
Abstract
Purpose:
The purpose of this study was to clinically compare the single-incision and dual-incision approaches for the treatment of distal tibial and fibular fractures.
Methods:
In total, 93 patients were enrolled, and the mean follow-up was 15 months (range 12–19 months). The patients treated for open reduction and internal fixation were randomly classified into two groups based on the approach used: 45 patients were treated using the single-incision approach (group 1) and 48 patients were treated using the dual-incision approach (group 2). In these two groups, operation time, discharge time, postoperative complications, and ankle function evaluations (Olerud–Molander Ankle Score) were compared between the two groups.
Results:
There were no significant differences in the mean operation time (98.2 ± 18.5 vs. 103.6 ± 19.3), discharge time (11.1 ± 3.9 vs. 12.5 ± 5.7), overall surgical complication rates (9/45 vs. 15/48), or ankle function between the two groups (p > 0.05). However, the rate of soft tissue-related complications, such as skin slough, infection, nonunion, and delayed union, was significantly lower in group 1 (5/45) than in group 2 (14/48) (p < 0.05).
Conclusion:
The two incision approaches were found to have similar clinical outcomes. However, with regard to soft tissue conservation, the single-incision approach was superior to the dual-incision and maybe a reliable alternative.
Introduction
Distal tibial and fibular fractures commonly result from high-energy trauma, such as fall from a height that results in axial compressive injury, direct bending, or rotational force due to motor vehicle accidents or twisting injuries. 1,2 Due to the etiology, fracture types, and anatomic characteristics, distal tibial and fibular fractures often result in nonunion and soft tissue complications. 3
The following methods may be used to treat distal tibial and fibular fractures depending on the specific situation: closed reduction and cast application; external fixation; a combination of limited internal fixation with the application of an external fixation; or open reduction and internal fixation (ORIF) with plates, nails, and screws. However, for certain fracture types, orthopedic surgeons may prefer ORIF as a final treatment, which follows the AO principles of anatomical reduction, rigid fixation, and early mobilization. In these situations, two separate incisions are performed: an anterior incision to the distal tibia and a lateral incision to the distal fibula. These combined incisions may lead to extensive soft tissue injury and periosteal damage with a subsequently high risk of soft tissue necrosis and nonunion. Furthermore, when the initial injury involves extensive soft tissue damage or the combined incisions are separated by a distance of 7 cm or less, a poor outcome may be inevitable. 4
As a result, several alternative techniques have been proposed for the preservation of soft tissue at the fracture site. In recent years, a single-incision approach has been suggested for the treatment of distal tibial and fibular fractures. Several studies have evaluated the feasibility of this approach and its application to clinical practice. 5,6 To the best of our knowledge, research on the clinical prognoses of this approach, such as the rates of skin slough, infection, nerve injury, nonunion, and delayed union, remains limited.
The current study was based on the hypothesis that the single-incision approach has advantages in clinical outcome, especially with regard to soft tissue conservation, over the dual-incision approach. As a result, the study aimed to compare the single-incision approach with the dual-incision using clinical findings with the ultimate aim to provide guidance in clinical practice.
Methods
Patient demographics
Between June 2016 and June 2018, 126 patients (86 males and 40 females) presenting with distal tibial and fibular fractures that required fixation were treated by the single-incision approach (group 1) or the dual-incision approach (group 2). The study was approved by the medical ethic of authors’ affiliated institutions and all subjects provided informed consent prior to their participation in the study. The inclusion criteria were as follows: closed metaphyseal fracture, including all types of distal tibial and fibular fractures, based on the AO classification system, modified by Müller. 7 The exclusion criteria consisted of medial or posterior malleolus fractures requiring operation, open fractures, historical operation of the distal tibial and fibular fractures, and the patients who were lost to follow-up. Finally, 93 patients (63 males and 30 females) completed the study and were included in the final outcome analysis. This sample size met the results of a power analysis. The demographics and injury conditions of the patients in both groups were noted in detail and compared (Table 1).
