
Abstract
Introduction
Fractures of the tibia and fibula occurring at the same level can be technically challenging. Fibular plating (FP) prior to intramedullary nailing (IMN) may facilitate tibial reduction, stabilization, and subsequent tibial healing. The primary goal of this study was to compare tibial fracture healing between FP and no fibular plating (NFP) in patients with same-level distal third tibia/fibula fractures.
Methods
Patients ≥18 years with distal third tibia/fibula fractures occurring at the same level were randomized to FP or NFP prior to infrapatellar IMN. Same-level fractures were defined as distal third tibia fractures with an ipsilateral supra-syndesmotic distal third fibula fracture. Intraoperative parameters, patient-reported outcome measures (PROMs), modified Radiographic Union Scale in Tibial fractures (mRUST) scores, radiographic alignment, and adverse events were recorded.
Results
30 patients were recruited, with 15 randomized to each group. There were no differences in baseline characteristics between groups. Total operative time was longer in FP compared with NFP (105.5 vs 65.8 minutes, p = .001). Mean duration of fibular fixation was 28.1 minutes (SD = 11.9). There was no difference in duration of IMN; however, less time was required to pass the guidewire in FP (4.5 vs 11.8 minutes, p = .01). Patients in FP had higher mRUST scores at 6 months, lower incidence of delayed union, and shorter fibular time-to-union. There were no differences in alignment between groups.
Conclusion
Fibula-first fixation facilitated passage of the tibial guidewire and resulted in a modest improvement in the rate of tibia fracture healing. The results of this pilot study suggest that fibula-first fixation may be beneficial in patients with same-level distal third tibia/fibula fractures. Further research with larger sample sizes is needed to determine which patients may benefit most from fibula-first fixation.
Introduction
Malunion, delayed union, and nonunion are common following diaphyseal tibia fractures, with up to 14% of patients developing nonunion and 50% of patients developing malunion.1,2 The presence of an ipsilateral fibula fracture increases surgical complexity and is associated with higher rates of malalignment and nonunion, especially when the tibia and fibula fractures occur at the same level.2–4 Management of the fibula fracture in patients with same-level distal third tibia/fibula fractures is controversial. The proposed benefits of fibular fixation include facilitating tibial reduction, maintenance of alignment, increased stability, and lower rates of nonunion; however, the evidence is mixed. Some authors report no benefit of fibular fixation regarding alignment,5–10 while others report improved coronal, sagittal, and/or rotational alignment.4,7,11–19 Likewise, some authors suggest that factors such as the presence of a fibula fracture, fracture pattern, use of multiplanar locking screws, number of locking screws, and static versus dynamic locking appear to be more important than fibular fixation in minimizing tibial malalignment.4,10,20 Early cadaveric studies demonstrated higher stiffness and load to failure with fibular fixation21,22; however, advanced nail designs allowing for multiple distal interlocking screws may provide equal, if not greater stability, compared with fibular fixation.9,23,24
Although the role of fibular fixation in maintaining tibial alignment is debatable, there is consensus that fibular fixation does not reduce the risk of tibial nonunion.8,11–14,16,25 Not surprisingly, fibular fixation reduces the risk of fibular nonunion from 27% to 0%, which can be a considerable source of discomfort for patients, with over 50% of these patients undergoing surgical intervention.26,27 Most studies have found no benefit of fibular fixation regarding patient-reported outcomes (PROMs)2,11–13,26; however, some authors report faster return to full weightbearing, greater range of motion, and higher American Orthopaedic Foot and Ankle Society (AOFAS) score and Olerud-Molander Ankle Score (OMAS). 15
Only three randomized controlled trials have evaluated the role of fibula-first fixation in patients with combined tibia/fibula fractures.7,8,28 Only one study reported intraoperative metrics, including operative and fluoroscopic time, reporting no significant difference between fibular fixation and no fibular fixation in patients undergoing IMN. 7 Furthermore, only one study specified their definition of nonunion, and none used a radiographic scoring system to quantify fracture healing.7,8,28
The goal of this study was to compare the effects of fibula-first plating (FP) versus no fibular plating (NFP) on intraoperative parameters, time-to-union, malalignment, and functional outcomes in patients with same-level distal third tibia/fibula fractures. Our primary outcome was rate of tibial union at 6 months postoperatively, defined by an mRUST score ≥13 with bridging of ≥3 cortices . We hypothesized that FP prior to IMN would not affect tibial union.
