
Abstract
Purpose:
This study aims to investigate further how the coronavirus disease 2019 (COVID-19) pandemic is affecting orthopaedic surgeon in Malaysia in terms of exposure, general perceptions of risk, and the impact on their current and future practice.
Methods:
Orthopaedic surgeons nationwide were invited through email and text messages to answer an online self-administered questionnaire collecting demographic information, COVID-19 exposure experience, perception of risk, and impact on orthopaedic practice.
Results:
Of the respondents, 4.7% and 14.0% were involved in frontline treatment for COVID-19 patients with non-orthopaedic and orthopaedic problem, respectively. Respondents working in Ministry of Health had highest percentage of involvement as frontliner, 7.8% (8/103) and 20.4% (21/103) for non-orthopaedic and orthopaedic related COVID-19 treatment, respectively (not significant). Their main concern was an infection of family members (125/235, 53.2%). Majority of respondents were still working (223/235, 94.9%), running outpatient clinics (168/223, 75.3%), and continued with their semi-emergency (190/223, 85.2%) and emergency surgeries (213/223, 95.5%). Of the surgeons, 11.2% (25/223) did not screen their patients for COVID-19 prior to elective surgeries, 30.9% (69/223) did not have any training on proper handling of personal protective equipment (PPE), 84.8% (189/223) make decision to manage more conservatively due to COVID-19 and 61.9% (138/223) had their income affected. Of the surgeons, 19.3% (43/223) started using telehealth facilities.
Conclusion:
Direct exposure to treatment of COVID-19 patients among the respondent is low and the main concern was infecting their family member. There are still several surgeons who did not conduct preoperative COVID-19 screening and practice without proper PPE training.
Keywords
Introduction
The finding of the new coronavirus Wuhan in late 2019 has alerted medical professionals worldwide. 1 The virus was named as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is a successor of SARS-CoV-1 that caused SARS back in 2002. 2 The disease was named coronavirus disease 2019 (COVID-19), following the guide on the best practice for naming human infectious diseases by World Health Organization focusing on the causal pathogen and the year of its first detection. 3
As of 16 April 2020, Malaysia has the highest number of confirmed cases in Southeast Asia. The reported cases have reached 5182 with 2332 (45.0%) actively treated cases, 2766 (53.4%) recovered, and 84 deaths (1.6%). 4 Following the second wave of COVID-19 outbreak in late February in this country, Malaysia has started a 14-day movement control order (MCO) from 18 March 2020 to reduce the rate and to break the chain of infection. 5 We are currently at the fourth phase of MCO ending on the 12 May 2020. 6
The present ratio of orthopaedic surgeons to the population of Malaysia is 1:50,000 7 and the specialty may not be directly involved in the pandemic in general. Nonetheless, the specialty contributes indirectly in helping the management of the COVID-19 patients, reduces the chance of nosocomial infection and prevents transmission to healthcare workers. These changes were made according to the general guidelines provided by the Ministry of Health (MOH), Malaysia, along with other published guidelines on surgical management during COVID-19. 8 Orthopaedic cases are still being managed in almost all hospitals nationwide. COVID-19 has affected surgeons who continued to practice despite the outbreak with respect to their exposure risks, perceptions, and practice routines. Early sharing of relevant information and strategies has helped most surgeons to cope with the rising challenges to continue their practice during this trying time. Many surgeons have been continuously planning and hopefully moving in the same direction with respect to the current “safe” practice and adopting to the “new normal” practice routines. Nevertheless, the actual effects of COVID-19 pandemic on their daily practice were still not clear.
Considering the situation, this study aims to investigate how COVID-19 pandemic is affecting orthopaedic surgeon in Malaysia in terms of exposure, general perceptions of risk and the impact on the orthopaedic surgeons’ current and future practice.
Materials and methods
Study design and participants
This study was a cross-sectional survey. Starting on 7 April 2020, the study lasted for nine days, during which, the number of confirmed cases was increasing, and this was the third week of MCO implemented in our country. Orthopaedic surgeons from all states of Malaysia (Johor, Kedah, Kelantan, Melaka, Negeri Sembilan, Pahang, Pulau Pinang, Perak, Perlis, Selangor, Terengganu, Sabah, Sarawak and Federal Territories (Kuala Lumpur, Labuan and Putrajaya)) were invited. There are 804 orthopaedic surgeons registered in the National Specialist Register (NSR), however, the exact number of surgeons who are actively practicing was unknown. The invitation to answer the structured questionnaires was distributed via (1) email from NSR, (2) the mailing list of the Malaysian Orthopaedic Association (MOA) and (3) additional Whatsapp text messages with a link to the questionnaire. The respondents could decide whether to participate in the study by giving digital informed consent. The survey was anonymous, and confidentiality of information was assured. Only a single response to the questionnaire was permitted for each participant. The questionnaire includes four parts: basic demographic data, the occupational exposure experience, risk perception of COVID-19 and the impact of COVID-19 on orthopaedic surgery practice.
