
Abstract
This report describes clinical and radiographic characteristics of two pediatric patients with a presumptive diagnosis of subchondral fracture of the femoral head made based on their clinical course and imaging findings. An 8-year-old boy and an 8-year-old girl had subchondral fracture in the femoral head without osteonecrosis, which was verified by contrast-enhanced magnetic resonance imaging. Although complete disappearance of the fracture line was confirmed in the boy, the girl had a residual femoral head deformity after conservative treatment. Subchondral fracture of the femoral head should be included in the differential diagnosis of pediatric hip pain.
Keywords
Introduction
Subchondral fracture of the femoral head is commonly observed in elderly patients with osteopenia. They can cause acute hip pain and resultant osteoarthritic changes in the affected hip joint. 1,2 Several reports have emphasized that subchondral fracture should be differentiated from osteonecrosis of the femoral head, since these two conditions might have similar clinical and radiological features, such as acute onset and femoral head collapse. 3,4 Unlike osteonecrosis of the femoral head, which is an incurable condition, subchondral fracture of the femoral head can be treated with appropriate conservative therapy if the fracture is detected in an early phase without severe femoral head collapse. 5,6
Recent studies have demonstrated that subchondral fracture of the femoral head occasionally affects young patients in states of bone insufficiency or as a result of fatigue type fracture. 7 –9 However, there have been no published reports of such fracture in children. We herein describe two pediatric patients in whom a diagnosis of subchondral fracture of the femoral head was made on the basis of clinical and radiological findings. We discuss this condition as part of the differential diagnosis for pediatric hip pain.
Case reports
Case 1
An 8-year-old boy (height: 122 cm, weight: 21 kg) complained of right groin pain and began limping 1 day after participating in nonprofessional athletic activities for a school sports day event, including running, jumping, and gymnastics. He presented with these symptoms 7 weeks after the onset and was referred to our pediatric medical center because Legg–Calvé–Perthes disease was suspected at another hospital. He had a history of left lower extremity pain and limping at age 2, but symptoms resolved within 2 weeks without any treatment. He did not have any history of fracture in the past. The range of hip motion was 110°/140° (right/left) flexion, 10°/20° extension, 20°/45° internal rotation, 45°/45° external rotation, and 20°/30° abduction. The bone mineral density measured by dual-energy X-ray absorptiometry using an X-ray of his both hands indicated a similar value with an average of the same age boys (Z-score −0.3).
Hip joint X-rays taken 8 weeks after pain onset did not show any signs of femoral head collapse, but a slight sclerotic change was observed in the right femoral head (Figure 1(a)). T1-weighted and T2-weighted magnetic resonance (MR) images detected a short, irregular, discontinuous, low-intensity band in the superior portion of the right femoral head that was convex to the articular surface and parallel to the subchondral bone endplate (Figure 1(b)). However, no reduction in blood flow to the right femoral head was demonstrated with gadolinium-enhanced fat-saturated contrast-enhanced MR imaging, which did not support a diagnosis of Legg–Calvé–Perthes disease (Figure 1(c)). Computed tomography (CT) confirmed a linear sclerotic change in the right femoral head corresponding to the low-intensity band in MR images (Figure 1(d)). An axial plane of magnetic resonance imaging (MRI) at the most proximal level of the acetabulum showed bilateral acetabular retroversion (Figure 1(e)). Since he was suspected to have a subchondral fracture of the femoral head or unusual Legg–Calvé–Perthes disease on the right side, conservative treatment consisting of nonweight-bearing with crutches was carried out. At 12 weeks after pain onset, his symptoms resolved and the range of motion of both hip joints normalized. Weight-bearing was initiated. Follow-up X-rays showed the small sclerotic change in the right femoral head corresponding to the lesion detected on CT but no femoral head collapse. Follow-up imaging taken at 7 months after pain onset demonstrated complete disappearance of the low-intensity band on MR images and the corresponding sclerotic change on X-ray and CT (Figure 2(a) to (c)). We confirmed that his subchondral fracture of the femoral head was healed with conservative treatment and there was no residual femoral head deformity. One year after pain onset, he maintained no symptom and no restriction for sports activities.
