
Abstract
Purpose:
Iatrogenic radial nerve injury caused by surgical exposure of the humerus is a serious complication. We aimed to describe the course of the radial nerve at the posterior humeral shaft using a three-dimensional (3D) reconstruction technique by utilizing computed tomography (CT) images of living subjects. We hypothesized that the course of the radial nerve in the posterior aspect of the humeral shaft would be reliably established using this technique and the measurements would have satisfactory intraobserver/interobserver reliabilities.
Methods:
This in vivo anatomical study utilized 652 upper extremity CT angiography images from 326 patients. A 3D modeling of the humerus and radial nerve was performed. We evaluated the segment of the radial nerve that lays directly on the posterior aspect of the humeral shaft and measured its proximal point, mid, and distal points. The shortest distances from the olecranon fossa to these points were defined as R1, R2, and R3, respectively. The relationships between these parameters and humeral length (HL) and transcondylar length (TL) were evaluated, and the intraobserver/interobserver reliabilities of these parameters were measured.
Results:
The HL was 293.6 mm, and TL was 58.64 mm on average. The R1 measured 159.2 (range 127.1–198.2) mm, R2 was 136.6 (105.7–182.5), and R3 was 112.8 (76.8–150.0) mm on average (p < .001). The intraobserver/interobserver reliabilities ranged from 0.90 to 0.98.
Conclusion:
The course of the radial nerve at the posterior aspect of the humeral shaft can be reliably established using the 3D reconstruction technique, and all measurements had excellent intraobserver/interobserver reliability.
Introduction
The reported incidence of iatrogenic radial nerve injury during surgical treatment of humeral shaft fractures ranges between 7% and 20% of all radial nerve palsies, and most cases of this complication require surgical treatment. 1 –6 The radial nerve was reported to be in direct contact with the posterior humerus within the spiral groove proximally and tethered by lateral intermuscular septum on the anterior compartment as it extends distally. Little mobility due to this anatomical constraint may lead to an increased risk of nerve injury in the posterior aspect of the humeral shaft when using the posterior approach to treat humeral shaft fractures. 7 –10 Many anatomical studies have sought to define the course of the radial nerve as well as to establish a consistent danger zone of the radial nerve in relation to the various anatomical landmarks of the humerus, such as the deltoid tuberosity, medial/lateral epicondyle, and olecranon fossa. 1,7,9 –15 However, because of the use of cadaveric specimens, the sample size was limited in several studies. 7,8
Ongoing development of three-dimensional (3D) reconstruction technology has extended the application of this technology to orthopedic research. The 3D reconstruction of soft tissues, such as muscles and nerve bundles, using computed tomography (CT) images may offer an enhanced understanding of the relationship of their locations. 16 This technique makes it possible to evaluate the relationship of the nerve to the reference anatomical landmarks by using living subjects without limitation to the number of samples. Therefore, we conducted an in vivo anatomical study to describe the course of the radial nerve at the humeral shaft using a 3D reconstruction technique and CT scan images of living subjects.
The aims of the present study were to (1) evaluate the course of the radial nerve at the posterior aspect of the humeral shaft to avoid iatrogenic injury when using the posterior approach to treat humeral shaft fractures and (2) determine the intraobserver and interobserver reliabilities of the measurements assessed by 3D reconstruction software. We hypothesized that the course of the radial nerve in the posterior aspect of the humeral shaft would be reliably established and the measurements would have satisfactory intraobserver/interobserver reliabilities.
Materials and methods
Study design and population
The study was approved by the institutional review board of our institution. We retrospectively reviewed 329 consecutive patients from August 2016 to November 2017 (658 upper extremity CT angiography images). The patients were selected from a pool of patients who had undergone CT angiography (CTA) in our institution for work-up of cardiovascular disease, trauma, or infection. We excluded patients with any tumors, neurologic deficits of the upper extremity, or pathology causing a substantial alteration to the normal anatomy of the humerus and surrounding soft tissue. Three images showing a history of humeral shaft fractures, 2 images (1 patient) with poor image quality, and 1 image with leakage of contrast medium were excluded. In total, 652 CT images from 326 patients were used in this study. The patients were all from Asian ethnic groups. We evaluated the segment where there was direct contact of the radial nerve with the posterior humeral shaft because this segment is reported as the most frequent area of iatrogenic radial nerve injury when using the posterior approach to treat humeral shaft fractures because of the intimate relationship of the radial nerve with the humeral shaft and less mobility. 7 –9,17,18
Upper extremity CTA
All CTA images were acquired with a 64-detector CT scanner (Brilliance, Philips Medical Systems, NA, Bothell, WA), and the images were obtained in 1-mm sections and saved in Digital Imaging and Communications in Medicine format (Figure 1(a)). Patients were scanned in the supine position with both upper extremities placed over their head, with their palms ventral and fingers extended and straightened. The usual scanning parameters were manual 100 kV, 150–600 SmartmA (0.80-s gantry rotation period), and 80-mm table travel per rotation. Intravenous access was obtained with an 18 or 20-gauge catheter in the antecubital fossa, and 100 mL of a nonionic contrast medium (Iomeron® 400) at a concentration of 370 mg/mL was injected at a rate of 3–4 mL/s, followed by a 40-mL saline flush at the same rate.