Questionnaire on basic demographic data, exposure to COVID-19, perception of risk and impact on orthopaedic practice
Demographic information, such as age groups, gender, marital status, work experience as orthopaedic surgeon, level of training, geographic location of practice, and environment of practice, were collected.
Participants were then asked about COVID-19 exposure experience related to their involvement in treating COVID-19 patient with or without orthopaedic-related problem or volunteering in treating COVID-19 patients. Questions on COVID-19 exposure such as having gone through quarantine or isolation, self-infected, and family members infected were also included.
Five questions were designed to investigate the perception of risk of COVID-19 infection. A five-point Likert scale was assigned, with a lower score indicating a higher concern. The five questions focused on concerns on self-infection, family members, colleagues at the frontline, protective measure and the current prevention and control strategy.
Fourteen questions were then asked to investigate the impact of COVID-19 on orthopaedic practice.
The questions used were listed in Table 1.
Questions used in “The impact of COVID-19 pandemic on orthopaedic fraternity in Malaysia” questionnaire.
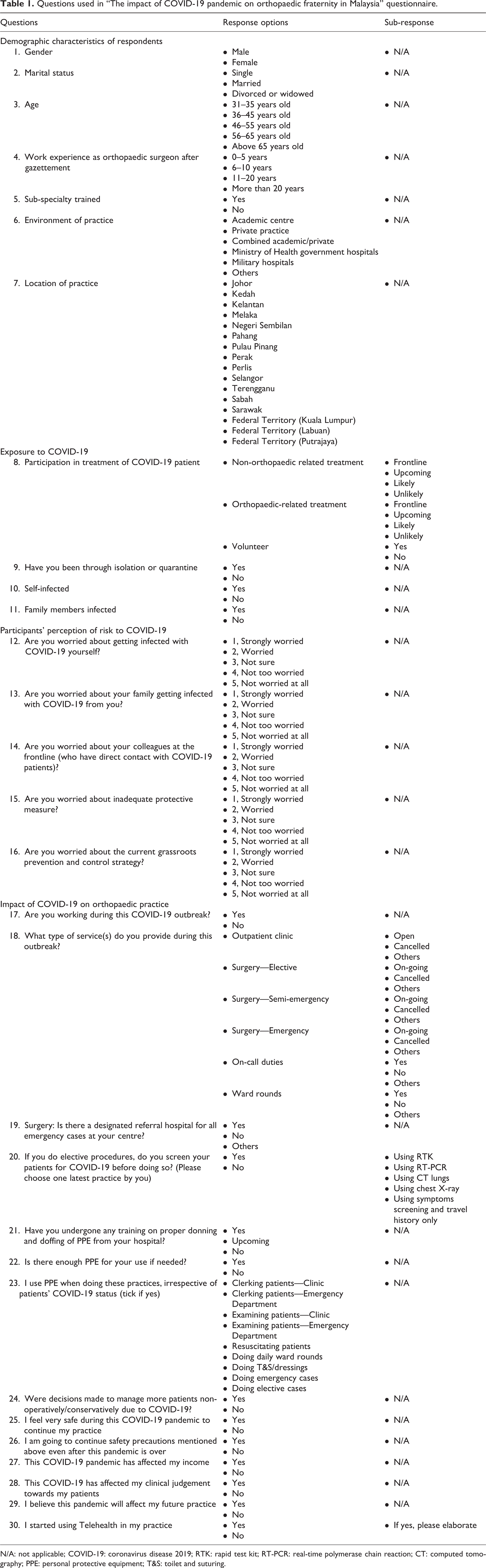
N/A: not applicable; COVID-19: coronavirus disease 2019; RTK: rapid test kit; RT-PCR: real-time polymerase chain reaction; CT: computed tomography; PPE: personal protective equipment; T&S: toilet and suturing.
