion only), grade 2 (bony erosion with early migration) and grade 3 (protrusio acetabuli). Loosening of the cemented stem was evaluated according to the Harris classification 23 into no loosening, possible, probable or definite loosening. Kaplan–Meier survivorship curves were analysed on three end points: free of reoperation for any reason, free of reoperation for aseptic femoral loosening and free of revision for acetabular wear.
Results
Among these 117 patients (120 hips), 25 (21.4%) were male and 92 (78.6%) were female. Mean age of surgery was 70.5 (range: 43–94). Five patients (4.3%) died at the same admission episode as the operation, and seven patients have never attended follow-up after discharge. These 12 patients were excluded from our study.
Mean follow-up for the remaining 105 patients (108 hips) was 7.4 years (range: 2.2–18.3 years). At the time of current study, 46 patients were still alive with 38 of them still attending regular follow-up. The mean age of these 38 patients was 81.0 (range: 69–91) with a mean follow-up of 13.1 years (range: 8.2–18.3 years).
Mortality and morbidity
There was no intraoperative death. Five patients (4.3%) died at the same admission episode as the operation. Causes were due to post-operative stroke, recurrent carcinoma of epiglottis diagnosed post-operatively, myocardial infarction and two cases of pneumonia. One year mortality was 6.8% (8 patients). By the time of analysis, a further 59 patients died – 24 of pneumonia, 13 of malignancy, 4 of renal failure, 3 of acute myocardial infarction, 2 by aspiration, 2 by acute exacerbation of chronic obstructive pulmonary disease and 11 of unknown cause. Overall, none of the deaths were directly related to the index bipolar hip surgery. Mean duration of death from operation was 6.6 years. Mean age of death was 78.6.
Complication and reoperation
We report six cases (5.6%) requiring additional operation (Table 1). Among these, four cases (3.7%) were due to suspected or confirmed deep infection. Two of the four infected cases were managed with debridement alone, with good post-operative recovery. The other two cases of deep infection resulted in revision and conversion to THA. The first case was a 67-year-old lady with a history of rheumatoid arthritis. She suffered from traumatic fracture of both hips. The right hip bipolar was performed in 2004 and a left hip bipolar in 2005. The right side was infected 3 years post-operatively and was successfully treated in a two-stage exchange revision. Post-operatively