
Abstract
Reconstruction of an infected knee joint with a large defect and extensor mechanism deficiency is challenging. In this study, we aim to describe a one-stage reconstruction surgery and provide its surgical outcome. Two patients had patellar open fracture and subsequent septic arthritis; in addition, a large soft tissue defect, loss of patella, and shortening of the patellar tendon were observed. The semitendinosus–gracilis tendon formed a loop to stabilize the patella. A free or supercharged reverse pedicle myocutaneous anterolateral thigh flap with fascial extension is designed to fill the defect and eradicate the infection. Mean clinical follow-up was 18 months. Although some limitation in the knee range of motion was observed, the dynamometer showed only partial loss in peak concentric power and eccentric power. We developed an innovative surgical procedure to alleviate infection and reconstruct a complex knee defect with extensor mechanism deficiency; this procedure resulted in favorable clinical outcomes.
Keywords
Introduction
Treating a complex traumatic knee defect is challenging. For infected knee defects, repeated and extensive debridement is required before reconstruction. A previous study proposed a knee reconstructive algorithm to treat knee defects based on the size of the wound, location of the wound, and presence of active deep infection. 1 Multiple-stage reconstruction is time consuming, and patients undergoing such reconstruction experience great suffering. Currently, one-stage reconstruction followed by early mobilization is preferred and provides favorable outcomes. 2 –4 In this report, we propose a one-stage reconstruction surgical technique to control infection, fill the large defect, and reestablish the extensor mechanism in two cases of traumatic knee osteomyelitis with massive patella bony and tendinous loss through simultaneous reconstruction with semitendinosus–gracilis (STG) tendons and an anterolateral thigh (ALT) flap and provided our objective functional assessment.
Case report
Case 1
A 58-year-old Taiwanese woman presenting a 6 × 8 cm open wound and traumatic complex knee defect in her left knee was transferred to our hospital. Previous wound swab culture indicated Pseudomonas aeruginosa infection. The plain radiograph showed loss of the lower pole of the patella and a comminution fracture of the upper pole. The lower limb angiography confirmed the patency of descending branch of the lateral femoral circumflex artery.
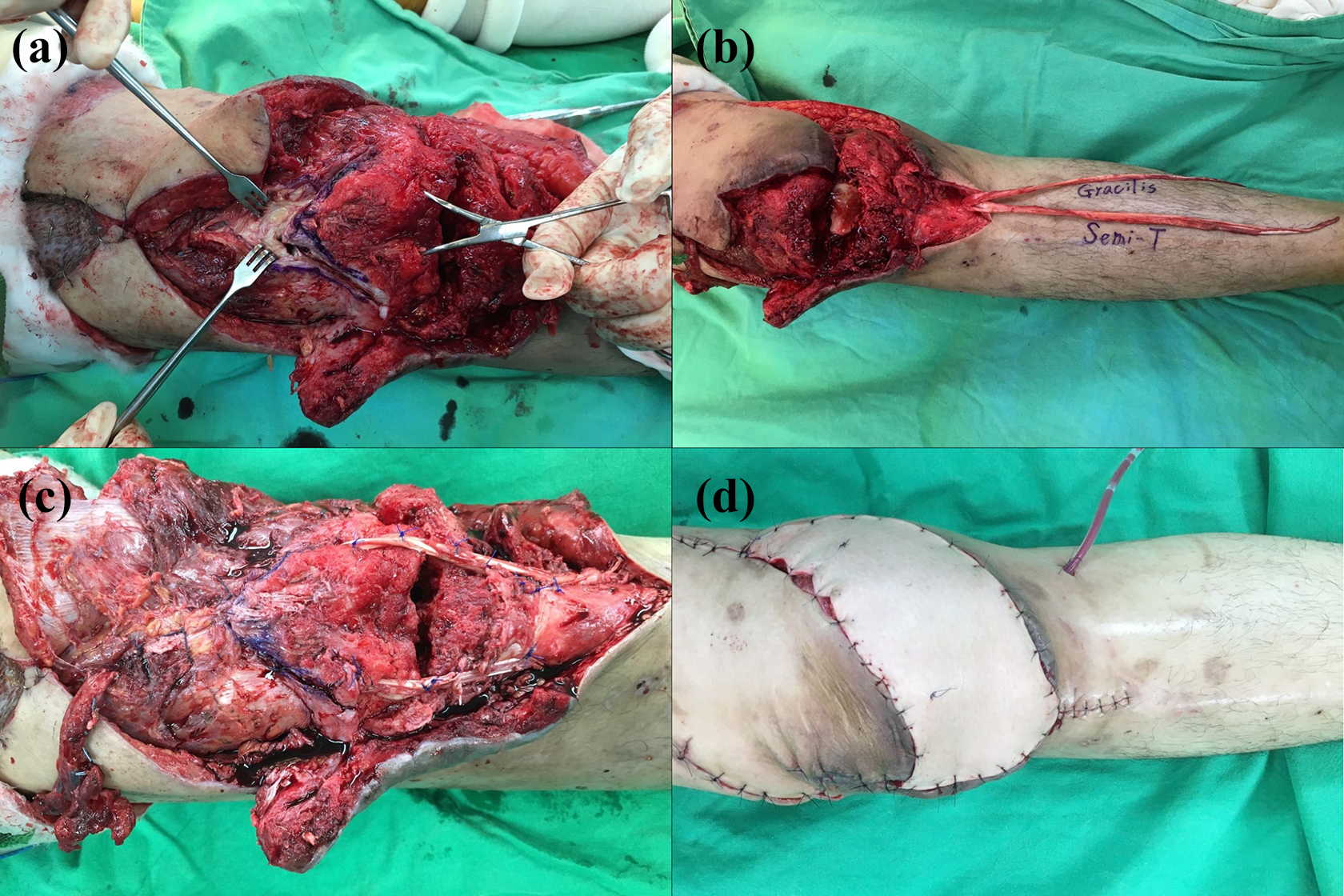
In the first step of our reconstruction surgical technique, her extensor mechanism was reestablished. We performed fixation of the upper pole of the patella by using a 4.5-mm cancellous screw. We harvested the STG tendons and preserved their distal insertions (Figure 1(a)). The free end of the semitendinosus tendon was passed through a tunnel in a medial-to-lateral direction. The free ends of the tendon were brought up proximally to surround the patella remnant and were passed transversely through a tunnel at the junction of the upper pole of the patella and the quadriceps tendon. The gracilis tendon was passed in a medial-to-lateral direction, and the semitendinosus tendon was passed in the opposite direction, and the quadriceps tendon was pulled distally with the knee joint in full extension. Each tendon was tied together with interrupted sutures where they overlapped (Figure 1(b)).

