
Abstract
Purpose:
The purpose of this article is to explore the real-life practice of clinical management of humeral shaft fracture associated with traumatic radial nerve palsy among orthopedic trauma surgeons.
Methods:
Two hundred seventy-nine orthopedic surgeons worldwide reviewed 10 real cases of a humeral shaft fracture associated with traumatic radial nerve palsy answering two questions: (1) What treatment would you choose/recommend: nonoperative or operative? (2) What are the reasons for your decision-making? The survey was developed in an online survey tool. All participants were active members from AOTrauma International.
Results:
Two hundred sixty-six (95.3%) participants were from Latin America and Asia/Pacific. One hundred sixty-two participants (58.1%) had more than 10 years in practice and 178 (63.8%) of them did trauma as the main area of interest. One hundred fifty-one (54.1%) participants treated less than three humeral shaft fractures a month. Traumatic radial nerve palsy was the main reason (88.4%) for surgeons to recommend surgical treatment. Open reduction and internal fixation (ORIF) or percutaneous fixation of the fracture associated with acutely explore of radial nerve was the first option in 62.0% of the cases. A combination of morphology and level of the fracture and the presence of the radial nerve palsy was the most suggested reason to surgically treat the humerus fracture. The main isolated factor was the morphology of the fracture.
Conclusion:
Our survey highlight the tendency for a more aggressive management of any humeral shaft fracture associated with a traumatic radial nerve palsy, with surgeons preferring to use ORIF with acute exploration of the radial nerve. Nonsurgical management was the less chosen option among the 279 respondents. Fracture morphology, level of the fracture, and the presence of the radial nerve palsy were most influential for guiding their treatment.
Introduction
Traumatic radial nerve palsy is the most common peripheral nerve injury complicating humeral shaft fractures, with an incidence ranging between 2% and 17%. 1 –3 The management of this particular injury and the clinical decision-making is still based on the empiric evidence garnered from literature with low evidence level. 4 In addition, the fate of elevated rates of recovery of the radial nerve (about 92% after closed fractures and 85% after open fractures) makes the decision between exploration andr not of a traumatic radial nerve palsy associated with a humeral fracture a continual subject of controversy.
Treatment options include expectant observation, early exploration, late exploration, or tendon transfers. 2,3 Initial nonsurgical management avoids the potentially surgical insult, conversely surgical exploration warrants early detection of a radial nerve entrapment or transection. This brings a challenging acute decision to the surgeon, mainly in closed fractures where there is no obvious reason to consider for immediate exploration of the nerve. Early exploration of the radial nerve has been advocated in cases of open humerus fracture or when surgical treatment is elected for other reasons. 1,2,5
Another source of confusion to deliberate between to explore and not a traumatic radial nerve palsy associated with a humerus shaft fracture is the complete lack of objective clinical and radiological factors. Anecdotally, high-energy humerus fractures and extensive local soft-tissue damage have been considered indications for early exploration and repair of a radial nerve lesion. 6 Again, these indications are mainly based on personal experience more than evidence-based data, thus patient selection criteria and optimum treatment method have yet to be established. Identifying a high-risk group for adverse outcome using objective factors, as the energy of trauma and the level of the fracture, will ultimately allow a safe algorithm for the management of this injury.
Nowadays, there is a growing tendency to use survey tools to help elucidate how surgeons are making treatment decisions and what factors are perceived to be important in choosing an appropriate treatment based on each individual experience. In the current study, we administered an online cross-sectional survey to understand orthopedic trauma surgeons’ perceptions of the importance of traumatic nerve palsy relative to definition of humerus shaft fracture management. In addition, we asked them to define which factor or factors influenced their decision.
Methods
Survey design and distribution
The survey was developed in an online survey tool, SurveyMonkey (Palo Alto, California, USA). We collected 10 cases of humeral shaft fracture associated with traumatic radial nerve palsy with adequate radiographic documentation and complete follow-up. The questionnaire addressed surgeons’ preference of methods for initial management—(1) What treatment would you choose/recommend—and the reason for the decision-making—(2) What reason(s) or What is(are) the reason(s) that led to this decision?. Specifically in question (2), respondents were surveyed on the factors that dictated their decision.