she was able to walk with a quadripod, and she died of an episode of traumatic cord compression, 7 years after revision procedure. The other case was a 74-year-old healthy man, who developed hypotension and transient asystole during cementation. Immediate resuscitation was necessary, jeopardizing the sterile surgical field. He survived the operation and was put on a 6-week course of antibiotics. Unfortunately, infection was evident 1 year later. A two-stage revision was performed and he recovered without any sequelae, being able to walk unaided.
Summary of the six patients requiring additional operation.a
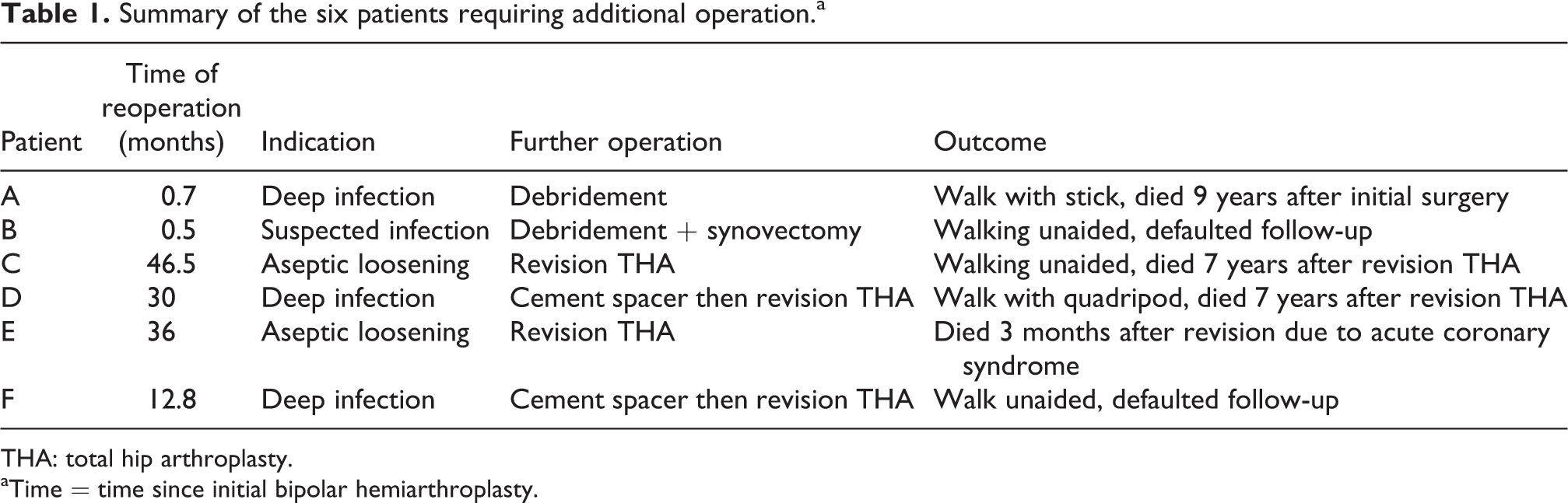
THA: total hip arthroplasty.
aTime = time since initial bipolar hemiarthroplasty.
There were two cases of aseptic loosening requiring further surgery at 3 and 4 years after initial operation. The first case was a 68-year-old man with a bipolar hemiarthroplasty in 2005. Post-operatively, varus alignment was already evident with possible poor cementation technique. Eventually, conversion to THA was performed 3 years after index operation due to pain and stem migration. He died of an acute coronary syndrome 3 months later. The other 65-year-old man presented with increasing thigh pain 4 years after the index surgery. Radiograph showed subsidence of the stem (Figure 1), and conversion to THA was performed. He recovered well and was able to walk unaided for 7 years before dying of pneumonia.

X-ray of patient with stem loosening and subsidence.
We report four cases (3.7%) of grade I acetabular erosion (Figure 2) with decreased joint space, detected at an average of 6.2 years post-operation (range: 3.5–8.2 years). None required revision surgery. There was no significant bony erosion or protrusio acetabuli detected in any of our patients.

X-ray of patient with grade I acetabular erosion.
There were two cases of post-operative deep vein thrombosis without pulmonary embolism. None of the patients had dislocation.
Survival analysis
Kaplan–Meier survivorship for the bipolar implants was analysed (Figure 3). For cases free of any form of reoperations, the survivorship (with 95% confidence intervals) was 95.8% (93.7–97.9%) at 3 years and 93.1% (90.3–95.9%) at 15 years. The survival free of revision because of aseptic loosening was 98.6% (97.2–100%) at 3 years and 97.1% (95.1–99.1%) at 15 years. None of our patients had revision due to acetabulum erosion, so the survival free of revision due to acetabulum erosion was 100% at 15 years.