A workflow diagram of the 3D model building process. (a) Axial images of upper extremity CTA. (b) CT data are imported into the 3D reconstruction software. (c) Humerus reconstruction. (d) Radial nerve reconstruction. (e) The 3D measurement of the bony structures. (f) The 3D measurement of the location of the radial nerve in relation to the bony structure. 3D: three-dimensional; CT: computed tomography; CTA: computed tomography angiography.
3D reconstruction model building
CT data were imported into the 3D reconstruction software (AVIEW Modeler 1.0; Coreline Soft Inc., Seoul, Republic of Korea). 19 –22 This software can perform automatic segmentation, 3D reconstruction, and measurements. CT images of the humerus and radial nerve were reconstructed into a 3D volume-rendered model (Figure 1(b)).
Humerus reconstruction
The cortical bone was rendered by setting the lower threshold, generally at 225 Hounsfield units (HU), so that all the pixels with a radiodensity greater than this threshold value were selected. Then both humeri (from the glenohumeral joint to the ulnohumeral joint) were isolated from the rest of the bony anatomy of the shoulder girdle and elbow joint by using the region growing technique. Occasionally, pixels bridging the humeral head to the glenoid fossa, olecranon fossa to the olecranon or trochlea to the coronoid process, as well as adjacent soft tissue or noise with radiodensity greater than 225 HU were manually excluded from the region of interest. The cortical bone of the humerus with radiodensity less than 225 HU was manually selected. Three-D rendering with smoothing of the segmented CT slices produced a 3D model of the humerus (Figure 1(c), Supplementary Figures 1 to 3).
Radial nerve reconstruction
In the multiplanar reconstruction platform that simultaneously shows the axial, sagittal, and coronal sections and the 3D reconstructed image, 3D rendering was performed. For the rendering of the radial artery, thresholding (lowest threshold, 184 HU) and the region growing technique were used. 23 As the artery enhanced by the contrast medium has a higher HU and circle-like shape in the axial plane, the region growing process can be performed automatically: when an initial seed point is chosen in the circle, the other points are automatically detected by the circle detection algorithm. 24 Because the radial nerve runs in the same path as the artery in the form of a neurovascular bundle, referencing the enhanced radial collateral artery helps locate the course of the radial nerve. Next, we traced the radial nerve branching from the posterior cord of the brachial plexus. Because the radial nerve had a similar HU to the surrounding soft tissue on the CT image, the automatic process was impossible. Thus, we performed the rendering manually. In each coronal view image, where the radial nerve was seen longitudinally, we reconstructed the trace of the radial nerve to the elbow joint level using a region growing tool and repeated this process for all coronal view images (Figure 1(d)). Reconstruction was performed with consideration of the location where the radial nerve rests in direct contact with the posterior aspect of the humeral shaft.
Measurements of the course of the radial nerve relative to the humerus
After the humeral and radial nerves were reconstructed, the 3D reconstruction software calculated the following five morphological parameters, which were chosen based on the findings of previous studies. 8,14,15,25 regarding the relationship of the radial nerve to the humerus. Humeral length (HL) was defined as the line measuring the distance between the tip of the humeral head to the most prominent point of the trochlea along the longitudinal axis of the humerus. Transcondylar length (TL) was defined as the largest distance between the most prominent points of medial and lateral epicondyles of the distal humerus (Figure 2). Regarding the segment where there was direct contact of the radial nerve with the posterior humeral shaft, we measured its entry point (proximal point), exit point (distal point), and midpoint, and then the shortest distances from the proximal edge of the olecranon fossa to these points were defined as R1, R3, and R2, respectively (Figure 3). These parameters are also expressed as the ratios in relation to HL and TL (R1/HL, R2/HL, and R3/HL and R1/TL, R2/TL, and R3/TL). Two fellowship-trained orthopedic surgeons (C-SM and K-KJ) independently measured these parameters in a randomized order.
