
Abstract
Background:
Local anesthesia (LA) is widely used in knee arthroscopic surgery but not in ankle arthroscopy.
Objective:
To understand the effectiveness and safety of LA combined with ropivacaine in pain control for ankle arthroscopy.
Study Design:
Retrospective cohort.
Methods:
We retrospectively collected data for patients who underwent ankle arthroscopy from April 2012 to April 2017. Patients were grouped by anesthesia method: LA, LA with ropivacaine (LA+R), spinal anesthesia (SA), and SA with ropivacaine (SA+R). Intra- and postoperative visual analog scale (VAS) scores, complications, doses of supplemental pain medication, hospitalization cost and duration, and satisfaction with pain control during hospitalization were analyzed.
Results:
The study included 276 patients (LA: 93; LA+R: 124; SA: 31; SA+R: 28). The LA and LA+R groups had significantly higher intraoperative VAS scores (LA vs. SA, p = 0.001; LA vs. SA+R, p = 0.002; LA+R vs. SA, p = 0.00; LA+R vs. SA+R, p = 0.00), but fewer complications, than the SA and SA+R groups. The LA+R and SA+R groups had significantly better outcomes for postoperative pain control (LA vs. LA+R, p = 0.01; LA vs. SA+R, p = 0.01; SA vs. SA+R, p = 0.01; SA vs. LA+R, p = 0.03) and required less supplemental pain medication. Hospitalization cost was lower and duration shorter in the LA and LA+R groups than in the SA and SA+R groups. There was no significant difference in satisfaction among the four groups.
Limitations:
This was a single-center retrospective and relatively short-term study.
Conclusions:
LA+R which could be safely applied in ankle arthroscopy provided satisfactory pain control, reduced postoperative pain intensity, fewer complications, shorter hospital stay, and good cost-effectiveness. It can be safely applied in ankle arthroscopy for the specific patients with ankle osteoarthritis.
Introduction
Ankle arthroscopy is a therapeutic procedure for ankle osteoarthritis, chondral lesion, loose body, and soft tissue impingement. 1 –5 It is also performed as a diagnostic procedure for intra-articular disease. 6 For arthroscopic ankle surgery, possible anesthetic methods include spinal anesthesia (SA), nerve block, and local anesthesia (LA). SA is often applied because of its convenience for patients and surgeons, as well as its safety. Moreover, it does not require airway manipulation like general anesthesia dose. Nerve block has been recently applied for ankle surgery which was reported with satisfied pain control. 7 However, both these anesthesia methods have disadvantages compared to LA: they are time-consuming, require multiple procedures, have a longer recovery period, require extensive monitoring, and so on.
LA is a simple and most commonly used anesthesia method in surgery. It was first applied in knee arthroscopic surgery in 1978 8 and today, arthroscopic debridement of the osteoarthritic knee under LA is considered as an appropriate treatment. 9 –11 The advantages of LA include its cost-effectiveness and safety. 12,13 It has faster onset, minimal postoperative emesis, and requires less nursing care postoperatively. LA has also been applied in ankle arthroscopy by some authors. 14,15 However, it is not widely used for this procedure and evidence supporting its application is rare. Many orthopedic surgeons are reluctant to use LA for fear of having to convert to general anesthesia in the event of inadequate pain control. Furthermore, postoperative pain after arthroscopic surgery may affect patient satisfaction with hospitalization.
Postoperative analgesia after arthroscopic surgery affects recovery largely through its critical effect on rehabilitation, postoperative complications, and patient satisfaction. Approximately 60% of patients undergoing knee arthroscopy are reported to experience moderate or severe pain. 16 Ropivacaine, a safe and long-acting regional anesthetic, has been used alone or in combination with other anesthetics for postoperative pain relief following arthroscopic surgery in areas such as the shoulder and knee. 17 –20 However, the effectiveness of ropivacaine for postoperative pain control after ankle arthroscopy needs to be confirmed.
Thus, the goal of the present study was to ascertain whether LA can provide satisfactory pain control during postoperative hospitalization after ankle arthroscopy. To test this, we retrospectively compared satisfaction with pain control during hospitalization, degree of pain control, complications, and hospitalization cost associated with LA and SA. We hypothesized that LA combined with intra-articular ropivacaine would provide patients with the same degree of satisfaction as SA while reducing complication rates and hospitalization costs.