Demographics and injury conditions of the patients.a
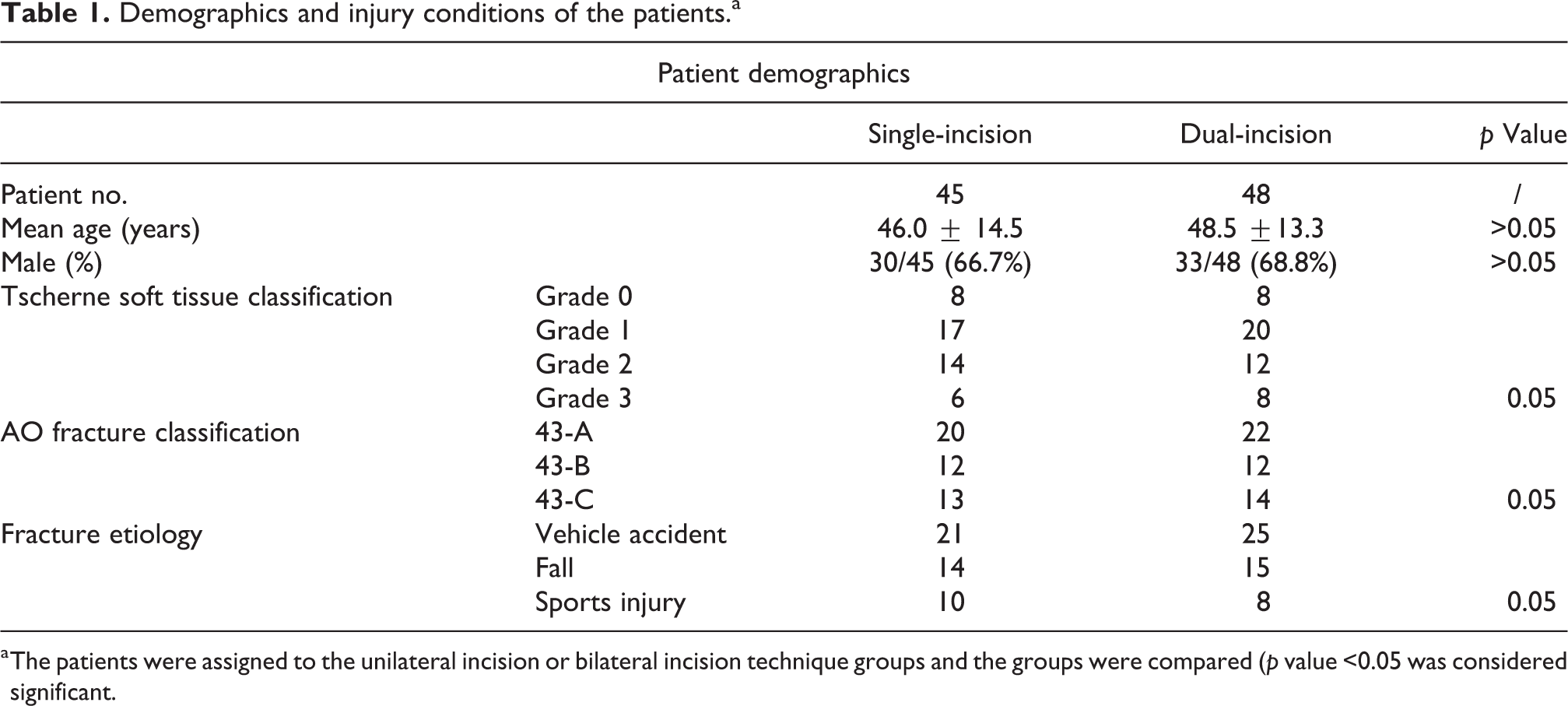
a The patients were assigned to the unilateral incision or bilateral incision technique groups and the groups were compared (p value <0.05 was considered significant.