According to the Arbeitsgemeinshaft für Osteosynthesefragen (AO) classification, there were one fracture 12-A1, one 12-A3, one 12-B1, three 12-B2, one 12-B3, one 12-C2, and two 12-C3. Two fractures were open, both Gustilo et al. grade 3A—one patient suffered a firearm injury and the other had a motorcycle accident. The mean age was 34.6 years old, ranging between 21 and 67 years old. There were six male and four female patients. In seven patients, the dominant side was injured (Table 1).
Demography of the patients.a

aClinical Decision Rules Group, 2016.
Invitations to participate were sent between August 2015 and December 2015. Survey was distributed to orthopedic trauma surgeons affiliated to the AO Trauma International (AOTI). An e-mail was sent with a cover letter describing the objectives of the study and providing a link to the survey. We sent one follow-up e-mail, approximately a month apart, to all nonresponders to remind them to complete the survey. The questionnaire was sent in English for the members from AOTI North America, Europe (except Portugal), Asia/Pacific, and Middle East; in Spanish for members from AOTI Latin America (LA; except Brazil); and in Portuguese for members from AOTI in Brazil and Portugal.
Statistical analysis
Descriptive statistics was calculated as frequencies with percentages and continuous variables as mean with standard deviation. The Mann–Whitney U-test was used to compare numerical variables in independent groups, such as geographic region and treatment option, mainly between surgeons from LA and Asia/Pacific. The Fisher’s exact test was used to test the association between the treatment option and the factors that influenced the decision-making. All reported p values are two tailed with p < 0.05 being considered significant.
Results
Characterization of the participants
There were 279 participants in this survey. Of those who completed the survey, 266 (95.3%) were from LA (n = 142, 50.9%) and Asia/Pacific (n = 124, 44.4%). The other 13 participants were from North America and Europe. There were no participants from Middle East.
One hundred sixty-two participants (58.1%) had more than 10 years in practice and 178 (63.8%) of them did trauma as the main area of interest. One hundred fifty-one (54.1%) participants treated less than three humeral shaft fractures a month. Figure 1 shows the correlation between the degree of experience in orthopedics and the number of humerus shaft fractures treated a month.

Degree of experience versus humerus shaft fractures treated a month.
Fracture treatment
Surgeons were more likely to recommend surgery for a patient presenting a humerus shaft fracture with traumatic radial nerve palsy (88.4%), with 62.0% of them preferring to acutely explore the radial nerve, either by open reduction and internal fixation (ORIF) or percutaneous fixation of the fracture (p < 0.05). Interestingly, 26.3% of the participants chose to only perform percutaneous fixation at the first moment, without exploring the radial nerve (Figure 2).

Preferred treatment for humeral shaft fractures associated with traumatic radial nerve palsy. NonS: nonsurgical; PFix: percutaneous fixation; PFix+: percutaneous fixation and acute radial nerve exploration; ORIF+: open reduction and internal fixation plus acute radial nerve exploration; No: number of responses (there were a total of 2790 responses).
A comparison was established on the preferred treatment among orthopedic trauma surgeons from LA and Asia/Pacific, as they represented 95.3% of the respondents (Figure 3). Again, the majority either preferred ORIF with acute exploration of the radial nerve or percutaneous fixation without exploring the radial nerve. There was no statistically significant difference among those surgeons on the preferred treatment for a humeral shaft fracture associated with traumatic radial nerve palsy (p = 0.08).

Comparison on the preferred treatment among surgeons from LA and Asia/Pacific. There was no statistically significant difference (p = 0.08). NonS: nonsurgical; PFix: percutaneous fixation; PFix+: percutaneous fixation and acute radial nerve exploration; ORIF+: open reduction and internal fixation plus acute radial nerve exploration; No: number of responses (there were a total of 2790 responses); LA: Latin America.
Suggested reasons for decision-making
The major factors to operate on a patient with humeral shaft fracture associated with radial nerve palsy were (i) the morphology of the fracture, (ii) the presence of the radial nerve injury, (iii) the level of the fracture, and (iv) the mechanism of trauma. A combination of morphology and level of the fracture and the presence of the radial nerve palsy was the most suggested reason to surgically treat the humerus fracture. The main isolated factor was the morphology of the fracture. Figure 4 shows the five most suggested reasons for decision-making.