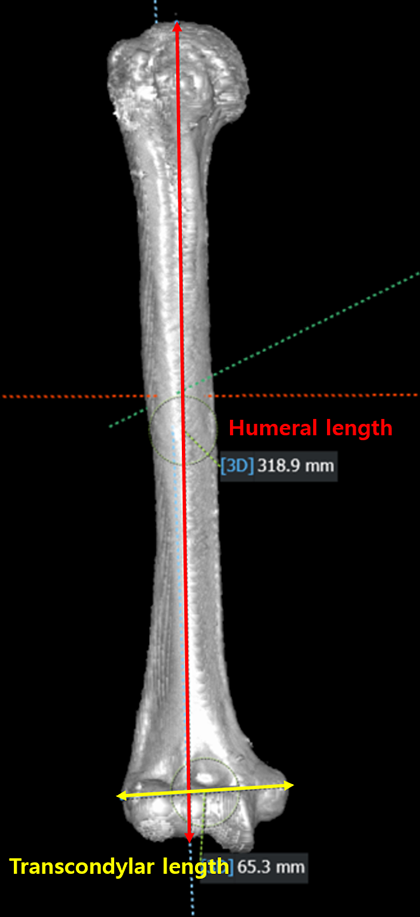
Three-dimensional measurement of the humeral length and transcondylar length.

Measurement of R1, R2, and R3 at the posterior aspect of the left humerus. R1 is the distance of the olecranon fossa to the entry point of the radial nerve at the posterior aspect of the humeral shaft; R2 is the distance of the olecranon fossa to the midpoint of the radial nerve; R3 is the distance of the olecranon fossa to the exit point of the radial nerve.
Statistical analysis
A power analysis was conducted to assess whether the sample size was sufficient to demonstrate the existence of a true difference in R1, R2, and R3. The effect size (D) for the difference was calculated, and the number of patients per parameter required to detect that effect size with 95% power at a 5% significance level was calculated with the use of an analysis of variance (ANOVA) test. The effect size (D) was 1.323, which indicated that a minimum sample size of 15 would be required to detect the significant difference. Therefore, the sample size in our study was adequate to demonstrate that such a difference existed.
Measurements were performed on two separate occasions by two independent investigators in a blinded manner. Each investigator was blinded to the measurements of other investigators and to one’s own previous measurements; each set of measurements was obtained with a minimum interval of 1 month. Interobserver and intraobserver reliabilities were determined by calculating the intraclass correlation coefficients. 26 Descriptive statistics are used to summarize patients’ demographic characteristics.
Data are represented as a mean and 95% confidence interval. A two-sided ANOVA test was performed to evaluate differences of R1, R2, and R3. Paired t test analysis was used to compare differences between two limbs of a pair, and the Student’s t test was used to compare differences between male and female patients with regard to all parameters.
Spearman correlation analysis was used to analyze the correlation of (1) the height of patients with the HL and TL and (2) HL and TL with the R1, R2, R3, and their ratio values, respectively. The values of p < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
Results
The average age of patients was 61.37 years (95% confidence interval (CI) 60.2–62.6). There were 158 (48%) female and 168 (52%) male patients. The height was measured at 161.4 cm on average (95% CI 160.5–162.3 cm). The intraobserver and interobserver reliabilities indicated high reliability for each method between the investigators (Table 1).
Intraclass correlation coefficients for intraobserver/interobserver reliabilities of each observer.

R1: the distance of the olecranon fossa to the entry point of the radial nerve at the posterior aspect of the humeral shaft; R2: the distance of the olecranon fossa to the midpoint of the radial nerve; R3: the distance of the olecranon fossa to the exit point of the radial nerve; CI: confidence interval.
The HL was 293.6 mm (95% CI 292.1–295.1 mm) on average, and the TL was 58.64 mm (95% CI 58.2–59.0 mm) on average. On average, R1 was 159.2 mm (95% CI 157.9–160.4; range 127.1–198.2 mm), midpoint (R2) was 136.6 mm (95% CI 135.6–137.7; range 105.7–182.5 mm), and exit point (R3) was 112.8 mm (95% CI 111.8–113.8; range 76.8–150.0 mm). These parameters showed significant differences between each other (all p < 0.001). The mean R1/HL ratio was 0.54 (95% CI 0.54–0.54; range 0.44–0.63), mean R2/HL ratio was 0.47 (95% CI 0.46–0.47; range 0.39–0.56), and mean R3/HL ratio was 0.38 (95% CI 0.38–0.39; range 0.29–0.47). The average R1/TL ratio was 2.72 (95% CI 2.70–2.74), and it ranged from 2.18 to 3.32. The average R2/TL ratio was 2.34 (95% CI 2.32–2.36), and it ranged from 1.83 to 2.98. The mean R3/TL ratio was 1.93 (95% CI 1.91–1.95; range 1.40–2.57). We could not find any statistically significant differences between the two limbs of a pair with regard to all parameters (Supplementary Table 1).