Before the operation, each patient received routine examinations by standard X-ray and computed tomography scan with reconstruction. Patient allocation to groups was randomized by computer prospectively through the use of sequentially numbered opaque envelopes. Envelopes were opened inside the operating theater by a nurse who was blind to the allocation. The surgeries were performed by one attending traumatic surgeon and two trauma fellows as surgical assistants, who all had significant experience in traumatic surgeries at a single institution. Surgical implants were provided by the same device manufacturers. The assessments were conducted by two surgical fellows, and when there were disagreements in the assessment, the final scoring of the images was conducted by the attending surgeon.
Operative procedures
Single-incision approach
After subarachnoid block anesthesia, the patient was placed in the supine position with a cushion placed underneath the ipsilateral hip to prevent the usual external rotation of the operative limb. The operative limb was tourniquet inflated and straightened in an appropriate fashion. The maximal duration of tourniquet was 90 min, and tourniquet would be released before the final closure. Centering on the fracture line of distal leg, a longitudinal anterolateral incision was performed on the skin and subcutaneous tissues along the projection line of the extensor digitorum longus muscle between the tibia and fibula. The distal end of the incision was allowed to be extended to slightly above the ankle joint. The proximal end of the incision could also be further extended, depending on the placing requirement of internal fixation. The fibular fracture was the first to be exposed when the peroneus longus and brevis muscles were retracted laterally. Either one-third tubular plate or distal fibular anatomical locking plate (AO/Synthes, New Jersey, USA) was applied for distal fibular fracture depending on the location of the fracture line. Superficial peroneal nerve should be exposed carefully and retracted medially along with the extensor digitorum longus. Reduction was managed so as to achieve the length reference of the tibia. Next, the tibialis anterior, extensor hallucis longus, and extensor digitorum longus muscles were together retracted laterally in the proximal part of the fracture. The tibialis anterior and deep peroneal nerve would be retracted medially at the distal end to expose the distal tibia. When a reduction of the tibial fracture was achieved, an anterolateral L-anatomical locking plate (Wego Group Co., Ltd, Shandong, China) was applied on the lateral aspect of the tibia for fixation (Figure 1).

A 53-year-old female suffered a car crash, sustaining a closed distal tibial and fibular fracture (OTA: 43-A1 and 44-C; Tscherne soft tissue classification: grade 1). The operation procedure was managed by a single-incision approach. (a) Superficial markings for the longitudinal incision were made along the projection line of the extensor digitorum longus muscle. (b) The soft tissue was blunt dissected between the peroneal and extensor muscles. The superficial peroneal nerve (star) was exposed and protected. (c) The fibular fracture was the first to be fixed. (d) The tibialis anterior muscle (star) and other muscles could be retracted laterally in the proximal part of the fracture. (e) The extensor digitorum longus (star) and the superficial peroneal nerve were retracted medially in the distal end to expose the distal tibia. (f) Vacuum drainage was positioned and the incision was closed without tension. OTA: Orthopedic Trauma Association.
Dual-incision approach
Operation preparation was similar to that for the single-incision approach. Briefly, the fibular fracture was the first to be exposed, and a longitudinal lateral incision was performed along the projection line of the posterior fibular border. The soft tissue was posteriorly blunt dissected over the fibula to allow reduction and plate fixation (AO/Synthes) while taking care to restore the length, alignment, and rotation, allowing for a stable and diaplastic lateral column to achieve reconstruction of the distal limb. The tibial fracture was then managed as follows: Centering on the fracture line of the distal tibia, a slightly curved longitudinal incision was made from the proximal end, 1 cm from the lateral site of the tibia crest to the distal end of the medial malleolus, crossing through the anterior tibial muscle tendon. The soft tissue was blunt dissected and the extensor retinaculum was incised. The anterior tibial muscle tendon was retracted laterally to expose the anterior part of the distal tibia. Next, the reduction of the tibial fracture was performed surgically, and an anterolateral L-anatomical locking plate (Wego Group Co., Ltd) fixation for the lateral site of the tibia was accomplished (Figure 2).