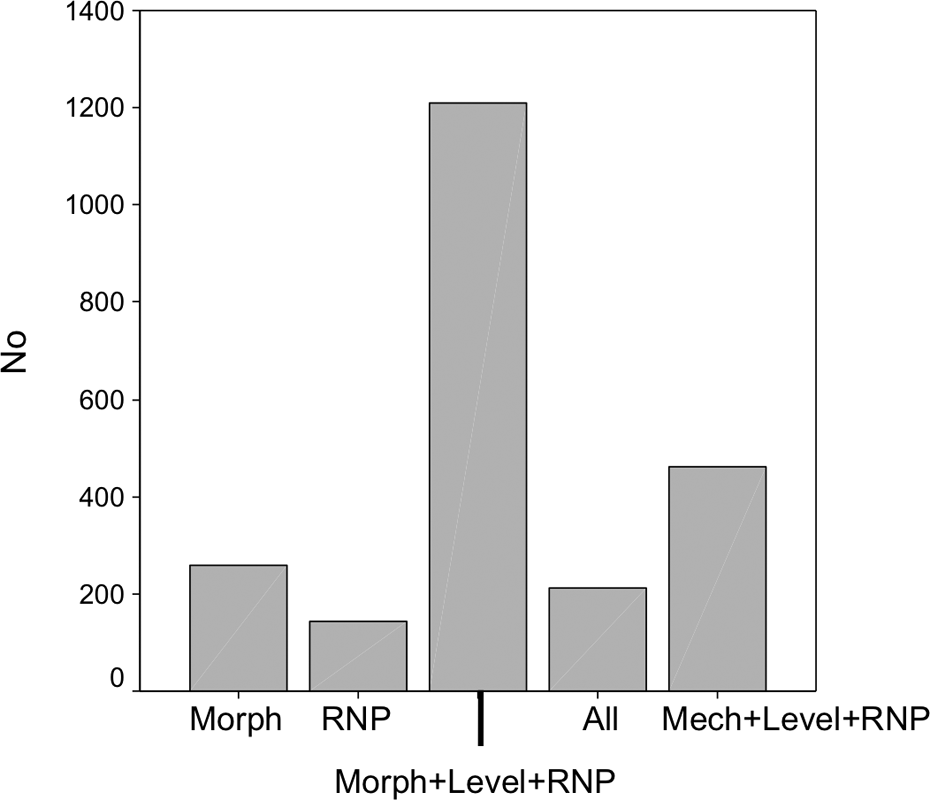
Five most suggested reasons for decision-making. Morph: morphology of the fracture; RNP: radial nerve palsy; Morph+Level+RNP: morphology and level of the fracture and radial nerve palsy; All: morphology and level of the fracture, radial nerve palsy, and mechanism of trauma; Mech+Level+RNP: mechanism of trauma, level of the fracture, and radial nerve palsy; No: number of responses (there were a total of 2790 responses).
Of note, cases 4 and 7 had the mechanism of injury as the main factor for the indication of surgical treatment. In both cases, patients had a high-energy trauma causing severe open fracture. Case 4 presented a 21-year-old right-hand-dominant male who suffered an injury by firearm during a robbery, sustaining a left open multifragmentary humeral shaft fracture with traumatic radial nerve palsy and case 7 showed a 30-year-old right-hand-dominant male dispenser who had a motorcycle accident, sustaining a Gustilo et al. type 3A open left transverse humeral shaft fracture associated with a traumatic radial nerve palsy (Figures 5 and 6).

Case 4: Radiographs of a 21-year-old right-hand-dominant male who suffered an injury by firearm during a robbery, sustaining a left open multifragmentary humeral shaft fracture with traumatic radial nerve palsy.

Case 7: Radiographs of a 30-year-old right-hand-dominant male dispenser who had a motorcycle accident, sustaining a Gustilo et al. type 3A open left transverse humeral shaft fracture associated with a traumatic radial nerve palsy.
The major factors for the decision-making for each case are presented in Figure 7.