Methods
Patients
This study was approved by the ethics committee of Chinese PLA General Hospital. We identified the medical records of patients with ankle osteoarthritis who underwent arthroscopic surgery in the Sports Medicine Center of Chinese PLA General Hospital from April 2012 to April 2017. Patient data, which were collected prospectively but reviewed retrospectively, included demographics and clinical characteristics, pain intensity, complications, satisfaction, and hospitalization cost. Patients with ankle osteoarthritis requiring debridement, including elimination of fragments of articular cartilage or chondral flaps, biopsy, and/or synovectomy were included. Exclusion criteria were (1) an extremely narrow joint space that prevented the regular surgery procedure, (2) intra-articular fracture, (3) requirement for stabilization via ankle reconstruction, (4) known allergy to bupivacaine or ropivacaine, (5) renal insufficiency, (6) neurologic disorders, (7) coagulation disorders, (8) use of any opioid or sedative medications in the week prior to surgery, and (9) history of alcohol or drug abuse. Before the arthroscopic surgery, the risks and benefits of LA and SA were described to patients, who then provided their written informed consent to undergo the procedure. The standard anesthetic method was LA, but SA was substituted in patients who refused LA or specifically asked for SA. At the end of surgery, patients were randomly assigned to receive ropivacaine intra-articularly and at the incision site. Thus, four treatment groups were considered: LA and no ropivacaine postoperatively (LA), LA plus ropivacaine postoperatively (LA+R), SA and no ropivacaine postoperatively (SA), and SA plus ropivacaine postoperatively (SA+R).
Interventions and outcome measures
In the LA group, 20 mL of 2% lidocaine combined with 40 mL saline and 4 drops of epinephrine hydrochloride was injected intra-articularly and at the site of the incision. In the SA group, SA was performed according to standard procedures with the application of 5 mL of 0.2% bupivacaine. Experienced surgeons performed all arthroscopic surgeries. The operation included trimming areas of meniscal damage and fragments of articular cartilage or chondral flaps, smoothing the bone surface by eliminating osteophytes, synovectomy, and joint lavage. Abrasion or microfracture of chondral defects was performed in patients with a massive cartilaginous lesion. During surgery, if patients experienced pain, they were asked to report their pain level on a visual analog scale (VAS) ranging from 0 to 10 and the maximum VAS score was recorded. General anesthesia was induced when LA proved to be insufficient and the patient’s pain was intolerable.
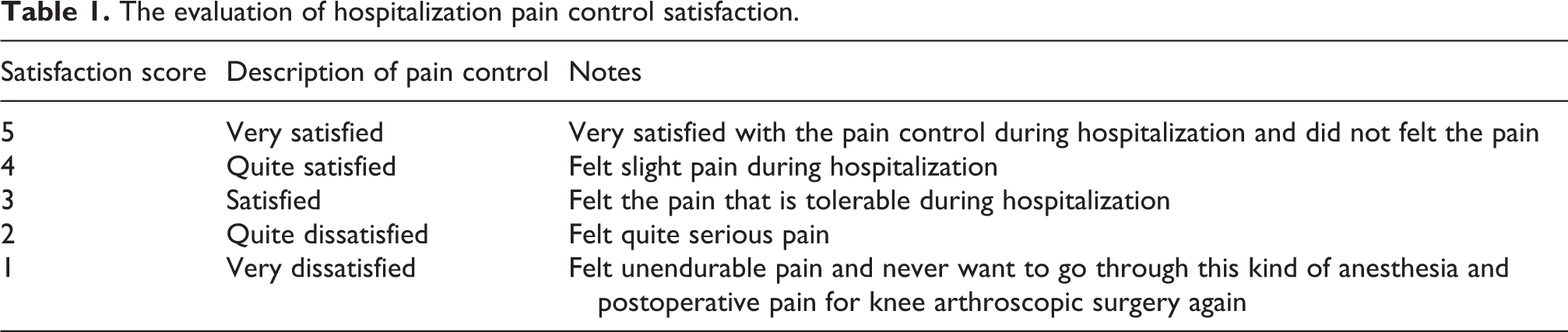
Postoperatively, we recommended patients stay in bed for 6 h before ambulating or using the full range of motion of their affected operated ankle. Nurses recorded VAS scores at postoperative hour 3 for the maximum pain experienced between 0 and 3 h postoperatively, at hour 6 for maximum pain experienced between 3 and 6 h postoperatively, at hour 12 for maximum pain experienced between 6 and 12 h postoperatively, and at hour 24 for maximum pain experienced between 12 and 24 h postoperatively. Supplemental pain medication (intravenous injection of flurbiprofen axetil) was administered to patients whose pain was intolerable, and those patients’ VAS scores were not recorded for that time period. All complications related to anesthesia were recorded. Before being discharged from hospital, patients who had not received supplemental pain medication after surgery completed a questionnaire regarding satisfaction with pain control during hospitalization (Table 1). After discharge, length of hospital stay and total cost of hospitalization were collected from medical records and the hospital database.