A 56-year-old male suffered a car crash, sustaining a closed distal tibial and fibular fracture (OTA: 43-B1 and 44-B; Tscherne soft tissue classification: grade 1). The operation procedure was managed by a dual-incision approach. (a) A longitudinal lateral incision was performed along the projection line of the posterior fibular border and the fibular fracture was the first to be fixed. (b) Centering on the fracture line of the distal tibia, a slightly curved longitudinal incision was made anteriorly to expose the distal tibia fracture. (c) Reduction of the tibial fracture was performed surgically and an anterolateral L-anatomical locking plate and screws fixation for the lateral site of the tibia was accomplished. (d) Vacuum drainage was positioned and the incision was closed without tension. OTA: Orthopedic Trauma Association.
Intraoperative and postoperative data
During the operation, intraoperative blood loss was recorded in detail. Furthermore, the key steps of both approaches were clearly photographed.
At the postoperative follow-up, all patients were assessed with X-rays within 24 h (Figure 3). The reduction quality of the tibial and fibular fractures was evaluated by two surgical fellows. Radiological deformity was assessed by three parameters: shortening (>10 mm), anteroposterior angulation (>10°), and lateral angulation (>5°). 8 The fractured leg was protected by a below-knee cast for 4–6 weeks, depending on the bone quality and fracture type. Patients were discharged from hospital when their vital signs were stable and there was no exudation from the incision. Mobilization of the ankle and permission to weight-bearing were determined on a case-by-case basis following an assessment of visual analog scale pain score, local edema, image examination, and the stability obtained at the time of fixation. All patients were followed up at least until full weight-bearing and healing of the soft tissue were achieved (median 15 months; range 12–19 months; Figure 4). During follow-up, the patients were asked to visit the outpatient clinic at 4 weeks, 3 months, 6 months, and 1 year after surgery. Telephone follow-up was supplemented if necessary. All fractures were reviewed with postoperative X-rays by an orthopedic surgeon during each clinic visit. Range of motion (ROM) of ankle plantar flexion and dorsiflexion was measured with a goniometer at 1 year after surgery. In addition, the ankle function was evaluated using the Olerud–Molander Ankle Score. 9

Two cases of closed distal tibial and fibular fractures. (a)–(d) Case 1 (OTA: 43-A1 and 44-C; Tscherne soft tissue classification: grade 1) received surgery through single-incision approach. (e)–(h) Case 2 (OTA: 43-B1 and 44-B; Tscherne soft tissue classification: grade 1) received surgery through dual-incision approach. (a) and (e) Preoperative AP radiograph. (b) and (f) Preoperative lateral radiograph. (c) and (g) Postoperative AP radiograph. (d) and (h) Postoperative lateral radiograph. AP: anteroposterior; OTA: Orthopedic Trauma Association.