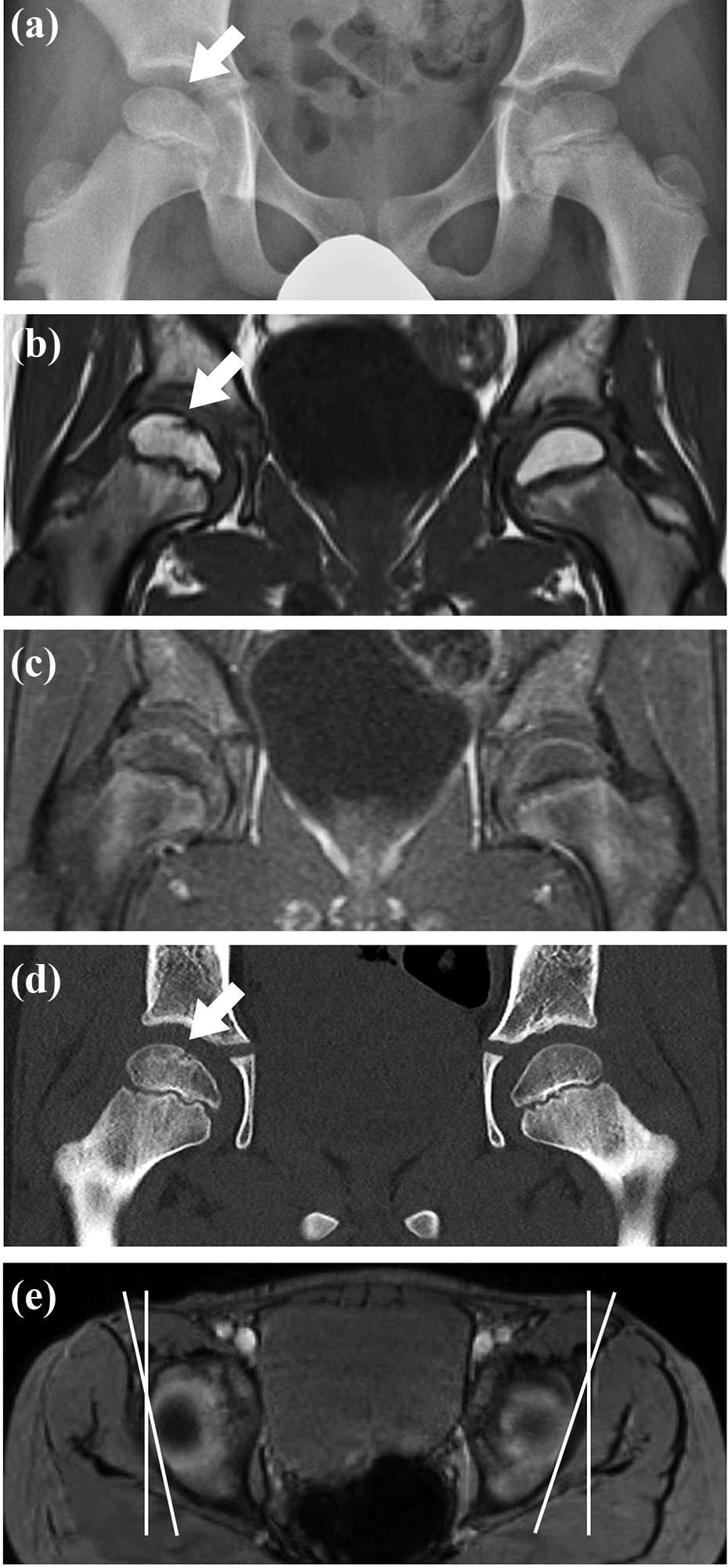
Imaging from an 8-year-old boy with subchondral fracture of the right femoral head (case 1) at the first visit. (a) Anteroposterior X-ray of both hip joints shows a small linear sclerotic change in the right femoral head (arrow), but no obvious femoral head collapse. (b) Coronal T1-weighted (TR/TE, 500/9.8) MR image of both hip joints shows a sharp, irregular, discontinuous, low-intensity band in the superior portion of the right femoral head (arrow), which is convex to the articular surface and parallel to the subchondral bone endplate. (c) Coronal contrast-enhanced fat-saturated T1-weighted (TR/TE, 620/11) spin-echo image of both hip joints demonstrates no reduction of blood flow to the right femoral head. (d) Coronal CT image of both hip joints shows a liner sclerotic change in the right femoral head (arrow) corresponding to the low-intensity band in MR images. (e) Axial multiecho data image combination image (TR/TE, 33/19) at the most proximal level of the acetabulum demonstrates bilateral acetabular retroversion. CT: computed tomography; MR: magnetic resonance; TE: echo time; TR: repetition time.