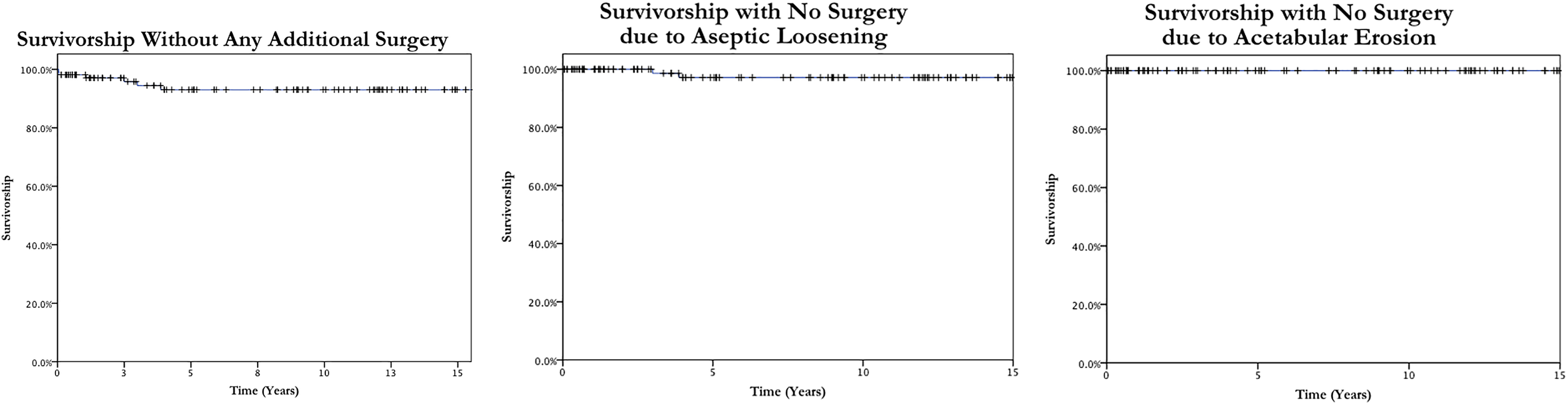
Kaplan–Meier survivorship analysis.
Clinical results
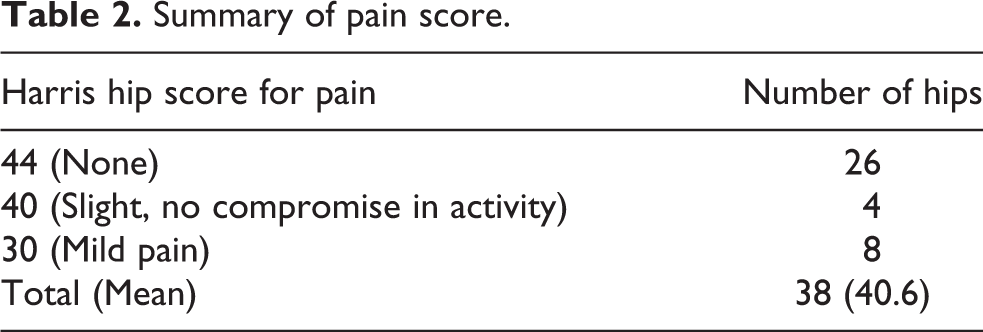
At the time of current study, 38 patients were still alive and attending follow-up. Mean age of these 38 patients was 81.0 (range: 69–91). Average follow-up duration of this group of patients was 13.1 years (range: 8.2–18.3 years). The mean Harris hip score for pain was 40.6 (Table 2).
Summary of pain score.
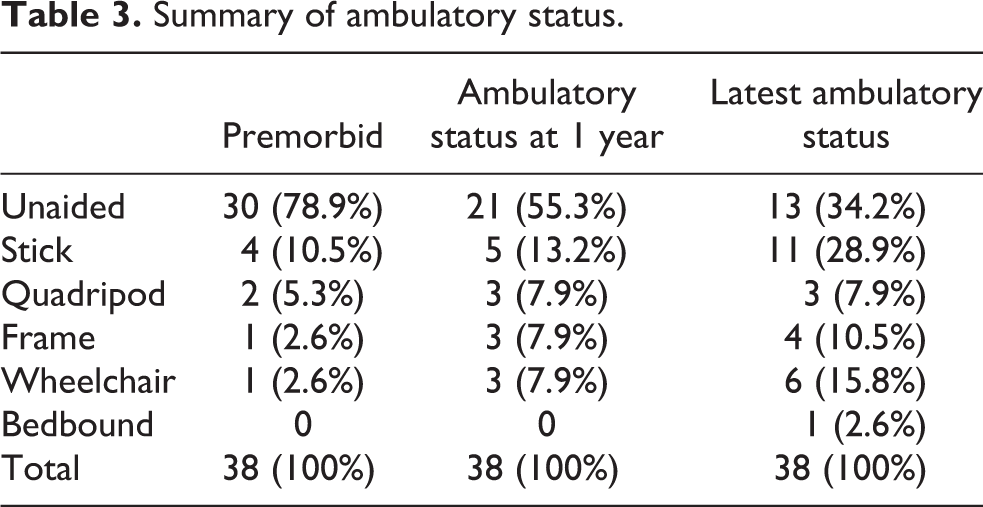
The ambulatory status of the patients before and after the operation was compared (Table 3). Over 78% of patients were able to walk unaided before sustaining a fracture hip. At 1 year after the operation, 55.3% of the patients were able to walk unaided. This excellent functional status deteriorated over time as many of our patients were already at an advanced age and suffered from other co-morbidities such as stroke, dementia, parkinsonism or another fracture. On the latest follow-up record, 34.2% were walking unaided and 28.9% were walking with a stick.