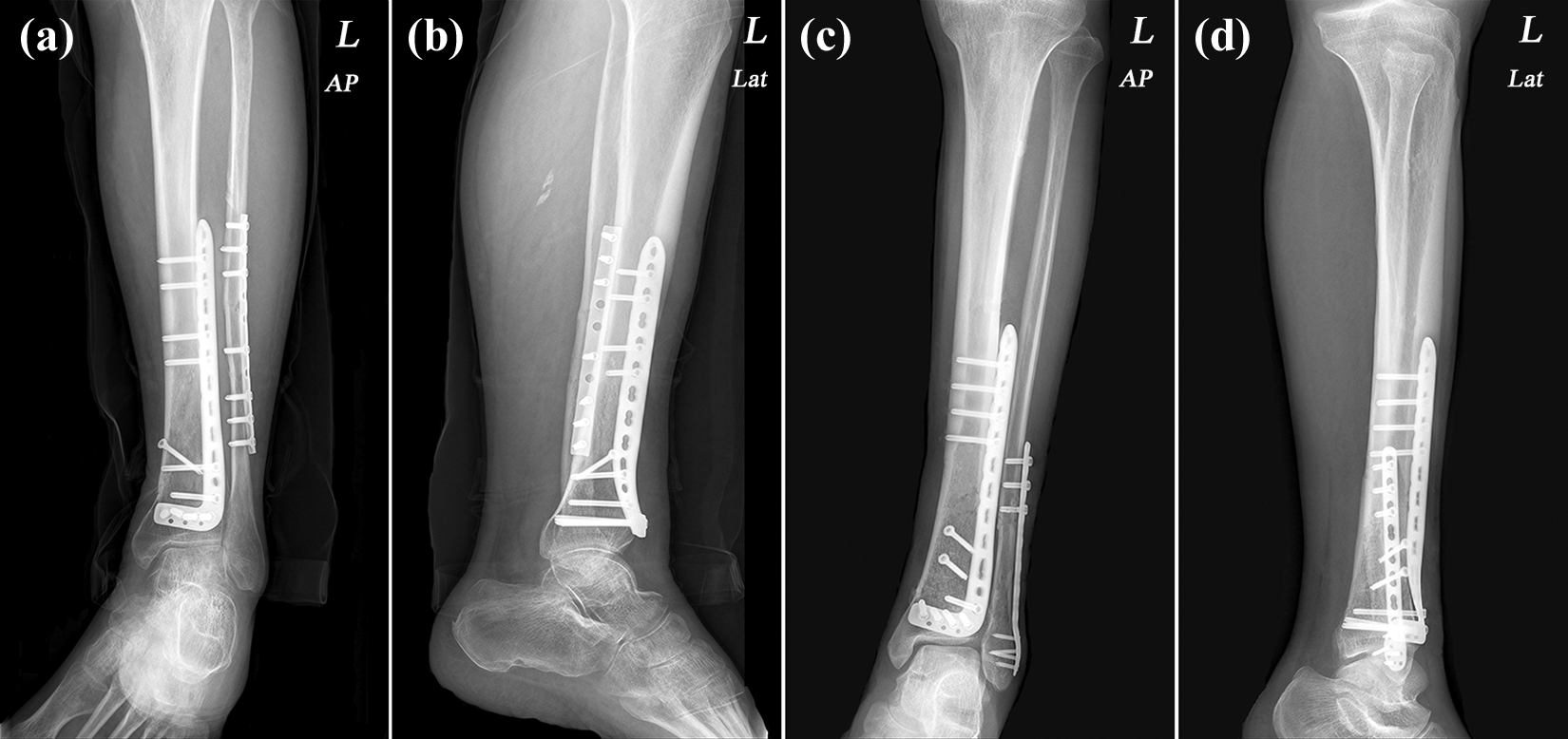
Two cases of closed distal tibial and fibular fractures. Postoperative X-rays show the complete healing of the fractures of both cases at 12 months after surgery. (a) and (b) Case 1 (OTA: 43-A1 and 44-C; Tscherne soft tissue classification: grade 1) received surgery through single-incision approach. (c) and (d) Case 2 (OTA: 43-B1 and 44-B; Tscherne soft tissue classification: grade 1) received surgery through dual-incision approach. Postoperative images of both cases showed dense callus and blurred fracture lines. OTA: Orthopedic Trauma Association.
Statistics
Descriptive statistics were recorded and collated, and the mean and standard deviation for the patient demographics and intraoperative outcomes were calculated from the original dataset. An unpaired t-test was used to compare the patient demographics and intraoperative outcomes between the two groups, and the χ 2 test was used to measure the association between the categorical data of the two groups. Results were considered significant when p <0.05. All statistical analyses were performed using SPSS 22.0 (SPSS Inc., Illinois, USA).
