
Abstract
Introduction:
There has been a global trend towards individually packaged screws for orthopaedic operations. Traditional practice makes use of screw caddies that require re-sterilization. Individually wrapped screws (IWS) are purported to decrease infection rates and avoid the deleterious effects of repeated screw sterilizations, despite marginal evidence. This review aimed to evaluate the safety, effectiveness and economics of screw caddies with IWS.
Material and methods:
The literature was surveyed in a systematic fashion between 1998 and 2017 and all relevant health technology assessments, systematic reviews, meta-analyses, randomized controlled trials, cohort studies, case-controlled studies and case series were sought. Any benefits or otherwise of IWS over screw caddies were then evaluated in the areas of safety, effectiveness and economics.
Results:
Two level III-3 papers suggested the use of caddies at least as safe as individual screws. Four level III-2 papers demonstrated that screws from caddies were as effective as individual alternatives, while a level III-3 paper reported that individual screws were significantly more expensive than screw caddies. Cost increases to our regional health service from ankle open reduction and internal fixations alone of at least $50,112 (AUD) per annum were calculated.
Conclusions:
From the results obtained, the authors recommend the continued use of screw caddies for orthopaedic procedures.
Introduction
Certain fractures require surgical management by open reduction and internal fixation (ORIF). This involves stabilization of a fracture by means of a plate coupled with screws. 1 At the authors’ principal place of practice (a secondary level referral hospital in NSW, Australia), local policy now dictates that screws are to be retrieved from individual packages (Figure 1). Until recently these screws had been retrieved from screw caddies (Figure 2). This is a global trend that some health systems are now adopting based on concerns that screws in caddies cannot be properly sterilized and are weakened by the process. 2 Presently, there exists limited evidence to prove these assertions, and this begs the question as to why policies are changing for individually wrapped screws (IWS) to be utilized in preference over screw caddies.

An example of an individually wrapped screw and the inner packaging that risks becoming contaminated when removal from the outer element is undertaken.
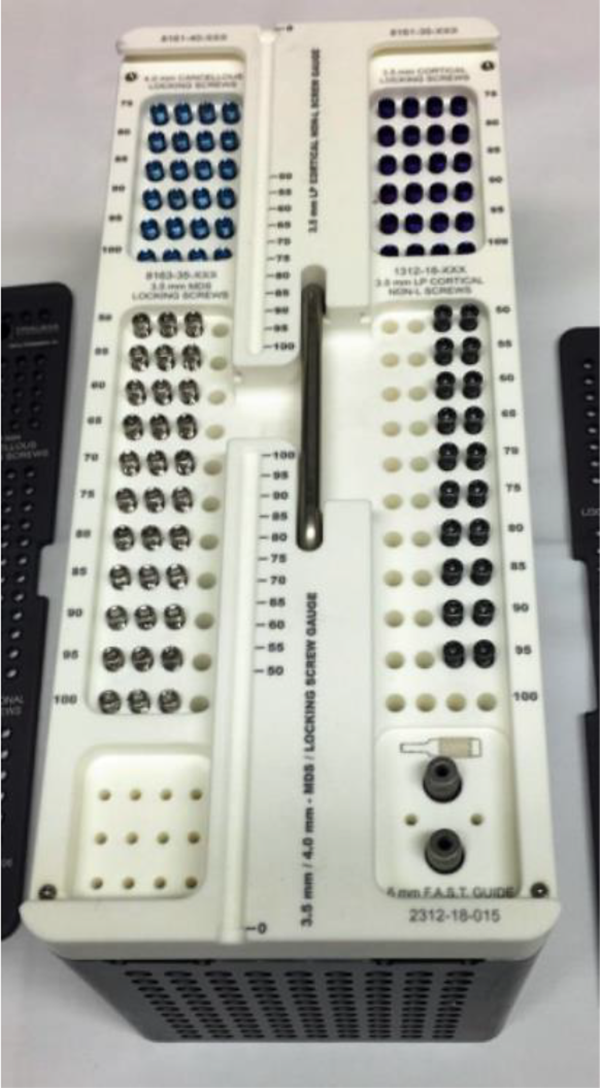
An example of screws as presented in a caddy. Once opened at the beginning of the case, the entire apparatus remains in the sterile operative environment.