Methods
Study design
This study was a single-centre, randomized controlled pilot study at a Level-1 academic trauma center. Institutional research ethics board approval was obtained prior to study commencement (REB 22,495). Eligible patients were identified by members of the orthopaedic trauma service upon presentation to the emergency department. Eligible patients were approached by a member of the research team to discuss study participation and to complete the informed consent process.
Study population
Adult patients 18 years of age or older, with extraarticular fractures of the distal third tibia and fibula that occurred at the same level as each other and at or distal to the tibial isthmus were eligible for participation. Same level was defined as a distal third tibia fracture with a suprasyndesmotic distal third fibula fracture. Patients with severe open fractures (Gustilo-Anderson IIIB-C), syndesmotic injury, fractures at different levels, pathologic fractures, peri-implant fractures, or American Society of Anesthesiologists (ASA) class ≥ IV were excluded. Patients were randomized to treatment groups prior to surgery using computer-generated block randomization with stratification by ASA classification in a 1:1 ratio Figure 1. All patients were treated with a reamed, statically locked infrapatellar IMN and were randomized to FP or NFP groups prior to IMN. Fibular fixation construct was left to the discretion of the treating surgeon; however, all patients underwent lateral plating using either a 1/3 tubular, distal fibula locking plate, or mini-fragment plate with a minimum of two screws above and below the fracture Figure 2. All surgeries were performed by a trauma fellowship-trained surgeon, or under their direct supervision. CONSORT diagram demonstrating participant recruitment, randomization, and follow-up rates. Radiographic series demonstrating initial displacement (a), tibial reduction following fibula fixation (b), early callus at 3 months (c), and union at 6 months (d).

Data collection
Data collection was performed in the emergency department, inpatient units, and the cast clinic. Baseline patient demographics, including age, sex, body mass index (BMI), smoking status, alcohol consumption, substance use, comorbidities, medication use, ASA classification, pre-injury activity level, and occupation were collected. Injury characteristics including mechanism of injury (MOI), AO/OTA fracture classification, and Gustilo-Anderson classification were collected. Intraoperative outcomes included total operative time, duration of fibular fixation, duration of tibial nailing, time taken to pass tibial guidewire, duration of reaming, use of reduction techniques, use of fluoroscopy, and estimated blood loss. In-hospital outcomes included length of stay and perioperative adverse outcomes. Adverse events were recorded throughout the study period, including incidence of implant irritation, implant failure, implant removal, secondary surgery, venous thromboembolism, and infection.
Patients were followed at 2- and 6-weeks, and 3-, 6-, 12-, and 24-months postoperatively. Orthogonal radiographs were performed at each follow-up appointment and were evaluated by two independent reviewers. Reviewers were blinded to treatment group and interval from surgery. Radiographic blinding was accomplished by cropping the fibula out of the AP radiograph. Blinding to treatment group was not possible for the lateral radiographs. Coronal and sagittal alignment were measured in degrees and fracture translation was measured in millimeters (mm). Alignment was measured at 2 weeks. Coronal and sagittal malalignment were analysed continuously and categorically using cutoffs of ≥2° and ≥5°. Fracture healing was quantified using the modified Radiographic Union Scale in Tibial fractures (mRUST) beginning at 6 weeks postoperatively. 29 Union was defined as an mRUST score ≥13 with bridging of ≥3 cortices. Time-to-union was measured in months. Fractures that were not united by 6 months and 12 months were classified as delayed union and nonunion, respectively. Weightbearing status was recorded at each follow-up appointment. Patient-reported outcome measures (PROMs) were collected at each follow-up appointment, including pain visual analogue scale (VAS), the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale, and the Hospital for Special Surgery Knee Disability Scale (HSS-KDS).
Data analysis
Our primary outcome variable was fracture healing, defined using mRUST scores. Alignment and fracture healing were analysed as continuous variables (degrees, mm, mRUST, and time-to-union) and as categorical variables (≥2 and ≥5° deformity, union status at each follow-up, delayed union, and nonunion). Secondary outcomes included operative time, PROMs, complications, and fibular healing time-to-union. Independent samples t-tests were conducted for continuous variables. Chi-squared and Fisher’s exact tests were used to compare categorical outcome variables between groups. Effect sizes were calculated using Cohen’s d for continuous data and Phi for categorical data. Statistical analysis was performed using a combination of SPSS (IBM, Chicago, Ill., USA) and R (R Foundation for Statistical Computing, Vienna, Austria) software. A biostatistician assisted with the analysis. An alpha value of 0.05 was used to determine statistical significance.