Images from case 1 at 1 year after the first visit. (a) Anteroposterior X-ray does not show femoral head collapse nor sclerotic change in the femoral head bilaterally. (b) No low-intensity band is observed on the coronal T1-weighted (TR/TE, 500/9.8) MR image in contrast to image from the first visit. (c) No liner sclerotic change in the right femoral head is observed on CT images in contrast to images from the first visit. CT: computed tomography; MR: magnetic resonance.
Case 2
An 8-year-old girl (height: 128 cm, weight: 27 kg) experienced a left femoral neck fracture due to a car accident 9 months before her visit to our pediatric medical center (Figure 3(a)). Before the accident, she had not experienced any fracture. On the day of the injury, she underwent internal fixation with three cannulated cancellous screws at another hospital. Nonweight-bearing period for 3 months following the surgery achieved bone healing at the fracture site, and coxa magna and local osteopenia were confirmed in the left hip without any deformity nor focal sclerosis in the femoral head (Figure 3(b)). Four months after the injury, full weight-bearing was initiated. Another 5 months later, she was suspected of having osteonecrosis of the left femoral head and referred to our center. She complained of mild left hip pain when she visited our center. The hip joint range of motion was 140°/140° flexion, 10°/10° extension, 50°/30° internal rotation, 60°/60° external rotation, and 30°/30° abduction.

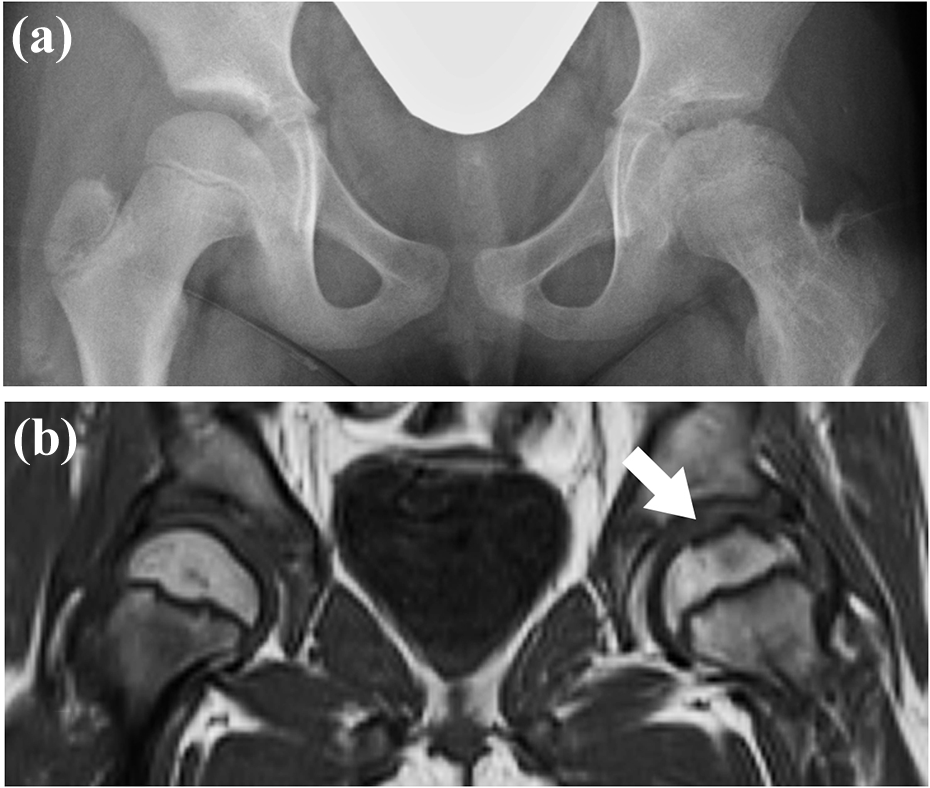
Images from an 8-year-old girl with subchondral fracture of the left femoral head following left femoral neck fracture (case 2). (a) The 3D CT image of the pelvis shows left femoral neck fracture. (b) Anteroposterior X-ray of both hip joints at 3 months after the surgery shows bone healing of femoral neck fracture, transtrochanteric internal fixation screws, coxa magna, and local osteopenia in the left hip without any deformity nor focal sclerosis in the femoral head. (c) Anteroposterior X-ray of both hip joints at 9 months after the surgery shows mild femoral head collapse in the anterosuperior portion (arrow), relatively insufficient acetabular coverage. (d) Coronal T1-weighted (TR/TE, 671/11) MR image of both hip joints showed a long, irregular, discontinuous, low-intensity band in the subchondral area of the left femoral head (arrow), and bone marrow edema patterns in the femoral head and neck. (e) Coronal contrast-enhanced fat-saturated T1-weighted (TR/TE, 615/101) spin-echo image demonstrated a maintained blood flow to the left femoral head, which did not suggest osteonecrosis of the femoral head. Cartilaginous coxa magna is observed in the left femoral head. CT: computed tomography; MR: magnetic resonance.