(a) The lower pole of the patella and the patellar tendon were lost, and the residual patella was exposed. We harvested the semitendinosus and gracilis tendons and preserved their distal insertions, and (b) we reconstructed the patellar tendon by suturing the semitendinosus and gracilis tendons in a circular manner. (c) We designed a chimeric supercharged reverse ALT flap with (d) vascularized fascia lata and (e) vastus lateralis to cover the complex soft tissue defect.
In the second step, the knee defect was reconstructed. We designed a supercharged reverse pedicle myocutaneous ALT flap with fascial extension. The pivot point was 10 cm above the knee, and the pedicle of the flap was passed through a subcutaneous tunnel (Figure 1(c)). The flap was transferred to cover the knee defect as a pedicle rotational flap. We filled the knee joint defect with the vastus lateralis (VL) (Figure 1(d)) and the vascularized fascia lata as an augmentation for the knee extensor apparatus (Figure 1(e)).
The patient received 2-week intravenous antibiotic treatment; her infection was fully under controlled, and no pathogen was cultured from the wound.
Case 2
A 40-year-old Taiwanese man transferred to our hospital with a congested 9 × 7 cm propeller flap and 15° knee flexion contracture. The previous wound swab culture indicated P. aeruginosa infection. The plain radiograph showed a comminution fracture of the lower pole of the patella.
After removing the previous local flap and wires and performing debridement, we performed a quadriceps V-Y advancement to resolve this anterior knee fibrosis (Figure 2(a)). Then, we harvested the STG tendon to reestablish the extensor mechanism, as described in case 1 (Figure 2(b) and (c)).
(a) Because of fibrosis of the soft tissue around the knee, we performed a V-Y advanced flap to pull down the distal portion of the quadriceps tendon. (b) Subsequently, we harvested the semitendinosus and gracilis tendons and preserved their distal insertions, and (c) we reconstructed the patellar tendon using the harvested tendons. (d) Finally, to cover the complex defect, we harvested a chimeric supercharged reversed pedicle ALT flap by anastomosing descending branch to the descending genicular artery and concomitant vein combined with the vascularized fascia lata and vastus lateralis.
We designed a 10 × 20 cm rectangular chimeric free flap with the vascularized tensor fascia lata and VL and designed a local rotational flap to cover the lateral skin defect (Figure 2(d)). The infection in the wound subsided after 3-week intravenous antibiotic treatment.