Results
During the study period, 93 patients completing the follow-up were recruited to either group 1 or group 2. There were no significant differences in the age, sex, distributions of Tscherne soft tissue classification, AO fracture classification, and fracture etiology between the two groups (p > 0.05; Table 1).
During surgery, the operation time of each patient was meticulously recorded. The operation time (98.2 ± 18.5 min vs. 103.6 ± 19.3 min) was not significantly different between the two groups (p > 0.05; Table 2). After surgery, the complication rate and function evaluation were the primary focus of this study. Patients were discharged from hospital when their vital signs were stable and there was no exudate from the incision. Radiographic evaluation revealed no radiological deformity in the study (p > 0.05). No significant differences were observed in ankle function at each follow-up period (p > 0.05). And ROM of dorsiflexion and plantar flexion was equal between two groups at 12 months after surgery (p > 0.05). There was no significant difference in discharge time between group 1 (11.1 ± 3.9 days) and group 2 (12.5 ± 5.7 days; p > 0.05). Moreover, the overall surgical complications, including skin slough, infection, nonunion, delayed union, nerve injury, and deformity, were followed for at least 12 months (range 12–19 months; mean 15 months) and registered in detail. In group 1, two cases of skin slough, two cases of delayed union, four cases of nerve injury, and one case of infection arose after surgery. In group 2, five cases of skin slough, two cases of superficial infection, two cases of nonunion, five cases of delayed union, and one case of nerve injury were recorded during the follow-up. There were no significant differences in the number of overall surgical complications between group 1 and group 2 (p > 0.05; Table 2). However, with regard to soft tissue-related complications, such as skin slough, infection, nonunion, and delayed union, the rate was significantly lower in group 1 (5/45) than in group B (14/48; p < 0.05). Two cases of nonunion and three cases of skin slough required surgical revisions, and all surgical complications eventually healed after intervention.
Intraoperative and postoperative data of patients.a

a Mean operating time, postoperative complications, discharge time, and ankle function were recorded and compared (p value <0.05 was considered significant).
Discussion
Soft tissue complication, a potential contributing factor to infection and delayed union/nonunion of the fractures, represents a major problem in the surgical treatment of fractures of the distal third of the tibia and fibula. 10,11 In the current study, injuries of the soft tissue were evaluated from the start of hospitalization using the Tscherne soft tissue classification. For severe or unstable fractures, calcaneus traction with mannitol detumescence was performed, especially in cases, where the Tscherne soft tissue classification was evaluated as grade 2 or grade 3. The soft tissue condition was assessed every 24 h by surgeons, and the operation was performed after local wrinkles arose and bruising faded. Furthermore, diabetes mellitus, which is a preexisting risk factor leading to several postoperative complications, was well controlled before the operation. All surgeries were selective and the average duration from hospitalization to surgery was 3–12 days. No patient complained of numbness and tingling of the injured limb before surgery as the swelling subsided.
To our knowledge, the optimal treatment for distal tibial fracture remains controversial. 12 Recent studies have been carried out comparing various interventions for the treatment of distal tibial fractures. 13 –16 The ORIF, minimally invasive plate osteosynthesis (MIPO), and intramedullary nail (IMN) techniques are the three main treatment methods used. Some researchers demonstrate that IMN has a lower risk of wound complications and better functional improvement of the ankle than does ORIF and MIPO. 17,18 However, ORIF seems to be more advantageous in achieving anatomical reduction and decreasing knee pain. 17 In the study, some cases could be performed with MIPO procedure or intramedullary nail as well. ORIF with anterolateral plating has the advantages of anatomic reduction and articular fracture management, which are not the indications for MIPO or IMN. For those cases without articulation involved, surgeons could choose the appropriate technique based on their experience.