Health technology assessments (HTAs) represent a multidisciplinary field of policy analysis that studies, among other things, the medical and economic implications of medical technology development and its implementation. 3 In Australia, the Medical Services Advisory Committee is an independent non-statutory committee responsible for conducting HTAs to advise the Federal Minister for Health on the funding of medical services. In doing so, the committee’s terms of reference require it to consider ‘the strength of evidence in relation to the comparative safety, effectiveness, cost-effectiveness and total cost of the medical service’ under assessment. 4 At the local level, the number of university hospitals worldwide performing hospital-based HTAs have increased over the last decade. 5 HTAs require decision-making processes that are fair, equitable and transparent. 6 Appropriating this ethos it is the authors’ intent in this review article to conduct an appraisal of the safety, effectiveness and cost-effectiveness of IWS usage when compared to screw caddies during orthopaedic procedures.
Material and methods
The medical literature was searched to identify relevant studies between 1998 and January 2017. This search was conducted via the Medline database and search string terms of ‘orthopedic, orthopedic screw, bone screw, fracture fixation, orthopedic procedure, screw bank, screw rack and screw caddy’ were applied and then combined. These results were then overlapped with the combined terms of ‘product packaging and packaging’. A snowball search of the literature was thereafter undertaken to identify any additional relevant studies and reviews for this time period.
For the purposes of this assessment, the index intervention was the use of IWS and the comparator was the use of a screw caddy. The three main HTA assessment parameters (safety, effectiveness and cost-effectiveness) were addressed by assessment of contamination risk (safety), insertional and fracture torque (effectiveness), and operating time and cost (cost-effectiveness). These parameters were chosen as they aligned with the arguments previously documented in support of the use of IWS.
Inclusion criteria were HTAs, systematic reviews, meta-analyses, randomized controlled trials (RCTs), other controlled trials, comparative studies, cohort studies and case series regardless of language used. Narrative reviews, editorials, letters, articles in abstract form only and individual case reports were excluded. Each included study was assessed according to the National Health and Medical Research Council (NHMRC) evidence hierarchy. 7