Statistical analysis
All analyses were performed with Statistical Product and Service Solutions 22.0. Significant level was set at p <0.05. Categorical variables were presented as numbers and percentages. Exposure experience to COVID-19 comparing different regions and groups was analyzed by mean of χ 2 tests. Independent t-test and analysis of variance (ANOVA) test were used to analyze the five-point Likert scale. ANOVA was then followed by Tukey’s post hoc test.
Results
Demographic characteristics
A total number of 235 responses were collected. Most of the respondents were male (202, 85.96%), were aged 36–45 years (120, 51.06%), were married (217, 92.34%), were in orthopaedic practices between 0 years and 5 years (90, 38.30%), and worked in MOH government hospitals (103, 43.83%; Table 2). Of the respondents, 62 (26.38%) worked in Kuala Lumpur and 59 (25.11%) worked in Selangor, 114 (48.51%) worked outside the capital of Malaysia (Figure 1). As Kuala Lumpur and Selangor are more densely populated, more orthopaedic surgeons were located here.
Demographic characteristics of the respondents of the study regarding the impact of COVID-19 on orthopaedic practice in Malaysia.


Map of Malaysia showing the distribution of respondents according to states.
COVID-19 exposure
Of the respondents, 11/235 (4.7%) are involved in frontline treatment of COVID-19 patients with no orthopaedic-related problem. Although not significant, majority of them came from MOH hospitals (8/11 of frontliners, 72.7%).
By looking at the environment of practice, respondents working in MOH had highest percentage of involvement (8/103 respondents in MOH, 7.8%) compared with those working in private (3/70 respondents in private, 4.3%; Table 3). They are mainly involved in screening and monitoring COVID-19 patients alongside with infectious disease team and they are not directly involved in active treatment of the patients. The authors believe that those who were involved as frontliners for non-orthopeadic related patients have received a briefing on standard precautions and refreshers before starting their duty. 9
COVID-19 exposure experiences of respondents in non-orthopaedic related treatment differentiated by environment of practice.
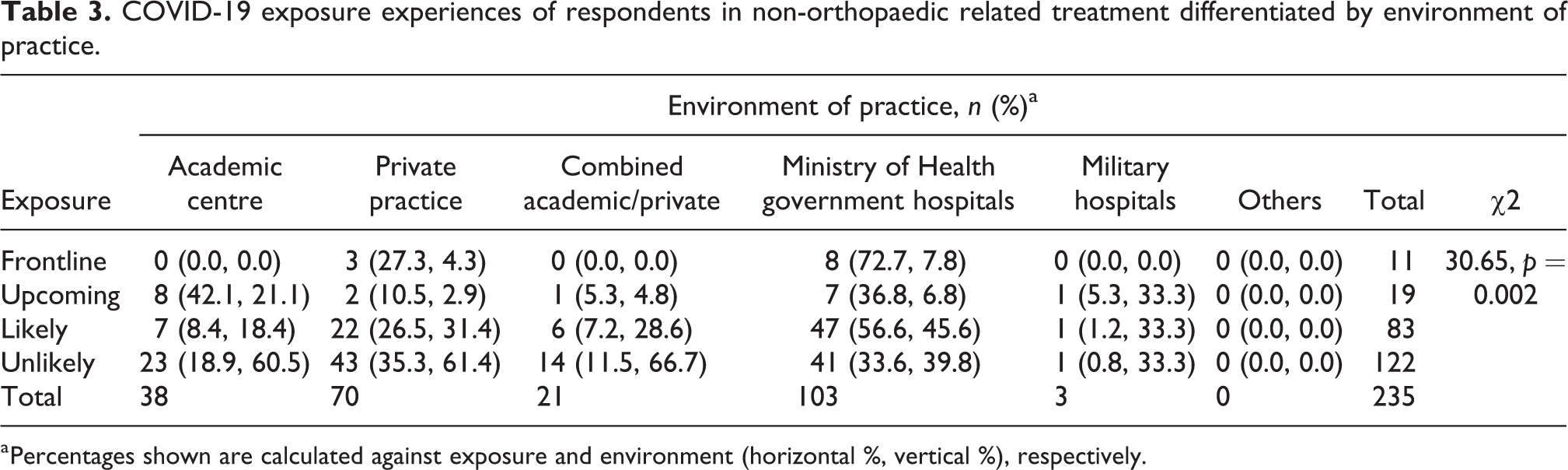
a Percentages shown are calculated against exposure and environment (horizontal %, vertical %), respectively.