An X-ray of the hip joints taken at the first visit showed mild femoral head collapse in the anterosuperior portion, relatively insufficient acetabular coverage due to coxa magna and transtrochanteric internal fixation screws in the left hip joint (Figure 3(c)). T1-weighted and T2-weighted MR images detected a long, irregular, discontinuous, low-intensity band in the subchondral area of the left femoral head and bone marrow edema patterns in the femoral head and neck (Figure 3(d)). However, blood flow to the left femoral head demonstrated by gadolinium injection was well maintained, which did not suggest post-traumatic osteonecrosis of the femoral head (Figure 3(e)). Cartilaginous coxa magna were also confirmed. Those radiological findings indicated that a subchondral fracture caused collapse of the left femoral head without femoral head ischemia. Since she had demonstrated femoral head collapse, screw removal and conservative treatment with a nonweight-bearing abduction brace were used. One year later, partial weight-bearing was initiated. Follow-up imaging at 1 year after the first visit demonstrated remodeling of the fracture area but residual femoral head deformity in the anterosuperior portion and coxa magna (Figure 4(a)). MR images still demonstrated the residual low-intensity band (Figure 4(b)). At this time, she had no hip pain and the range of motion was improved, but there was still residual femoral head deformity.
Images from case 2 at 1 year after the first visit. (a) Anteroposterior X-ray shows a remodeling of the fracture area but residual femoral head deformity in the anterosuperior portion as well as coxa magna. (b) A residual low-intensity band (arrow) is observed in the left femoral head in coronal T1-weighted (TR/TE, 670/11) MR images. MR: magnetic resonance.
Discussion
Subchondral fracture of the femoral head is one of the important differential diagnoses of acute hip pain in elderly patients with osteoporosis because it may result in destructive degeneration of the hip joint requiring surgical reconstruction. 2 –4 Recently, it has been recognized to be associated with not only systemic osteoporosis but also local osteopenia of the hip joint, as well as activity fatigue type of fracture, even in young patients. 7 –10 We demonstrated that pediatric patients could have this type of fracture, in which detailed radiological findings had not been reported. These patients were diagnosed based on radiological evidence of a fracture line in living bone confirmed with contrast-enhanced MR images and clinical evidence of a fracture healing process.