Clinical outcomes
Case 1
At 1-year follow-up, the magnetic resonance imaging (MRI) showed favorable continuity of the reconstructed patellar tendon (Figure 3(a)). She could extend her leg against gravity actively (Figure 4(a)), but her range of motion (ROM) was limited (range 20°–50°). To treat severe knee stiffness, we lengthened the rectus femoris through quadriceps V-Y advancement and performed resection to adequately release scarring and adherent tissues. Intraoperative passive ROM of the knee was 0°–80°. She received postoperative analgesics for pain relief and rehabilitation to maintain the ROM obtained intraoperatively. However, 6 months after open release, the stiff knee still showed deterioration (Figure 3(b) and (c)). Objective functional assessment of the knee joint was performed using a dynamometer (Biodex, USA). The isokinetic test at 120° per second showed 78% deficit in peak concentric extensor power and a 68% deficit in peak eccentric extensor power (Table 1). However, the isometric test at 20° flexion showed a 22% deficit in concentric extensor power.

Magnetic resonance imaging showed favorable continuity of the reconstructed patellar tendon in patient nos 1 (a) and 2 (b).

At 1.5-year follow-up, patient no. 1 could actively extend her leg against gravity (a). However, her knee was stiff (range 0°–20°) (b and c). Patient no. 2 could actively extend his leg against gravity (d). The range of motion of his knee was limited (range 14°–92°) (e and f).
Case 2
At 1.5-year follow-up, the follow-up knee MRI showed favorable continuity of the reconstructed patellar tendon (Figure 3(b)). He could actively extend his knee up to only 14° extension lag and flex up to 92° (Figure 4(d) to (f)). The isokinetic test at 120° per second showed only a 24% deficit in peak concentric extensor power and a 32% deficit in peak eccentric extensor power (Table 1).
Isokinetic dynamometry and ROM of the knees.

Con: concentric; Ecc: eccentric; ROM: range of motion.
Discussion
Treating a complex infected knee defect is challenging. For the massive soft tissue defect around the knee, a review proposed an algorithm for flap reconstruction of the knee. 1 The ALT flap remains the first choice of either pedicle or microsurgical reconstruction to treat a large defect in different regions of lower extremities. When a septic knee and large defect occur simultaneously, a ALT flap along with VL is recommended; it has higher anti-infection ability than does the conventional gastrocnemius (GM) muscle flap; it not only avoids a bulging outcome but also provides relief for flap congestion. 1 Our limited—but successful—clinical experience demonstrates that free flaps can be used to reconstruct infected large knee defects according to the algorithm. Although the pedicle GM flap is an alternative method to reconstruct soft tissue defects and restore the extensor mechanism, 2,4 –6 previous studies have shown that extension insufficiency is commonly observed after reconstruction with the GM flap 6 ; thus, this flap may not be suitable for reconstructing large defects (>6 cm). 1
Previously many surgical techniques have been proposed to reconstruct the extensor mechanism of the knee. 7 –9 A study proposed one-stage ALT with vascularized fascia lata to reconstruct a complex knee defect with a deficiency of the patellar tendon. 3 Although this study revealed favorable functional recovery, the isometric power test at 30° flexion of the quadriceps indicated an 80% deficit. In comparison with our result, reconstructing the patellar tendon with autologous STG tendon was a better choice.
Post-traumatic knee stiffness is a problem. Two patients showed severe knee stiffness when transferring to our hospital. These patients received multiple aggressive debridement procedures and were immobilized for more than 1 month. Persistent quadriceps force to the patella without the opposite force of the patellar tendon and intra-articular fixation cause patella alta. Intra-articular adherent tissue formation and quadriceps fibrosis cause joint stiffness. Thus, we performed resection of intra-articular adherent tissue before the reconstruction procedure. Due to severe intraoperative knee stiffness, we performed additional quadriceps V-Y advancement in patient no. 2 to extend the knee. The patient no. 1 was delayed in rehabilitation and showed persistent knee ROM limitation after 1-year follow-up. Although we have tried another scar tissue resection and joint capsule release, the effect was limited.
During follow-up, both patients recovered from the infected knee and showed favorable soft tissue healing. The plain radiograph showed patella bony union and no patella alta, and MRI showed favorable continuity of the reconstructed patellar tendons. However, the postoperative ROM and muscle power of the two patients varied (Table 1). We have found that patient, who was younger, having more motivation to return to workplace and stuck to the rehabilitation program, had a more favorable functional outcome.
Conclusion
Myocutaneous ALT flap with fascial extension, either locally supercharged reverse pedicle or free and which involves the creation of the ipsilateral vascularized STG tendon loop for patellar tendon reconstruction, is an effective and reliable option for large complex knee joint soft tissue defect with extensor mechanism disruption.
Footnotes
Authors’ note
All contributors meet the criteria for authorship of International Committee of Medical Journal Editors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This research project was analyzed and approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-E(I)-20180023).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.