Of the respondents, 33/235 (14.0%) are involved in frontline orthopaedic treatment of COVID-19 patients. Involvement of frontline orthopaedic treatment of COVID-19 patients was also higher in MOH hospitals (21/33 of frontliners, 63.6%).
By comparing place of practice, respondents working in MOH had a higher percentage of involvement (21/103 of MOH orthopaedic surgeons, 20.4%). This was followed by private practice (9/70, 12.9%), combined academic centre and private practice (2/21, 9.5%) and academic centre (1.38, 2.6%). In addition, Perak, a state outside the capital of Malaysia, has the highest percentage of frontliners involved (4/13 of respondents from Perak, 30.8%) when compared according to regions (Table 4). However, these findings on the frontline group are not statistically significant.
COVID-19 exposure experiences of respondents in orthopaedic-related treatment differentiated by environment of practice and location of practice.
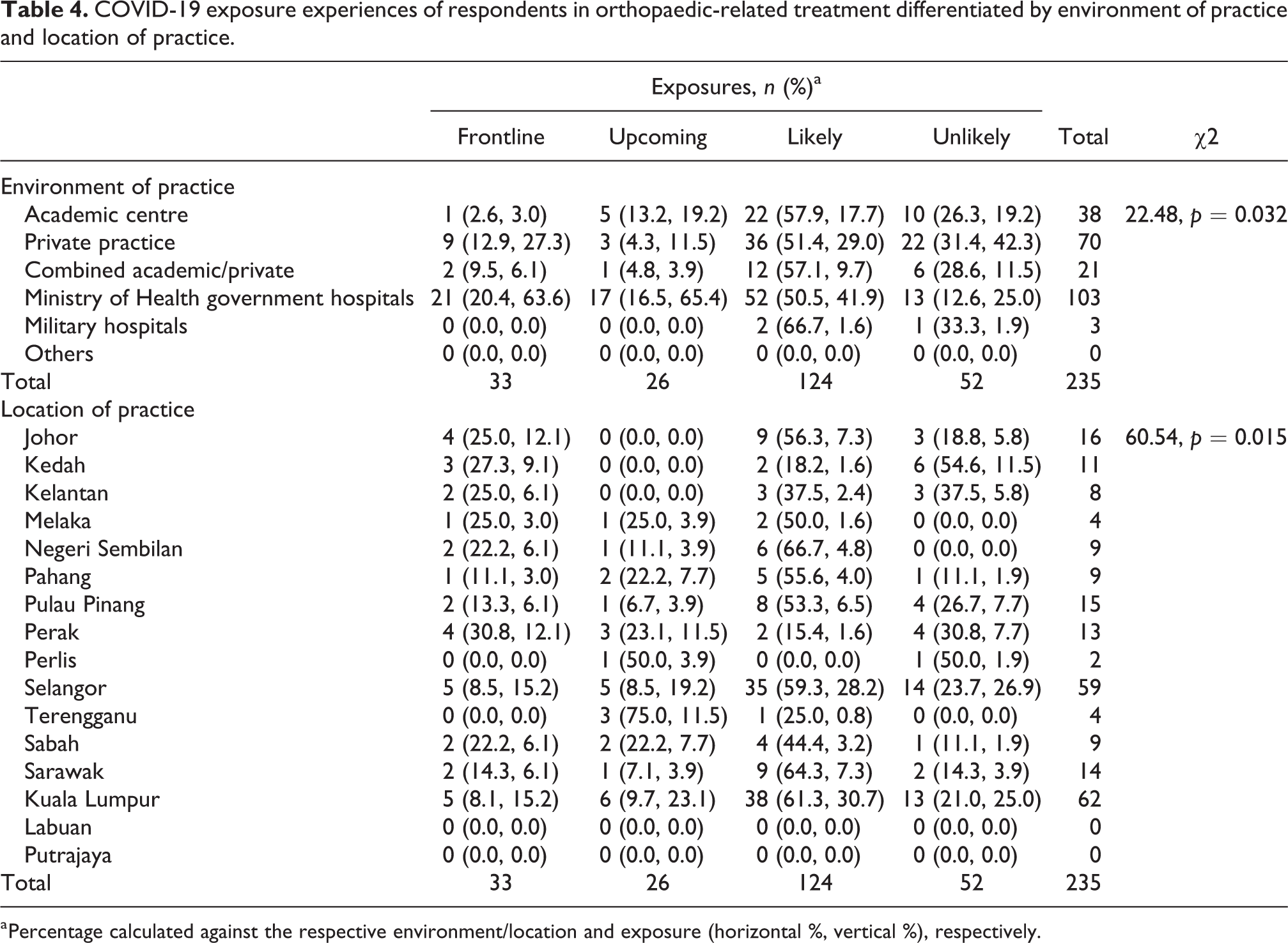
a Percentage calculated against the respective environment/location and exposure (horizontal %, vertical %), respectively.