Data were extracted for this assessment by one review (MH) and checked by a second (PL). Cross-examination of the studies presented via the NHMRC hierarchy was overseen by the final authors (AMS and LAA). The literature was surveyed and data have been presented in a systematic fashion.
An assessment was then made with respect to the relative safety, effectiveness and cost-effectiveness of the screw rack versus IWS.
Results
Our search identified 16 unique records. Of these, 2 were included for the assessment of safety, 1 for the assessment of cost-effectiveness and 13 were excluded because they did not meet our inclusion criteria. A snowball search of the literature further identified four relevant studies for the assessment of effectiveness. In total, seven studies were included (see Figure 3).
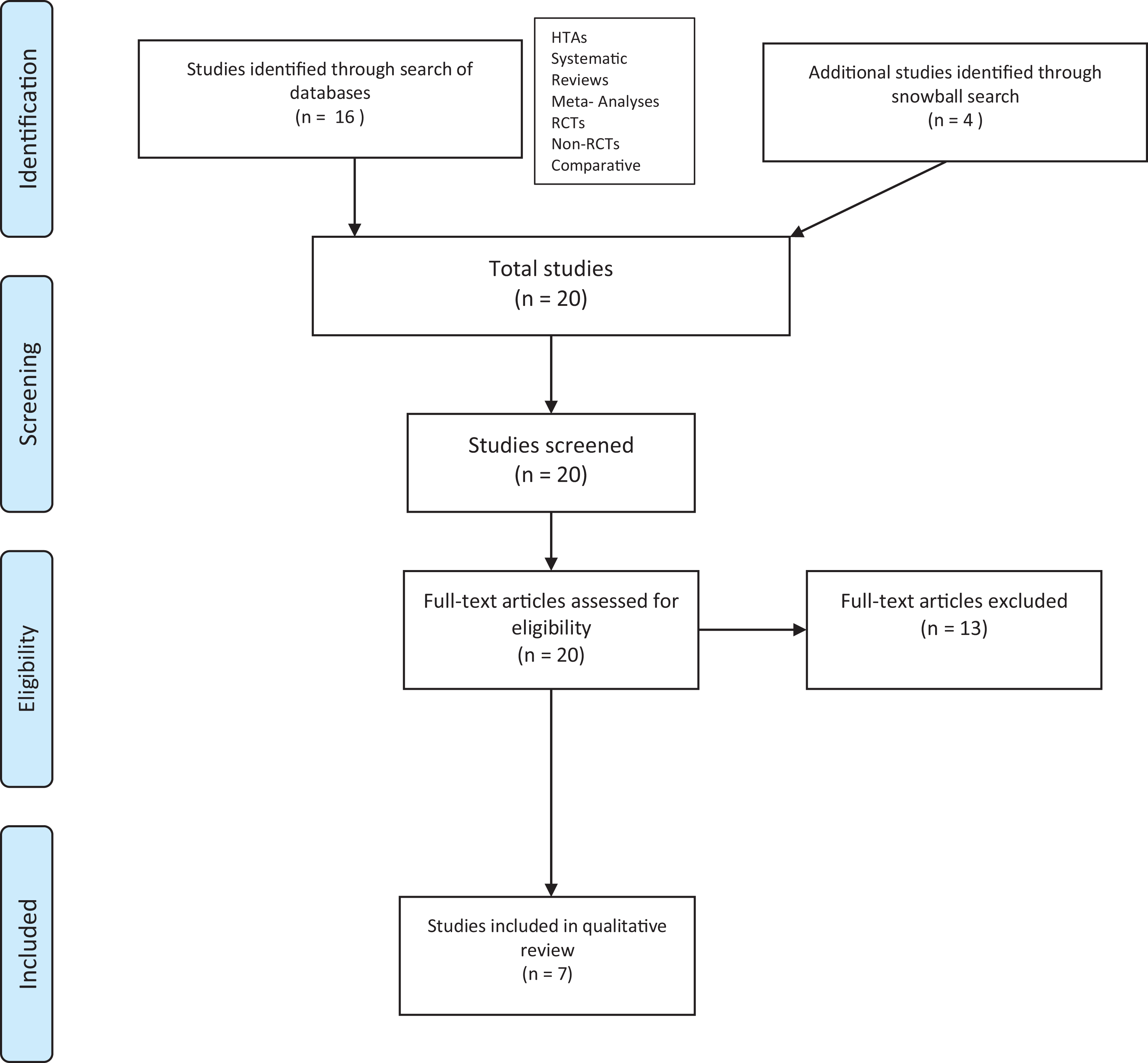
Selection algorithm for included studies.
Safety
Two level III-3 papers demonstrated an increased risk for infection when IWS are used in preference to screw caddies. Smith et al. cultured screw packets that were opened using standard operating theatre protocol. 8 They found that the act of opening packets yielded a growth in 7/50 cases. This contrasted with no growth on control Petri dishes that were left open to air in the same theatre.
While not statistically significant (p = 0.50), Smith et al. considered the result to be clinically relevant (see Figure 4).

The results of the relevant papers as cross-referenced with the criteria of an HTA to evaluate appropriateness of an intervention for the health system to generate optimum value for government. Further details of the studies may be seen in Online Supplemental Figure A1. HTA: health technology assessment.
Crick et al. used a cream designed to be visible only under ultraviolet light to identify any contamination during the opening of screws as if being carried out during an operation. 9 One out of 100 screws was noted to be contaminated, while no contamination was noted from a screw bank used as a control. The statistical significance of this result was unclear, but in concert with Smith et al.’s findings there is no justification to change policy to the use of IWS (see Figure 4).
Anderssen et al. postulated that the use of IWS also has the potential to increase traffic flow in and out of the theatre. 10 He noted a strong positive correlation between colony-forming units in the air and total traffic flow per operation (r = 0.74; p = 0.001; n = 24).