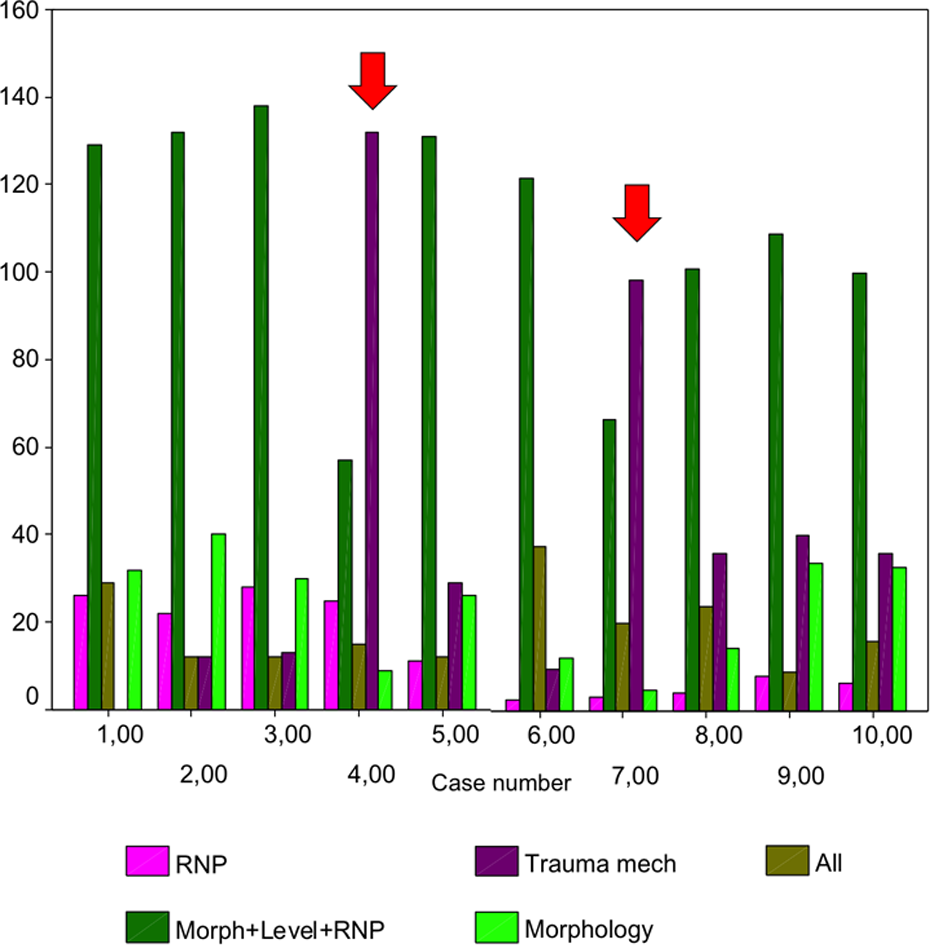
Five most suggested reasons for decision-making for each case. Note the red arrow in cases 4 and 7 demonstrating the trauma mechanism as the main factor for the surgical treatment of the fracture. RNP: radial nerve palsy; Morph+Level+RNP: morphology and level of the fracture and radial nerve palsy; All: morphology and level of the fracture, radial nerve palsy, and mechanism of trauma; Trauma mech: Trauma mechanism. There were a total of 279 responses per case.
Discussion
Whether or not acutely exploring a traumatic radial nerve palsy associated with a humeral shaft fracture is indicated is still a source of controversy. Despite many personal recommendations accumulated from retrospective case series, no standardized criteria have been defined to operate on or not this devastating injury. In general, closed humeral shaft fracture associated with radial nerve palsy presents a spontaneous recovery rate in up to 80%, thus suggesting that acute operation may not be required. 2 –4,7 In addition to that, early surgical exploration in this particular situation rarely demonstrates macroscopic reparable nerve damage. In fact, a systematic review study by Shao et al. found that initial expectant treatment does not affect the extent of nerve recovery adversely, thus avoiding unnecessary operations. 8 In another study, Bishop and Ring showed that observation is the optimal treatment strategy when managing traumatic radial nerve palsy associated with a humerus fracture. 9 On the other side, open fractures and high-energy trauma mechanism are generally considered for operative management because of the elevated rate of nerve entrapment or transection. 5,6
The current study provides important information about attitudes of orthopedic surgeons all over the world regarding the treatment of humeral shaft fracture associated with traumatic radial nerve palsy. Although initial conservative management has shown good fracture healing and high rate of nerve recovery, respondents overwhelmingly believe that fracture fixation is the best treatment in these cases, clearly demonstrating a change of concept, with gradual abandonment of nonsurgical treatment. This finding was completely unexpected for us as 8 of 10 cases presented low-energy closed humerus shaft fractures, theoretically amenable for observational conservative management.