The evaluation of hospitalization pain control satisfaction.
Statistical analysis
Data analysis was performed with SPSS Statistics for Windows, Version 17.0 (SPSS Inc., Chicago, Illinois, USA). Baseline characteristics were analyzed using descriptive statistics. VAS scores during surgery and at 3, 6, 12, and 24 h after surgery were compared among groups using analysis of covariance. Comparisons between groups were performed using the Mann–Whitney U test since data were not normally distributed. A two-sided p value of <0.05 was considered statistically significant. All analyses were performed according to the intention-to-treat principle. Missing values were imputed using the principle of last case carried forward. All statistical analyses were performed by a statistician.
Results
Complete data were collected for 276 patients (LA, n = 93; LA+R, n = 124; SA, n = 31; SA+R, n = 28; Figure 1). No significant differences in age, height, weight, body mass index, or preoperative American Academy of Orthopaedic Surgeons® score were present among the four groups (Table 2). The types of procedures performed were comparable for all four groups.

The flowchart of participants through this retrospective study.
Basic characteristics of patients involved in the study.

BMI: body mass index; ASA: American Society of Anesthesiologists; LA: local anesthesia; LA+R: local anesthesia combined with ropivacaine; SA: spinal anesthesia; SA+R: spinal anesthesia combined with ropivacaine.
Intraoperative pain control
Figure 2 shows the VAS scores for the four groups. The VAS scores of the LA and LA+R groups were significantly higher than those of the SA and SA+R groups (LA vs. SA, p = 0.001; LA vs. SA+R, p = 0.002; LA+R vs. SA, p = 0.00; LA+R vs. SA+R, p = 0.00). There was no significant difference in VAS score between the LA and LA+R groups or between the SA and SA+R groups. The most severe pain reported occurred during plasma radiofrequency ablation of subchondral bone; almost no pain was felt during other procedures. In no case was conversion to general anesthesia necessary.

The VAS score between LA, LA+R, SA, and SA+R groups during arthroscopic surgery. *There remains statistical difference between SA, SA+R and LA, LA+R groups while no difference were found between SA and SA+R or LA and LA+R. VAS: visual analog scale; LA: local anesthesia; LA+R: local anesthesia combined with ropivacaine; SA: spinal anesthesia; SA+R: spinal anesthesia combined with ropivacaine.
Postoperative pain control
The highest VAS score was reported for the period between 6 and 12 h after surgery (the 12-h time point) in all groups (Figure 3). LA and SA patients who received ropivacaine had significantly lower VAS scores at the 6-h time point (LA vs. LA+R, p = 0.01; LA vs. SA+R, p = 0.01; SA vs. SA+R, p = 0.01; SA vs. LA+R, p = 0.03). However, although the VAS scores of the LA+R and SA +R groups were significantly lower than those of the other two groups, the VAS scores of the LA+R and SA+R groups did not differ significantly from each other (p = 0.36) at the 6-h time point (3–6 h postoperatively). For all other postoperative time periods, no meaningful differences occurred among groups, although the LA+R and SA+R groups had lower VAS score at the 12-h time point (between 6 and 12 h postoperatively).

The VAS score of four groups at each postoperative time periods. *The difference between LA+R versus LA, LA+R versus SA groups was statistically significant, p = 0.01, 0.03, during 3–6 h after the surgery. &The difference between SA+R versus LA, SA+R versus SA groups was statistically significant, p = 0.01, 0.01, during 3–6 h after the surgery. There remains no statistical difference between each group during other time periods. VAS: visual analog scale; LA: local anesthesia; LA+R: local anesthesia combined with ropivacaine; SA: spinal anesthesia; SA+R: spinal anesthesia combined with ropivacaine.