Fifty-six (23.8%) of the respondents have volunteered to participate in treatment of COVID-19 patients with orthopaedic-related problems. These respondents have received a training on proper use of personal protective equipment (PPE) during treatment. 9
There is no significant difference in COVID-19 exposure, both as frontliners or volunteers, in terms of age, years of practice and regardless of subspecialty trained. However, there is a higher percentage of respondents in the junior years of practice (0–5 years) being involved in frontline orthopaedic treatment of COVID-19 patients.
Thirty-six (15.3%) of the respondents reported to have been through self-isolation or quarantine. The reasons given include recent travel history, symptoms of COVID-19 and exposure to COVID-19 positive patients both at work, home and own social gatherings. None of the respondents were infected, whereas four (1.7%) of the respondents have family members who are infected. These responses were self-reported as the questionnaire did not include additional remarks on the tests conducted or how their family members got infected. However, the authors believe that some respondents might have gone through nasopharyngeal swab tests following a close contact with patients or other factors. On the other hand, the family members who were infected might have contracted the virus through other means.
Risk perception
The main concerns of the respondents were getting family members infected (53.2%), infection of colleagues at frontline (49.8%) and protective measures (48.9%). Of the respondents, 30.6% expressed being strongly worried about self-infection. Only 22.6% expressed being strongly worried about current prevention and control methods (Figure 2).

Distribution of risk perception of COVID-19 among the respondents. COVID-19: coronavirus disease 2019.
Respondents between 6 years and 10 years in practice were significantly more worried about their family members being infected compared to those who have been in practice for more than 20 years (F = 2.7, p = 0.05).
Among the different practice environments, respondents working at MOH hospitals were significantly more worried about current prevention and control strategy compared to respondents working at academic centres and combined academic/private setting (F = 4.7, p = 0.001).
Impact on orthopaedic practice
Majority of all respondents (94.9%) were still working during this COVID-19 pandemic. 75.3% still opened their outpatient clinics, while 4.9% have closed their outpatient services completely with majority (68.4%) of them were due to a directive from the higher authority. The other 19.7% of total respondents gave input that their outpatient services were cut down in frequency and continued mainly for their post-operative, trauma or malignancy cases only, among others.
Examples of surgery cases according to categories were summarized in Table 5. Elective surgical cases were cancelled by 90.1% of respondents, with three quarters of them not doing surgery due to directive from their administration, and the rest by personal choice. Then, 6.3% continued with their elective surgeries.
Categories and examples of surgery cases: elective, semi-emergency and emergency.

Semi-emergency and emergency cases continued to be performed by 85.2% and 95.5% of surgeons, respectively, with those not performing these surgeries referring their cases to other hospitals. The majority of those not performing these surgeries (14.8% and 4.5%) had stopped doing so due to directive from their administrative authority. Only 38.1% of the respondents had designated referral hospitals for emergency cases, while 59.2% did not have. One respondent brought up the issue of not having an officially designated referral hospital to refer their cases, hence facing difficulties to refer their cases out. Most respondents continued to do on-call services (96%) and ward rounds (90.1%) during the COVID-19 pandemic.
Of the surgeons, 11.2% did not screen their patients for COVID-19 infections before performing elective surgeries by any means (Figure 3). The majority (60.5%) did real-time polymerase chain reaction (RT-PCR) test before surgery, 20.2% used symptoms and travel history, while the rest used serology kit (4.9%), chest radiographs (2.7%) and computed tomography scan of the lungs (0.4%).

COVID-19 screening on patients prior to elective procedures. CT-scan: computed tomography scan; RT-PCR: real-time polymerase chain reaction.
With regard to PPE, 31% respondents did not have any training by their hospitals on proper donning and doffing, while 47.5% have undergone the process and the rest (21.5%) will be training soon. Of the surgeons, 41.3% did not think that PPE supply in their hospital were sufficient.