Summary of ambulatory status.
Radiographic results
Among the 38 living patients, two cases of grade I acetabulum erosion were noted with narrowing of the joint space but no bone erosion. Both cases did not complain of groin pain. All other patients had no noticeable erosion of the acetabulum. One case of definite stem loosening was detected. However, the patient was too frail and declined further operation. One case of possible loosening was detected, currently under regular radiographic review.
Discussion
There is little doubt, and the evidence is convincing, that arthroplasty surgery, instead of internal fixation, should be performed for elderly suffering from displaced intracapsular hip fractures. 3,4 The debate on the choice of implant is, however, never-ending. This decision is often influenced not only by whether one implant is more superior to another, but as surgeons, we must also take into account patient’s medical comorbidities, functional demands and premorbid ambulatory status and, inevitably, financial considerations.
Traditional monoblock unipolar hemiarthroplasty with Austin Moore or Thompson prosthesis is an economic compromise in treating fracture neck of femur. However, thigh pain with stem loosening and acetabular erosion and protrusio are known associated complications. Various authors have reported high rates of failure with these unipolar implants. Kofoed and Kofod showed a 37% failure rate with the Austin-Moore prosthesis in 2 years. 24 With the cemented Thompson implant, D’Arey and Devas reported 18.9% failure rate for 3 years of review. 25 Such high failure rate is expected to be more pronounced in active patients.
The design of the bipolar prosthesis aims to alleviate the problems associated with the unipolar counterpart. Ong et al. 17 compared 101 bipolar against 180 unipolar hips in a retrospective study and found no significant difference in functional recovery or complications. The minimum follow-up duration was 36 months with a mean follow-up time of 48 months. There was, however, no X-ray evaluation of acetabular erosion.
A randomized study by Calder et al. 16 showed no significant difference in complications or hip scores in 250 patients over 80 years old. The comparison was made between a Thompson and a Monk bipolar prosthesis. At 2 years of follow-up, there were three patients in the unipolar group showing acetabular erosion with protrusio. On the other hand, none of the patients in the bipolar group had acetabular erosion.
In a short-term randomized study by Cornell et al., 14 33 patients with bipolar hemiarthroplasties were compared against 15 modular unipolar prosthesis. Although there was no difference in hip score at 6 months of follow-up, the patients in the bipolar group had better range of movement and were able to walk faster.
Hedbeck et al. 12 investigates 120 patients who were randomized to receive a unipolar or a bipolar hemiarthroplasty. Again, no difference was noted in terms of complications rates. However, at 1-year follow-up, 20% of patients in the unipolar group already displayed acetabular erosion, compared to 5% in the bipolar group. A follow-up study by Inngul et al. 13 traces the same cohort at a 4-year review. The bipolar group results in better Health Related Quality of Life (HRQoL) beyond the first 2 years after surgery compared to unipolar group. The bipolar group also displayed a later onset of acetabular erosion compared to the unipolar group.