Postoperative complications and supplemental pain control
Twenty-two patients had complications, including headache, vomiting, nausea, urinary retention, and back discomfort (Table 3). Two patients experienced nausea and headache simultaneously. Significantly fewer complications occurred in the LA group compared to the SA group. No patient experienced neurologic complications.
The postoperative complications of two groups.

LA: local anesthesia; LA+R: local anesthesia combined with ropivacaine; SA: spinal anesthesia; SA+R: spinal anesthesia combined with ropivacaine.
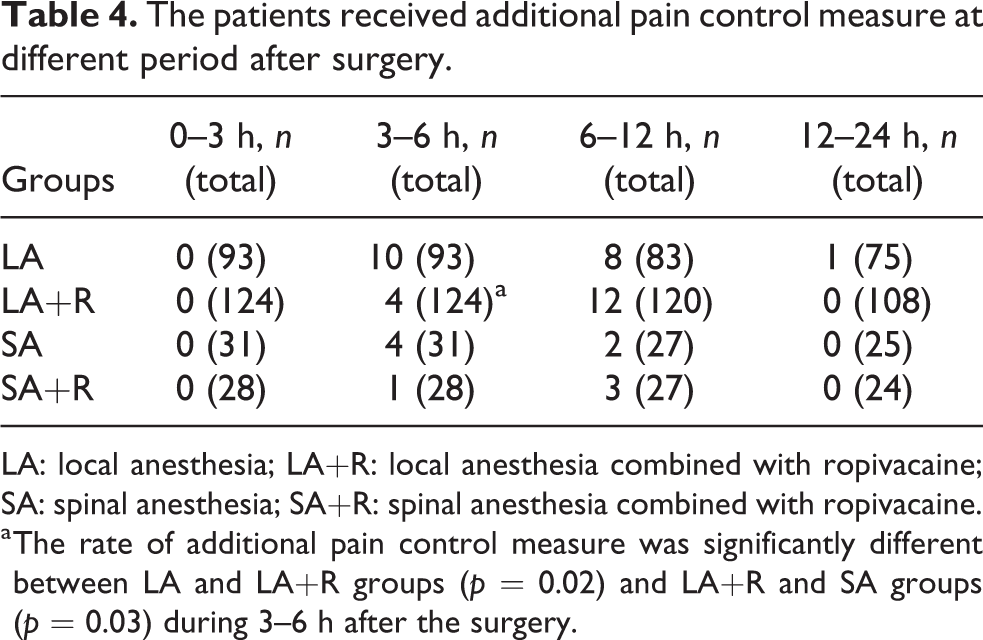
Supplemental pain control medication with intravenous injection of flurbiprofen axetil was administered to patients in all four treatment groups: 19 of 93 patients in the LA group, 16 of 124 patients in the LA+R group, 6 of 31 in the SA group, and 4 of 28 patients in the SA+R group (Table 4). The addition of ropivacaine decreased the requirement for supplemental flurbiprofen 3–6 h postoperatively.
The patients received additional pain control measure at different period after surgery.
LA: local anesthesia; LA+R: local anesthesia combined with ropivacaine; SA: spinal anesthesia; SA+R: spinal anesthesia combined with ropivacaine.
a The rate of additional pain control measure was significantly different between LA and LA+R groups (p = 0.02) and LA+R and SA groups (p = 0.03) during 3–6 h after the surgery.
Hospitalization pain control satisfaction, cost, and period
Figure 4 shows the scores for satisfaction with pain control in the four groups. The SA+R group had the highest score in satisfaction with hospitalization, but no significant difference in satisfaction scores among the four groups occurred. Although the SA and SA+R groups experienced less pain during surgery, overall satisfaction did not differ among the four groups.

The pain control satisfaction of hospitalization for the patients accepted ankle arthroscopy in four groups. There remains no statistical difference between four groups even LA+R and SA+R groups came with the higher score compared with other two groups.