The usage of PPEs was low in resuscitating patients (38.1%) and in doing elective cases (44.4%) while almost 90% of surgeons used PPEs in their emergency surgeries. These three situations involve potential aerosol-producing procedures (Figure 4).

The usage of PPEs in daily routine of respondents. ED: emergency department; T&S: toilet and suturing; PPE: personal protective equipment.
The respondents (84.8%) were made to manage more of their patients conservatively due to COVID-19 with the other 15.2% not changing their management armamentarium. About 87.4% felt that they do not feel safe to practice during this outbreak, with 85.2% admitting that they would continue to exercise safety precautions even after the pandemic is over.
Of the surgeons, 61.9% claimed that the outbreak had affected their income due to reduced number of patients and procedures performed. Although only one-third of the respondents are practicing in the private sector, most senior orthopaedic surgeons from government sector and academic centres, whose income is relatively fixed, are also allowed to conduct a part-time private practice. Therefore, their overall income was also indirectly affected by this pandemic.
Of the respondents, 73.1% felt that the pandemic will affect their future practice. However, more than half (56.5%) of the respondents agreed that COVID-19 had not affected their judgement in managing their patients.
Essentially, only 19.3% of the surgeons had started using telehealth facilities during this pandemic, mainly for meetings, webinars, rearrangement of appointments and online CME or teaching. Some used telehealth for teleconsultations with patients for non-urgent opinions, virtual follow-ups, and to communicate with their foreign patients, who were unable to make their appointment trip into Malaysia due to travel restrictions. The other 80.7% of respondents have not started using telehealth facilities. The possible reasons could be due to the lack of awareness on the role of telehealth facilities in orthopaedic surgeons’ practices, the fear of breaching doctor-patient confidentiality and the use of telehealth in this country is not yet widespread.
Discussion
The COVID-19 pandemic has taken the world by storm, 10 creating a huge strain on global healthcare system and subsequently affecting orthopaedic services and surgeons around the world. With high infection transmission risk, 11,12 orthopaedic surgeons would have to take all necessary precautions at their workplace to minimize their risk of contracting this highly contagious disease. A study done in Wuhan among orthopaedic surgeons found that surgeons were infected at their workplace and were also infecting other co-workers. The suspected sites of exposure were general wards (79.2%), public places at the hospital (20.8%), operating rooms (12.5%), the intensive care unit (4.2%) and the outpatient clinic (4.2%). There was also transmission from these doctors to others in 25% of cases, including to family members (20.8%), colleagues, patients and friends (4.2% each). 1
In this cross-sectional survey, 51.4% of the respondents were working in Kuala Lumpur and Selangor, which were listed as red zone. Districts in Malaysia were categorized into different zones: red (areas with at least 41 COVID-19 positive cases); orange (20–40 cases); yellow (1–19 cases) and green (no case). Kuala Lumpur and Selangor recorded the highest number COVID-19 positive cases.
In this study, 4.7% of the respondents were involved in frontline treatment of COVID-19 patients with no orthopaedic problem and 14.0% were involved in frontline orthopaedic treatment of COVID-19 patients. By comparing practice location, orthopaedic surgeons working in Perak are found to be more involved as frontliners. This is possibly due to limited healthcare manpower in a smaller district since the number of COVID-19 positive cases is only 250 compared to 1299 in Selangor and 899 in Kuala Lumpur on 14 April 2020. 13 Orthopaedic surgeons working in MOH hospitals had higher exposure to treating COVID-19 positive patients as all COVID-19 positive patients were being treated in MOH designated hospitals. In Hospital Kuala Lumpur, which is one of the MOH hospitals, for instance, medical officers, specialists and consultants were rostered to review patients in COVID-19 wards due to shortage of staff and increasing number of positive cases around mid-March. In big centres, there were also COVID-positive patients requiring orthopaedic management, such as for traumatic injuries or concurrent limb infections.