We believe the difficulty to keep adequate splinting of the fracture, actual global need for fast return to daily labor activities, and nerve damage have greatly contributed to the change. As a matter of fact, 62.0% of the respondents preferred to acutely explore the radial nerve, 46.4% of them preferring ORIF, probably reflecting both surgeons’ training and better visual inspection of both fracture reduction and the radial nerve. 3 Minimal invasive percutaneous osteosynthesis techniques, either with extramedullary or intramedullary implants, were preferred for 41.9% of the participants. Although this was not the first choice for the majority of the participants, there is an obvious tendency for a less invasive approach for several traumatic injuries and this can also be considered for the humerus shaft. 10,11
In eight cases, a combination of morphology and level of the fracture and the presence of the radial nerve palsy were the most suggested reason to surgically treat the humerus fracture, with the morphology of the fracture being the major isolated factor. This is in accordance with the general literature, where acute indications for surgical exploration of the radial nerve include spiral or oblique fracture patterns in the middle to distal one-third of the humeral shaft with associated radial nerve palsy (like the Holstein–Lewis fracture pattern), open fractures with associated radial nerve palsies, and radial nerve palsy after a penetrating injury. 3,5 In two cases with open high-energy fractures, the mechanism of injury was the main factor for the indication for surgical treatment. This observation is corroborated by the study of Venouziou et al., who found severely damaged radial nerves in 8 of 13 patients presenting radial nerve palsy associated with humeral shaft fracture. 12 Patients with high-energy trauma had a significantly prolonged fracture healing time and unfavorable nerve recovery compared to those with low energy fractures and should be informed of the poor prognosis and the potential need of tendon transfers in the future.
Our findings highlight the tendency for a more aggressive management of any humeral shaft fracture associated with a traumatic radial nerve palsy, it does not matter whether closed or open, low energy or high energy, or more proximal, midshaft, or more distal. However, the beliefs and practices of the surgeons surveyed may not reflect a worldwide therapeutic decision-making, as 266 (95.3%) participants were from LA and Asia/Pacific. This observation can be seen as strength but at the same time as weakness, since these two population samples present very different cultures, social habits, and economies. It is known by far that heterogeneity in assessment can reflect a potential for significant heterogeneity in management.
The greatest impact of this observation may be that it allows for a comparison among surgeons of two parts of the globe with its socioeconomic differences, as mentioned before. Interestingly, in both regions, most surgeons preferred ORIF with acute exploration of the radial nerve, with no statistically significant difference on the preferred treatment for a humerus shaft fracture associated with traumatic radial nerve palsy (p = 0.08). It is noteworthy that among surgeons in LA and in Asia/Pacific, both nonsurgical treatment and percutaneous fixation with exploration of the nerve were less chosen. The reasons for this huge difference are unclear for us. It is possible that some of the surgeons believe nonsurgical treatment brings the difficulty to keep adequate splinting of the fracture and some of them prefer to explore the radial nerve with a formal open approach. In this regard, we feel further investigation is necessary to elucidate these reasons. Nevertheless, both methods should be considered when managing a humeral shaft fracture associated with traumatic radial nerve palsy.
This article carries some limitations. First, 266 respondents were from LA and Asia/Pacific, thus our observations do not address specifically how the injury is managed in other regions, particularly in North America and Europe. However, we do not believe responses would be much different than we got, as all the surgeons are active members from AOTrauma International and in general have similar practices and preferences for managing humeral shaft fracture associated with traumatic radial nerve palsy. Second, in the present study we do not examine specific aspects related to the treatment, as the choice of approach for ORIF, definition of the implant and the type of immobilization, in the case of nonsurgical management, and adopted protocol to evaluate the radial nerve palsy recovery. Our interest was in surgeons’ expertise on how and why professionals treat this devastating injury. There is no doubt that these questions deserve focused attention, given its potential relevance for both surgeons and patients, and we believe our initiative can allow future research to assess those specific information. Finally, investigations such as the present study are not intended to define a surgeon’s behavior on decision-making for any clinical condition in medicine but to generate conversation and hypotheses. Therefore, we feel our efforts might yield valuable insights to opportunely establish a rationale for managing patients with humeral shaft fracture associated with traumatic radial nerve palsy.
Conclusion
Our survey highlights the tendency for a more aggressive management of any humeral shaft fracture associated with a traumatic radial nerve palsy, with surgeons preferring to use ORIF with acute exploration of the radial nerve. Nonsurgical management was the less chosen option among the 279 respondents. Fracture morphology, level of the fracture, and the presence of the radial nerve palsy were most influential factors for guiding their treatment.
Footnotes
Acknowledgment
The authors would like to aknowledge AO Trauma Latina America Board for the academic support and all AO Trauma members from Asia-Pacific and Latin America that participated answering the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.