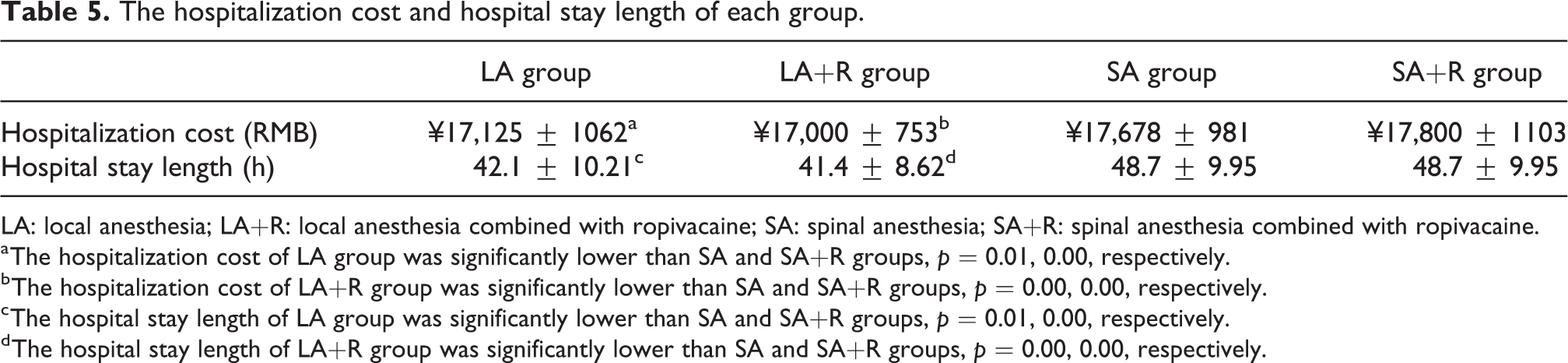
Hospitalization cost for the four groups are shown in Table 5. Costs in the SA and SA+R groups were significantly higher than those in the LA and LA+R groups, but there was no significant difference in cost between the SA and SA+R groups (p = 0.08) or between the LA and LA+R groups (p = 0.07). Hospital stays were significantly longer for the SA and SA+R groups than for the LA and LA+R groups (Table 5), but there was no difference in length of hospital stay between the SA and SA+R groups (p = 0.06) or between the LA and LA+R groups (p = 0.07).
The hospitalization cost and hospital stay length of each group.
LA: local anesthesia; LA+R: local anesthesia combined with ropivacaine; SA: spinal anesthesia; SA+R: spinal anesthesia combined with ropivacaine.
a The hospitalization cost of LA group was significantly lower than SA and SA+R groups, p = 0.01, 0.00, respectively.
b The hospitalization cost of LA+R group was significantly lower than SA and SA+R groups, p = 0.00, 0.00, respectively.
c The hospital stay length of LA group was significantly lower than SA and SA+R groups, p = 0.01, 0.00, respectively.
d The hospital stay length of LA+R group was significantly lower than SA and SA+R groups, p = 0.00, 0.00, respectively.
Discussion
The present study sought to assess whether LA is safe enough to be applied in ankle arthroscopy. Our results show that LA+R can provide satisfactory pain control during and after the surgery and has the advantage of fewer complications, shorter hospitalization, and increased cost-effectiveness. As far as we know, this is the first study on the effectiveness of LA and LA+R for ankle arthroscopic surgery.
Three aspects influence the choice of anesthesia for a specific surgical procedure: patient safety, patient (and surgeon) satisfaction, and cost. 21 Many orthopedic surgeons are reluctant to use LA for arthroscopy for fear of inadequate pain control during surgery. 22 However, SA also has disadvantages, including potential hemodynamic disturbances, lack of suitability for psychologically disturbed patients, inability to last for the duration of prolonged surgery, and potential failure of the spinal block. Complications associated with SA are total spinal or high SA, post-dural puncture headache (PDPH), urinary retention, and waist and back pain. In the present study, we observed that the level of pain during surgery was greater in LA and LA+R groups than the SA and SA+R groups.
According to the feedback of patients intraoperatively, and because none of the procedures in the LA group required conversion to general anesthesia, we concluded that this higher pain level was acceptable and did not affect patient satisfaction.
Intra-articular anesthetic injection or pain medication such as morphine has been administered to control postoperative pain. Ropivacaine is a long-lasting and less toxic anesthetic that has been widely used, separately or in combination, for arthroscopic surgery. The results of the present study show that compared with the LA and SA groups, the LA+R and SA+R groups had a lower mean VAS score during the 3- to 6-h, 6- to 12-h, and 12- to 24-h periods after operation, but only the VAS score during the 6- to 12-h period was significantly better.