Subchondral fracture of the femoral head in children has to be differentiated from Legg–Calvé–Perthes disease, post-traumatic osteonecrosis, and dysplasia epiphysealis capitis femoris, including Meyer dysplasia. Legg–Calvé–Perthes disease is a juvenile form of ischemic femoral head osteonecrosis that causes femoral head collapse and possibly permanent femoral head deformity. 11,12 Since the healing process against ischemia-induced necrotic bone in Legg–Calvé–Perthes disease and post-traumatic osteonecrosis takes several years, appropriate long-term therapy required. 13,14 MR imaging is useful for early detection of the disease. In particular, contrast enhancement with gadolinium provides precise information about the size of the ischemic area in the femoral epiphysis. 15,16 The patients in the present report demonstrated no reduction in contrast enhancement in the whole femoral head, which is an obvious difference from findings in patients with Legg–Calvé–Perthes disease or post-traumatic osteonecrosis (Figure 5). Furthermore, complete disappearance of the fracture line within several months, as in case 1, is not observed in Legg–Calvé–Perthes disease.
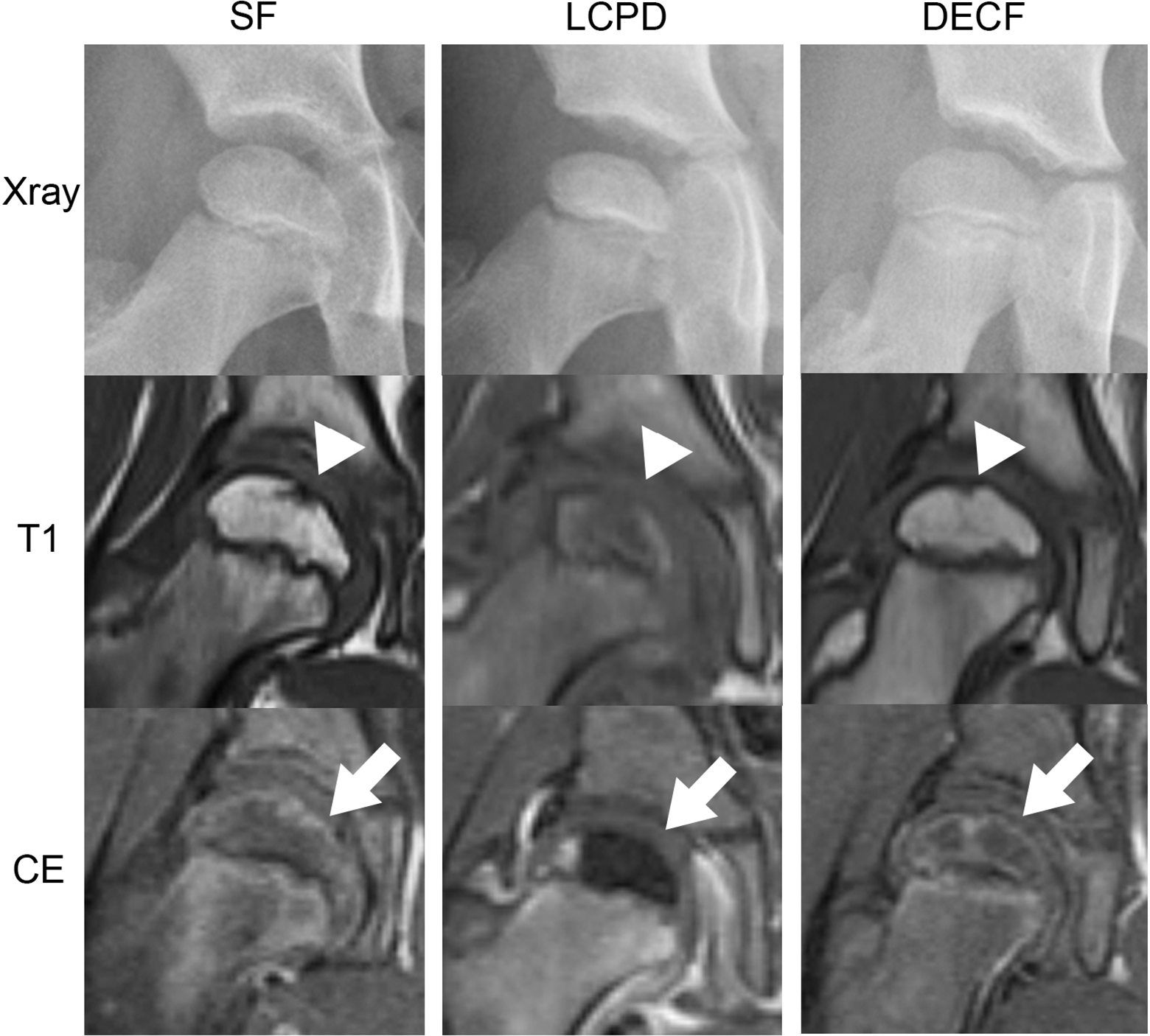
Comparisons of radiological findings among children with subchondral fracture of the femoral head (SF), LCPD and DECF. T1: T1-weighted MRI, CE: contrast-enhanced MRI SF patient shows a small linear sclerotic change in X-ray, a sharp low-intensity band (arrowhead) indicating the fracture line in T1-weighted MRI, and a well-maintained blood flow in the whole femoral head (arrow) in contrast-enhanced MRI. LCPD patient in the early stage shows an increased radiodensity in the femoral epiphysis in X-ray, an indistinct low-intensity area in the femoral epiphysis (arrowhead) in T1-weighted MRI, and a well-demarcated signal defect indicating ischemic area in the femoral epiphysis (arrow) in contrast-enhanced MRI. DECF patient shows a small pit in the top of femoral epiphysis in X-ray, a small low-intensity pit (arrowhead) without bone marrow edema changes, and no decreased blood flow around the hip joint (arrow). MRI: magnetic resonance imaging; DECF: dysplasia epiphysealis capitis femoris; LCPD: Legg–Calvé–Perthes disease.
On the other hand, dysplasia epiphysealis capitis femoris including Meyer dysplasia, which shows a delayed ossification center of femoral epiphysis, is thought to be one of asymptomatic normal variants shown during the development of the femoral head in children under 4 years of age. 17 –19 It has a course of spontaneous disappearance within several years without any treatment. 19 Our two patients were both 8 years old and complained of hip pain and reduced hip range of motion. In addition, radiological abnormalities disappeared within several months. These clinical characteristics are different from those of dysplasia epiphysealis capitis femoris. Although MR imaging findings in dysplasia epiphysealis capitis femoris have not been well characterized, clinical and radiological characteristics of patients in the present report are unlikely to indicate it.