In the current study, the patient demographics in the two groups were homogeneous. As a result, the surgical outcomes were comparable between the two groups. The dual-incision approach is widely used due to its clear exposure and direct manipulation. However, the single-incision approach is also applicable to fractures of the distal third of the tibia and fibula, especially in types A1, A2, B1, and C1 distal tibial fractures, and type C1 fibular fractures, according to the AO classification system. 6 In fact, all types of distal tibial and fibular fractures in AO classification can be performed by the means of single-incision approach in our study. Several studies also have evaluated the feasibility of this approach in clinical practice. 5,6,19 –21 Shantharam et al. 6 first proposed the feasibility of single-incision treatment for the management of fractures, while Yu et al. 5 discussed the anatomical basis of an anterolateral approach for the distal tibia and fibula. Their measurements demonstrated an obvious muscle gap and nerve interface in the anterolateral lower leg, and the single incision could avoid the major blood vessels and nerves. In our study, the single-incision approach could also attain adequate exposure for subsequent operations. Furthermore, the superficial/deep peroneal nerve and anterior tibial vessels could be clearly revealed, allowing extra precautions to be taken. 22,23
In our study, the radiological deformity rates were comparable. The ankle function, as assessed by the Olerud–Molander Ankle Score, and ROM of dorsiflexion and plantar flexion were similar between the two groups. These results indicate that high reduction quality and satisfied ankle function could be achieved by both approaches. The patients would be encouraged to return to work depending on radiographic evaluation of bony consolidation and ankle function. However, there were fewer soft tissue-related complications, including skin slough, infection, nonunion, and delayed union in group 1 (5/45) than in group 2 (14/48). Two patients in group 1, who had diabetes and continued smoking after surgery, suffered delayed union. The patient was obliged to quit smoking and was hospitalized for glucose control and physiotherapy. In group 2, five patients suffered delayed union and two patients suffered nonunion of tibial fractures. Two cases of nonunion received surgical revisions. All the cases with nonunion and delayed union healed eventually within the following visits. In the study, skin slough occurred in eight patients. Three cases with severe skin sloughs in group 2 required removal of necrotic tissue (Figure 5) and covering of skin defects and the rest with minimal area along the incision were conservatively treated. Three cases of infection were found during the follow-up. All the patients received intravenous antibiotics and local debridement dressing. Fortunately, all patients with soft tissue-related complications eventually recovered without severe consequences. There were four cases of nerve injury in group 1 and one case in group 2. All of them suffered numbness around the lateral ankle and a stabbing pain in the lateral dorsum of the foot, though the swelling of the injured ankle subsided, which were considered to be intraoperative traction injuries of the superficial peroneal nerve. The patients greatly improved over the course of several months with conservative treatment. Four cases of nerve injury through single-incision approach occurred at the early stage of the study. We may consider the potential bias in the “learning curve” of the new technique.

A 67-year-old male in the dual-incision approach group showed deep wound necrosis around the anterior incision, which required flap surgery.
Although our statistical results showed that the overall complication rates between the two groups were comparable, there were significantly more soft tissue complications in group 2. This result was consistent with our hypothesis that the single-incision approach had less of an effect on the soft tissue. However, with regard to intraoperative exposure and traction, nerve injury should be specifically considered in the single-incision approach. Furthermore, internal fixation removal is another important issue in the single-incision approach. In the single-incision approach, exposure is insufficient due to adhesion, and nerve injury is more likely to occur. As a result, a further lateral incision for fibular fixation removal may be inevitable.
Due to the small number of patients and the short-term follow-up involved in our study, further research is needed. More patients should be enrolled and a long-term follow-up was required to establish the safety and efficacy of this single-incision approach in the long term.
Conclusion
The single-incision and dual-incision approaches were found to be comparable for the operative management of distal tibial and fibular fractures for the majority of measured clinical outcomes. Although the single-incision approach appeared to be superior for soft tissue conservation, the risk of nerve injury should be carefully considered, especially at the early stage of the learning curve. Despite this, the single-incision approach may be a reliable alternative to provide better soft tissue conservation in distal tibial and fibular fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.