From this study, we found that the risk of COVID-19 exposure as frontline worker among the orthopaedic surgeons in Malaysia was low and none of the respondents was infected. This is credited to early awareness, infection prevention and control measures taken by hospitals following the general guideline provided by the MOH, Malaysia, along with other published guidelines on surgical management during COVID-19. 8
The main concerns of the respondents were worried about getting their family members infected. The group being significantly concerned were those in practice between 6 years and 10 years compared to those in practice for more than 20 years. In this case, we did not find any correlation although it is postulated that those in practice between 6 years and 10 years have living parents in the high-risk age group. It is in line with the situation in Malaysia, where the incidence per 100,000 populations was higher in people from 55 years to 59 years (31.5/100,000 populations) and 60–64 years of age (32.5/100,000 populations). Majority of the reported deaths in Malaysia involved patients above 60 years old (62.6%) and those with comorbidities (80.7%). 4
Only 22.6% of the respondents expressed to be very worried about current prevention and control methods. Apart from the MCO, orthopaedic specialty, especially in the government sector, has modified the routines to help in reducing the load in management of COVID-19 patients. Elective cases were postponed indefinitely; emergency and semi-emergency cases were treated with care in full PPE; outpatient clinics are also limited to urgent cases, such as trauma and tumor cases; and non-essential consultations were offered with longer duration prescription, rescheduled appointments and telephone or internet consultations. For postgraduate masters, orthopaedic training, their rotation posting, courses and Orthopaedic Specialty Committee Part 2 (final exit) examinations were also kept temporarily on hold. 14,15 Patient numbers (inpatients and especially, outpatients) have reduced dramatically due to fear of COVID-19 transmission within the population.
Most orthopaedic surgeons in Malaysia seemed to continue working during this pandemic, with between 85.2% and 95.5% continuing to manage their semi-urgent and urgent cases in their hospitals, and more than 90% of them still doing on-calls and daily ward rounds. Unfortunately, less than half of those doing their daily routines in the emergency department, wards and clinics are wearing PPEs, either due to reduced awareness or due to supply shortage. The low percentage of those using PPEs while resuscitating patients (38.1%) and in doing elective cases (44.4%) is of main concern as its importance in protecting healthcare workers cannot be overemphasized. 16
More than 90% of elective orthopaedic cases in Malaysia were cancelled or postponed due to this pandemic. This is also in line with recommendations by Correia et al. 17 that stated elective surgical procedures should be postponed to a more appropriate time to (i) provide room/spaces to host more patients; (ii) make available more mechanical ventilators in case of increased demand and (iii) prevent adverse events in patients undergoing expected low morbidity and mortality procedures but that became fatal because of COVID-19 infection in asymptomatic individuals. 17
Screening for COVID-19 status before performing any surgeries, especially those involving aerosol-producing procedures, such as endotracheal intubation and bone reaming and drilling, has been suggested by the local health authority in Malaysia. 8 Unfortunately, not all surgeons performed screening for their patients before performing surgeries. As our survey found out, less than two-thirds performed the more accurate RT-PCR test for their patients, with 20.2% only using symptoms and travel history, which are highly inaccurate, and another 11.2% not doing screening at all. We suggest that the local health authority take appropriate steps to increase awareness on the importance of doing more accurate preoperative and preprocedural screening tests before proceeding with any surgery or procedure.
Finally, with almost two-thirds of respondents reporting reduction of income during this pandemic, more innovative ways to increase patient numbers need to be created. Telehealth modalities should be looked at seriously, and explored extensively, while every effort should be made to protect doctor–patient confidentiality. The surgeons need to be made aware that telehealth will be one of the new norms in the future.
The authors suggest that healthcare authority should take steps to ensure surgeons adhere to updated policies and protocols including preprocedures screening and training on proper use of PPE. Telehealth modalities should be adopted to bring our practice back now and in future.
The limitation of this study may be related to the number of orthopaedic surgeons that can be reached through the available email addresses from the NSR and MOA along with the mobile phone contacts. The exact number of the actively practicing orthopaedic surgeons was also not available, thus, the participation rate could not be clearly determined as well.
Conclusion
Direct exposure to treatment of COVID-19 patients among the respondent is low and the main concern was infecting their family member. There are still several surgeons who did not conduct preoperative COVID-19 screening and practicing without proper PPE training.
Footnotes
Acknowledgements
We would like to thank Ms Uma from Malaysian Orthopaedic Association and Ms Dee Dee from Medical Conference Partners for their assistance in distributing the survey. We would also like to thank Honorary Prof. Dr Sharaf Ibrahim and Prof. Dr Sharifah Roohi Syed Waseem Ahmad for their advice in contacting our respondent. Finally, we would like to express our gratitude to the respondents who took part in this study.
Author contributions
TSH and NMN designed the study. TSH and MRAR designed the questionnaire and collected the data. All authors contributed in analyzing the data, writing, reviewing and approving the final manuscript.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The respondents could decide whether to participate in the study by giving digital informed consent in agreeing to participate in this study.