For postoperative pain release, significantly fewer patients in the LA+R and SA+R groups required supplemental pain medication with flurbiprofen axetil when compared with the LA and SA groups. Furthermore, the mean VAS score in the postoperative period was significantly lower in the LA+R group, suggesting that LA+R can provide better postoperative pain relief than LA and SA. In addition, compared with the SA+R group, the LA+R group suffered fewer postoperative complications. Zhou et al. 23 reported that single-dose intra-articular ropivacaine administered at the end of arthroscopic knee surgery provided effective pain relief in the immediate and early postoperative periods without increasing short-term side effects. Our study on pain relief for ankle arthroscopic surgery is consistent with results from knee surgery. Our results indicate that intra-articular injection of ropivacaine 5 mL can provide substantial pain relief in the 3–6 h after surgery and decreases the requirement for supplemental pain control after the ankle arthroscopic procedure.
Patients in the LA groups (LA and LA+R group) than in the SA groups (SA and SA+R group) had significantly fewer complications. Previous studies have reported that lidocaine and ropivacaine have chondrotoxic effects, but the effect appeared to be dose-dependent, meaning that a low-dose intra-articular injection could be the least harmful. 24 Piper et al. suggested that there is a greater risk for chondrolysis with longer exposures to higher concentrations of local anesthetics, such as with a pain pump, than with single bolus injections. 25 In a retrospective study, Ravnihar et al. 26 demonstrated that a single intra-articular injection of lidocaine hydrochloride in knee arthroscopy did not influence the viability, morphology, or cultivation potential of chondrocytes. Furthermore, a single-dose intra-articular injection of ropivacaine appears to be less toxic than other frequently used local anesthetic agents. 27,28 For the long-term retrospective recheck of the present study (results not shown), no toxic effects of ropivacaine have been observed, suggesting a single intra-articular ropivacaine injection is safe.
In the present study, although the SA and SA+R groups experienced more side effects than the LA and LA+R groups, overall satisfaction did not differ among groups. Systemic reactions related to LA are extremely rare, 26,29,30 and there are currently no reports on possible intra-articular complications after arthroscopy with LA. Our finding of no complications, either intra-articular or systemic, in patients in the LA group is consistent with previous reports. 31 –33 In patients receiving SA, complications observed were PDPH, back pain, and urinary retention. Thus, with respect to complications, LA and LA+R had a clear benefit over SA and SA+R.
The LA and LA+R groups demonstrated better cost-effectiveness and shorter hospitalization than the SA and SA+R groups in the present study. Previous literature indicates LA can provide shortened recovery time and improved cost-effectiveness for knee arthroscopy. 22,34 It has also been reported that the postoperative stay after knee arthroscopy was significantly shorter in subjects receiving LA compared to those receiving general anesthesia. We found the same trend for the ankle arthroscopy patients in the present study.
Note that we excluded patients with many osteophytes at the posterior talus; because the injection was performed at the front of the ankle, we felt that LA was unlikely to provide sufficient pain relief at those areas. We recommend the application of SA for such patients. We suggest that LA can be applied for eliminating osteophytes, synovectomy, trimming the fragments of articular cartilage or chondral flaps, and so on and it is not recommended for ligament reconstruction. Although this criterion may partly limit the general conclusions of the present study, our study nonetheless indicates that the application of LA and LA+RA can provide satisfactory anesthesia and postoperative pain control while also being more cost-effectives and reducing hospitalization time.
Limitations
The present study had several limitations. First, this was a single-center retrospective study, which is less persuasive than a multi-center randomized controlled trial. In addition, the specific surgical procedure may differ among surgeons, which could affect both the effectiveness of arthroscopy and the VAS score. In addition, the maximum VAS score was used to represent postoperative pain, which may overestimate the VAS score during and after the surgery. A larger study group can provide a more persuasive result. Finally, although current opinion holds that ropivacaine is harmless in the long-term, further studies are required to rule out any chondrotoxic effects.
Conclusions
The present study demonstrates that LA combined with intra-articular injection of ropivacaine for ankle arthroscopy provides satisfactory pain control during hospitalization. It performed well in terms of postoperative pain control, few complications, minimized hospitalization period, and good cost-effectiveness. It is a promising option for patients undergoing ankle arthroscopy surgery.
Footnotes
Authors’ note
MA and XS contributed equally to this work and should be considered as co-first authors. WQ and CL also contributed equally to this work and should be considered as co-corresponding authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research authorship, and/or publication of this article: This work was supported by Beijing Municipal Science and Technology Commission(Beijing Nova Program, grant number: Z181100006218058 and Beijing Municipal Natural Science Foundation, grant number: 7192195).