Effectiveness
While no papers were returned from the Medline search, four papers (level III-2) were identified via a snowball search. These examined the efficacy of orthodontic screws subjected to repeated sterilization. The authors considered these an adequate appropriation to orthopaedic screws given their similar surgical requirements to maintain stability within teeth, essentially an extension of the bony skeleton.
Firstly, Mattos et al. subjected implants from various manufacturers to a cycle of sterilization and compared them to a control group of ‘as-received’ implants. 11 They found that the effect of the autoclaving process did not have a statistically significant effect on the implants’ resistance to fracture (p = 0.411). Akyalcin et al. divided mini-screws into groups that were sterilized using a steam autoclave 1, 5 and 10 times. 12 All screws were then inserted into blocks simulating mandibular bone and while there was some variability in maximum insertion torque and lateral displacement force, the authors found that this bore no clinical relevance to stability. Noorollahian et al. assessed the effects of reprocessing and reusing titanium mini-screws when it came to fracture torque. 13 Fracture torque was assessed after five cycles of insertion, cleaning, processing and sterilizing with autoclave as compared with a control group. The authors found no significant difference between the groups (p = 0.485). Finally, Estelita et al. evaluated the effect of recycling processes on the torsional strength of mini-screws. 14 A total of 200 mini-screws were divided into groups of unused implants, inserted/removed implants, removed implants then subjected to sonification and autoclave sterilization, and removed implants then subjected to sonification, sandblasting and autoclave sterilization. The authors found that the torsional strength of screws was not affected by the recycling process, even when sandblasting was added (see Figure 4).
Cost-effectiveness
A comprehensive cost-effectiveness analysis on the use of IWS was not identified from the Medline search. A single-centred study (level III-3) by Man et al. was identified comparing the acquisition time of individually packaged screws and screws from a rack. 15 They found that the use of individually packaged screws significantly (p < 0.001) increased operating time by 96 s per screw. Application of this cost per minute data to the authors’ hospital operating suite showed significant additional costing. During the 12 months ending in November 2016, 87 ankle ORIF procedures were performed. Increased costs for these ORIFs were in excess of $50,000. This was calculated from a proposed benchmark for the cost per minute to run an operating theatre of between $40 and $45. 16 Finally, these costs were extrapolated for ankle ORIFs alone. It is logical that projected increased costs encompassing all ORIFs would be significantly higher (see Table 1 and Figure 4).
Estimated savings for ankle ORIFs at authors

ORIF: open reduction and internal fixation; OR: operating room; p.a.: per annum.
Discussion
Australia’s national HTA process is intended to ensure the ‘optimum value for money in the Government’s subsidisation of medical services, as well as prioritising the uptake of effective new technologies and procedures’. 17 At a local level, HTAs have been shown to have a positive influence on hospital decision-making and budgets, as well as positive perceptions from managers and clinicians. 5
This review article has appropriated the HTA method to evaluate whether IWS are superior to the use of screw caddies. Applying the HTA domains of safety, effectiveness and cost-effectiveness, our assessment suggests that the use of a screw caddy is no worse and indeed significantly cheaper and likely safer than the use of individually packaged screws. While the literature has been assessed in a manner akin to a systematic review, the data have been presented in a manner to reflect the unique evaluation algorithm for such HTAs since the arguments for IWS or otherwise surround this context.
HTAs are commonly limited by the availability of higher level evidence, something on which they depend. This is especially noteworthy in surgery due to historical difficulties cited in gathering high evidence for the assessment of safety and effectiveness given there is reticence to test a change of traditional practice when it has demonstrated effectiveness and benefit for patients. Indeed, one Australian study noted that only 19.6% of performed orthopaedic procedures had at least one low risk of bias RCT supporting operative treatment over non-operative alternatives. 18 This shortcoming extends to the comparison of caddies with IWS.