Although the precise mechanism of subchondral fracture of the femoral head has still been unclear, systemic and local osteopenia are known to be significant risk factors. 7 –9 Recently, pelvic anatomical abnormalities, such as acetabular retroversion and asphericity of femoral head–neck junction, were also reported to be associated with patients with this condition. 20 Case 1 in the present report had bilateral acetabular retroversion, while case 2 demonstrated local osteopenia in the left hip due to a long-term nonweight-bearing in addition to coxa magna. Those characteristics might have been related to producing a focal abnormal stress to the femoral head.
Our pediatric patients with subchondral fracture of the femoral head had different prognoses: complete healing or residual femoral head deformity. Iwasaki et al. reported that a longer fracture line and insufficient acetabular coverage are poor prognostic factors for the hip joint with subchondral fracture of the femoral head. 6 In the present study, case 2 had a relatively longer fracture line and insufficient acetabular coverage caused by coxa magna after femoral neck fracture, which might be associated with residual femoral head deformity. Joint preserving procedures in young patients with subchondral fracture of the femoral head have achieved more favorable outcomes than in patients with osteonecrosis of the femoral head due to fracture healing in living bone. 21 Surgical intervention transposing the weight-bearing area, such as transtrochanteric varus or rotational osteotomy, might have been appropriate for case 2 in addition to the removal of metal implants. 21,22
There are several limitations in the present study. First, only two cases were reported. Although subchondral fracture of the femoral head may be a relatively rare condition in children, it would be an important part of the differential diagnosis for pediatric hip pain because it is expected to have better prognosis than Legg–Calvé–Perthes disease. Secondary, pathological assessments were not performed in patients because no surgical intervention was performed. If pathological evidence could be obtained in the future, detailed comparisons would be possible among different conditions in the differential diagnosis.
Conclusion
We described subchondral fracture of the femoral head in children, which should be part of the differential diagnosis of pediatric hip pain. A detailed workup by MRI with gadolinium enhancement is essential for its diagnosis and subsequent management.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by JSPS KAKENHI under grant number 19K18534.