In the correlation analysis, the height of patients showed a significant correlation with the HL, TL, R1, R2, and R3 (r = 0.87, 0.74, 0.64, 0.56, and 0.36, respectively; all p < 0.001). The HL had a significant correlation with R1, R2, and R3 (r = 0.68, 0.63, and 0.45, respectively, all p < 0.001), and the TL correlated with R1, R2, and R3 (r = 0.51, 0.47, and 0.32, respectively; all p < .001) (Figure 4).

Correlation analysis of the factors that affect the location of the radial nerve along the posterior aspect of the humerus. Spearman correlation analysis shows a significant positive correlation between the height of the radial nerve and humeral length.
In the comparison between the male and the female subjects, R1, R2, and R3, as well as the HL and TL, were significantly larger in male subjects than in female subjects (all p < 0.001) (Table 2).
Comparison of measurements between male and female subjects.a

a Values are given as the mean and standard deviation unless otherwise noted.
HL: humeral length; R1: the distance of the olecranon fossa to the entry point of the radial nerve at the posterior aspect of the humeral shaft; R2: the distance of the olecranon fossa to the midpoint of the radial nerve; R3: the distance of the olecranon fossa to the exit point of the radial nerve.
Discussion
In this study, the segment of the radial nerve that laid directly on the posterior aspect of the humeral shaft can be reliably established, and all measurements had excellent intraobserver/interobserver reliabilities. Besides, the HL and TL were found to be reliable values for predicting the course of the radial nerve.
To our knowledge, many previous anatomical studies have used cadavers to determine the course of the radial nerve. However, the limited sample size of cadaveric specimens reduced the precision of the pooled estimates and the ability to detect statistical significance. Additionally, using embalmed cadaveric specimens may have represented a potential limitation: formalin causes shrinkage and dehydration of soft tissue structures, primarily affecting their neurovascular supply, which may alter anatomical measurements. 8,15,27,28 Moreover, disarticulation of the shoulder joint and dissection of the radial nerve to reach sufficient exposure may have affected the native course of the nerve. 8,15 Therefore, we conducted an in vivo anatomical study based on CTA that we believe overcomes these reported drawbacks associated with the use of cadaveric specimens, and we utilized 3D reconstruction of CT scan images of living subjects to simulate the in situ conditions. In the current study, sufficient data were obtained from CTA of living subjects. In addition, since the subjects did not need embalming or dissection, we could define the original course of the radial nerve. Another advantage of our study over conventional anatomical studies that used cadaveric specimens is that manpower and time were less required. In our study, two researchers were responsible for 3D modeling, and it took about 20 min to reconstruct a 3D model of two limbs of a pair humerus and radial nerve. We believe that our research has suggested the possibility of applying the 3D reoconstruction technique to the anatomical domian.
In the current study, all five 3D measurements (HL, TL, R1, R2, and R3) had excellent interobserver and intraobserver reliabilities (the correlation coefficient always greater than 0.90), and the results are comparable to those of other previous cadaveric studies regarding the course of the radial nerve. 7,8,10,14,15 A study detailing the course of the radial nerves in 100 pairs of cadavers by Hackl et al. 8 reported the following measurements: the HL was 30.8 cm (±1.9), transcondylar width was 6.3 cm (±0.6), and distance of the olecranon fossa to the radial nerve at the medial edge of the posterior aspect of the humeral shaft (R1) was 15.0 ± 2.1 cm; at the center of the humeral shaft, the distance (R2) was 12.7 ± 1.6 cm and that at the lateral border (R3) was 10.6 ± 1.3 cm. These measurements are very similar to the corresponding values in our study. Reported measurement differences among another study may have been due to the difference in points chosen for the measurement or variability in the course of the radial nerve in the distal aspect. 7,13,15,27,29
The course of the radial nerve was found to have a significant correlation with patients’ HL and TL. This finding is supported by several previous studies. 8,14 Hackl et al. 8 reported that the HL and transcondylar width correlated with the distance of the radial nerve to the olecranon fossa (r = 0.451–0.565). Kamineni et al., 14 in their cadaveric study regarding the relationship of the radial nerve to the elbow joint, demonstrated a positive correlation between the transepicondylar distance and the radial nerve lateral height (defined as the distance between the lateral epicondyle and the point at which the radial nerve crosses the humerus in the mid-lateral plane). Interestingly, despite the correlation of the HL and TL with the course of the radial nerve, its correlation coefficient was reduced as the radial nerve coursed distally. This finding is thought to be related to the variability of the course of the radial nerve, especially at the distal site. Our result supports that of previous literature, suggesting a great deal of variability in the course of the radial nerve, particularly at the distal aspect of the humerus. 13,15,29,30
The course of the radial nerve expressed as the absolute numerical value (R1, R2, and R3) may not be transferred to extremely larger or smaller people. Instead, more normalized values, such as R1/HL, R2/HL, and R3/HL and R1/TL, R2/TL, and R3/TL, could give predictable measurements that account for the interindividual variation of the location of the radial nerve in proportion to the patient’s size. 8,14,15 Thus, for example, multiplying the HL by a certain constant (0.54, 0.49, and 0.38 for R1, R2, and R3, respectively) can result in a more reliable prediction of the course of the radial nerve.