Meta-analyses of randomized control trials were recently made available. Jia et al. 20 confirmed a similar or better outcome in hip function, hip pain and quality of life in patients with bipolar implants, while Yang et al. 19 reported a significantly lower acetabular erosion rate in the bipolar group (1.2%) compared to the unipolar group (5.5%). Liu et al., 18 however, did not report a statistically significant difference between the two implants.
In our study, 3.7% of patients showed acetabular erosion at an average of 6.2 years. No patients require revision due to erosion. The result is comparable to other studies of the bipolar implant.
These results confirmed the expected outcome of the bipolar implant. With the surgical magnitude being similar to a unipolar hemiarthroplasty, clinical outcomes of bipolar hemiarthroplasty have been shown to be at least similar, and in some studies superior, to its unipolar counterpart, while maintaining a similar complication rate.
Many authors have shown that THA to be a superior treatment modality in relieving pain and improving mobility and with a better survival in the long term. A study by Baker et al. 6 consisted of 81 patients randomized to receive either a total hip replacement or unipolar hemiarthroplasty. The total hip group walked farther than the hemiarthroplasty group, as well as a better Oxford hip score on a mean follow-up of 3 years. The same cohort was followed up later by Avery et al. 26 (mean follow-up 9 years) suggesting a superior function and less reoperation in the total hip group although not statistically significant.
Another study by Blomfeldt et al. 5 randomized 120 patients, with a mean age of 81, to either a total hip replacement or a bipolar hemiarthroplasty. The former group showed a better Harris hip score at 1 year of follow-up. However, despite a trend for the total hip group to have better quality of life measurement, the results were not statistically significant. The total hip group also experienced greater operative blood loss and longer operative time.
The more expensive total hip implant also has its drawbacks. In many studies reviewed, THA runs a higher rate of dislocation. A meta-analysis by Hopley et al. 7 comparing total hip against hemiarthroplasty showed a 45% relative or 1% absolute risk in dislocation with total hip replacement. Meta-analyses by Wang et al. 9 and Yu et al. 10 also reported higher dislocation rate with THA compared with hemiarthroplasty. When Blomfeldt et al. 5 reported a zero dislocation rate, all the cases included were performed by consultants with modified Hardinge approach.
THA is simply a much higher magnitude of surgery, requiring special surgical expertise. With the tremendous caseload in our locality, it might not be feasible to involve a joint specialist in every hip fracture case. When total hip replacement is performed as emergency cases by trainees or specialists not trained in joint replacement, the complication rate is bound to increase.
In our cohort of bipolar hemiarthroplasties, there was no dislocation or periprosthetic fracture. Mean Harris hip score for pain in our living patients was 40.6 of 44 at an average follow-up of 13.1 years (range: 8.2–18.3 years). Many of our patients remain pain free. Considering most of the surgeries (65%) were completed by trainee surgeons with specialist supervision, bipolar hemiarthroplasty is a cost-effective option with excellent results and low revision rate.
Such excellent results are not limited to our own centre. Haidukewych et al. 27 have conducted a similar study which included 212 bipolar hemiarthroplasties. Survival rates were similar in his population with 10-year survivorship free of reoperation for any reason at 93.6%, for aseptic femoral loosening at 96.5% and acetabular cartilage wear at 99.4%. A drawback of his study was the use of various head and stem designs in his cohort. In contrast, we have reviewed the long-term outcome of a single type of bipolar hemiarthroplasty, performed selectively on patients with good premorbid function in this retrospective study. The long-term clinical and radiographic results were excellent and reproducible.
In conclusion, we report an excellent clinical and radiological result with the use of the bipolar hemiarthroplasty in long-term follow-up. While the advantage of THA in young hip fractures should not be undermined, bipolar hemiarthroplasty has shown an excellent long-term survivorship with minimal acetabular erosion. The bipolar implant increases our armamentarium in managing the heterogeneous population suffering from hip fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.