The requirement for further high-powered studies to evaluate cost-effectiveness within orthopaedic surgery is without question. Brauer et al. suggested a lack of level I evidence in orthopaedic surgery has limited the ability to perform high-quality cost analyses. 19 Furthermore, they claimed that when performed, cost analyses in orthopaedic surgery were of lower quality than those in other areas of medicine. This review article’s cost-saving calculation does, however, give useful data in comparing screw caddies with IWS. Furthermore, it demonstrates that definitive calculation of cost-effectiveness is necessary (and possible) in preference to an ad hoc and reactionary approach to policy implementation based on questionable claims. Poorly evaluated decisions can have flow-on effects with respect to safety, effectiveness and cost-effectiveness on a day-to-day basis and indeed, such an approach has been taken by HTAs with respect to screw caddies and the surgical count. NSW Health Policy dictates that ‘a mandatory accountable item is a reusable or disposable item which by its nature is at risk of being retained in the patient. It is therefore subject to mandatory documentation on the count sheet’. 20 A screw removed from a screw caddy and used during the course of an orthopaedic procedure would fall under this aforementioned definition, however, it is debatable that a screw left within the caddy during the procedure constitutes such a risk.
To compound this lack of clarity, there exists a varied interpretation of this statement among NSW hospitals and it is our experience that informal protocols are determined on a site-by-site basis. The authors propose that a consensus should be agreed upon by clinicians and administrators to clarify this doubt.
The potential for implants to be ‘traceable’ in the post-operative period is often touted as a justification for a move towards the use of individually packaged screws. While this concept may seem sensible, there is a lack of any literature to support this need. Furthermore, many authors and surgeons have proposed that caddies have a long and established track record in orthopaedics without problems, and these experienced end users have never witnessed any situation whereby implants have needed to be traced post insertion. At the very least, the benefit of tracking individual screws post insertion is yet to be proven. 15 Furthermore, even if IWS could be traced down to a ‘batch number’, the actual screw in question may still not be traceable because frequently in such operative procedures, multiple screws of the same length are utilized and could therefore not be individually traced.
This capacity for ‘tracing’ IWS may further be compromised even before the hardware reaches hospitals and sterilization units. Xiaolian et al., who have investigated errors based on surgical tracking systems, revealed that personnel elements were the primary cause for packaging errors, referring to the contents inside. 21 Their findings further showed that similarly shaped individually wrapped hardware with separate differentiating tags were packaged incorrectly due to mistakes when reading the small font of the tags in order to differentiate the similarly sized and shaped contents for packaging. While such errors could conceivably follow through the hospital system, more relevantly they nullify any tracing option if individual screws were mislabelled at the source, thus weakening the argument that IWS are superior to racks for this reason. In addition, the established grouping of screws in caddies, without individual tags or serials, may limit such misreads and mistakes in packaging.
This review article does have its limitations, not least of which is the lack of high-powered studies available to compare IWS with screw caddies. The authors would argue, however, that weak as the evidence is, it does demonstrate a trend towards the superiority of caddies over IWS. There does not appear to be any useful evidence to suggest the contrary, even though such ‘evidence’ has been proposed as an impetus for instigating this policy change in several hospitals. Criticism may be justified over our approximation of orthodontic screws to orthopaedic screws but in the absence of available evidence specific to orthopaedic screws, the approach adopted was considered reasonable given the similar constitution of both screws, the comparable medium in which they are required to maintain fixation, and similar parameters, such as fracture risk and insertion torque, used to judge their effectiveness.
Conclusions
Despite the paucity of high-powered evidence available for the comparison of IWS and those from caddies, this systematic review reveals thorough doubt on the notion that IWS are superior to the screw caddy in terms of safety, effectiveness and cost-effectiveness. Indeed, the literature currently suggests that IWS are no more effective and considerably more expensive. At the very least, there is a dire need to more thoroughly examine the effects of the IWS and those in caddies in larger higher quality studies. Furthermore, our interpretation of the literature in this area highlights the wider danger of ad hoc health policy dictation without substantiated evidence.
Supplemental material
Supplemental Material, Appendix_figure_A-1 - A comparison of risk profile for orthopaedic operations when utilizing individually wrapped screws (IWS) when compared with sterile screw caddies (screw racks)
Supplemental Material, Appendix_figure_A-1 for A comparison of risk profile for orthopaedic operations when utilizing individually wrapped screws (IWS) when compared with sterile screw caddies (screw racks) by Andrew M Suchowersky, Martin Hua, Peter Lorentzos and L Andrew Ashton in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.