In our study, R1, R2, and R3, as well as the HL and TL, were significantly larger in male subjects than in female subjects. There appears to be a debate as to whether the course of the radial nerve differs according to sex or race. Hackl et al. 8 noted that the HL and the transcondylar width were higher in male specimens than in female specimens; however, there was no sex-specific difference observed regarding the distance of the radial nerve in relation to the olecranon fossa. However, Uhl et al. 31 reported a difference in height from the distal articular surface of the elbow joint to the radial nerve tethered in the lateral intermuscular septum between male and female patients. Chou et al. 10 compared the distribution of the radial nerve in the upper arm of Chinese cadavers with those of Caucasian cadavers and elucidated racial differences. Further anatomical studies of high-quality data collected from a large, nationwide sample are necessary. Moreover, a unification of the reference point to determine the course of the radial nerve would be beneficial.
There are several limitations to this study. First, validating the accuracy and reproducibility of 3D rendering is insufficient. Second, there is a possibility for bias because of the subjective nature of setting the threshold of HU for the segmentation of each humerus. To validate the accuracy of 3D rendering, further studies are needed to compare the results of 3D rendering with those from the same cadaveric specimens. Third, although the same supine position with both upper extremities placed over the head is used for obtaining CTA images, varying degrees of extension or flexion of the elbow among individuals during imaging may have introduced bias. 10 Besides, in the clinical aspect, the positions of the elbow during surgery in the posterior approach or external fixation of the humeral shaft may be somewhat different from those from our analysis, which could affect the course of the radial nerve. Recently, Chen et al. 9 noted that radial nerve excursion is affected by the position of the elbow, as the elbow is flexed from 0° to 90°, excursion of the radial nerve is doubled. Therefore, our results should be interpreted with caution, and further study regarding the impact of the various positions of the elbow on the course of the radial nerve would be beneficial. We assumed the data from the left and right arms are independent. Given the physiological symmetry, this assumption may be incorrect and thus may cause overestimation of the importance of the differences. Lastly, our study could have been performed using non-enhanced preoperative CT images. However, as a retrospective study, our institute lacked CT scans of a whole-length and intact (not fractured) humerus. On the other hand, upper extremity CTA has the advantage of providing whole length, intact, and bilateral humeral images.
Conclusions
In summary, the distance from the olecranon fossa to the entry point of the radial nerve’s direct contact with the posterior humeral shaft (R1) was 159.2 (range 127.1–198.2) mm, midpoint (R2) was 136.6 (105.7–182.5) mm, and exit point (R3) was 112.8 (76.8–150.0) mm on average, and these values can be reliably predicted by the HL and TL. Our results verified that the 3D model measurements have excellent reliability and consistency with those in previous cadaveric studies. Therefore, orthopedic surgeons should be aware that when using the posterior approach for the humeral shaft fracture, the radial nerve may be in direct contact with the posterior humeral shaft from 76.8 mm (minimum value of R3) to 198.2 mm (maximum value of R1) proximal to the olecranon fossa. In addition, in patients who are too large or small, the HL or TL can be reliably used to predict the course of the radial nerve to avoid iatrogenic injury.
Supplemental material
suppplementary_figures - Three-dimensional measurement of the course of the radial nerve at the posterior humeral shaft: An in vivo anatomical study
suppplementary_figures for Three-dimensional measurement of the course of the radial nerve at the posterior humeral shaft: An in vivo anatomical study by Ji-Kang Park, Seung-Myung Choi, Sang-Woo Kang, Kook-Jong Kim and Kyoung-Tae Min in Journal of Orthopaedic Surgery
Footnotes
Data availability statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval and informed consent was waived because of the retrospective nature of the study. The study was approved by the institutional review board of Chunbuk National University Hospital institution.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the research grant of the Chungbuk National University Hospital in 2017.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.