Results
Participant baseline and injury-related characteristics.
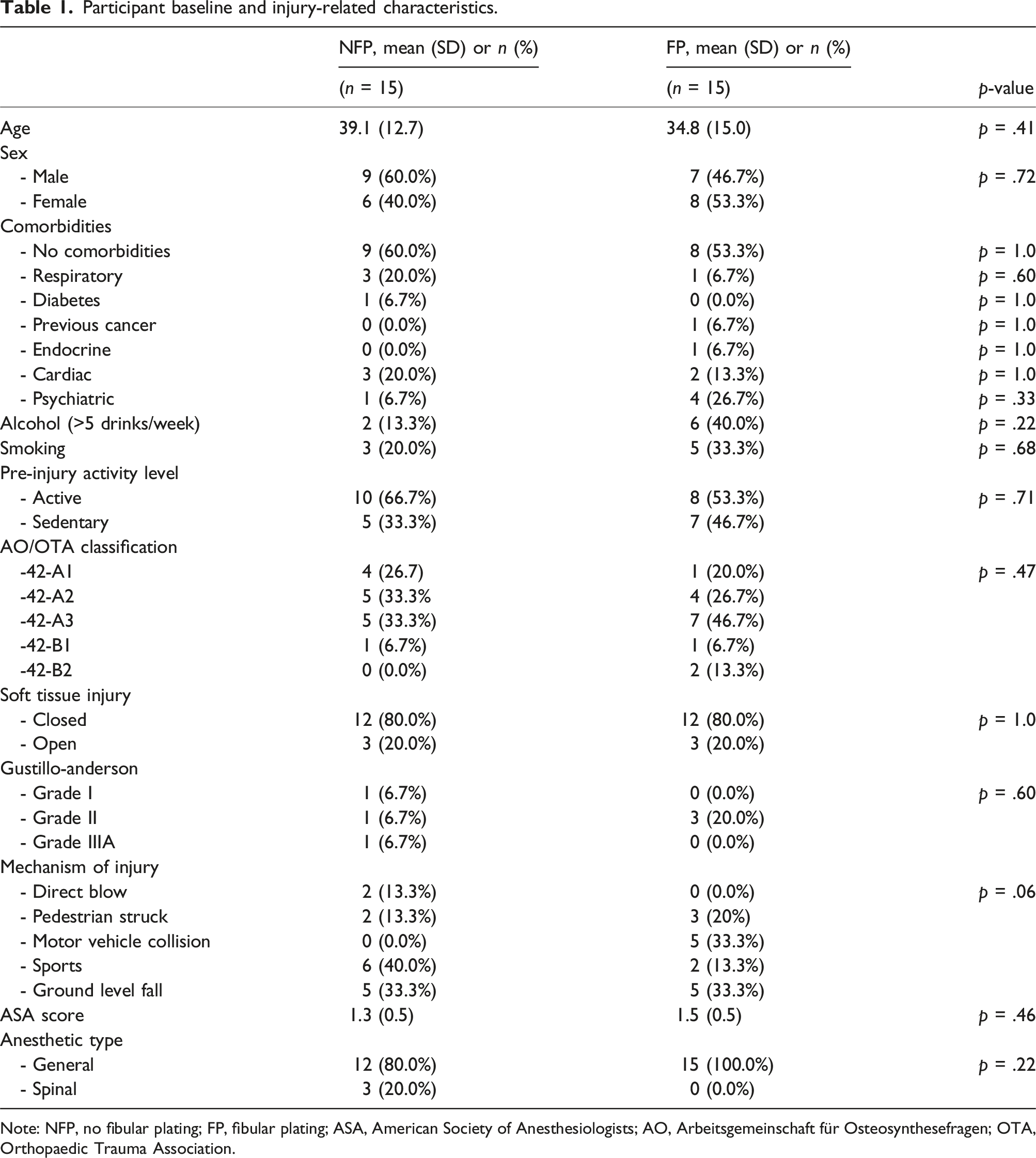
Note: NFP, no fibular plating; FP, fibular plating; ASA, American Society of Anesthesiologists; AO, Arbeitsgemeinschaft für Osteosynthesefragen; OTA, Orthopaedic Trauma Association.
Radiographic assessment of fracture healing.
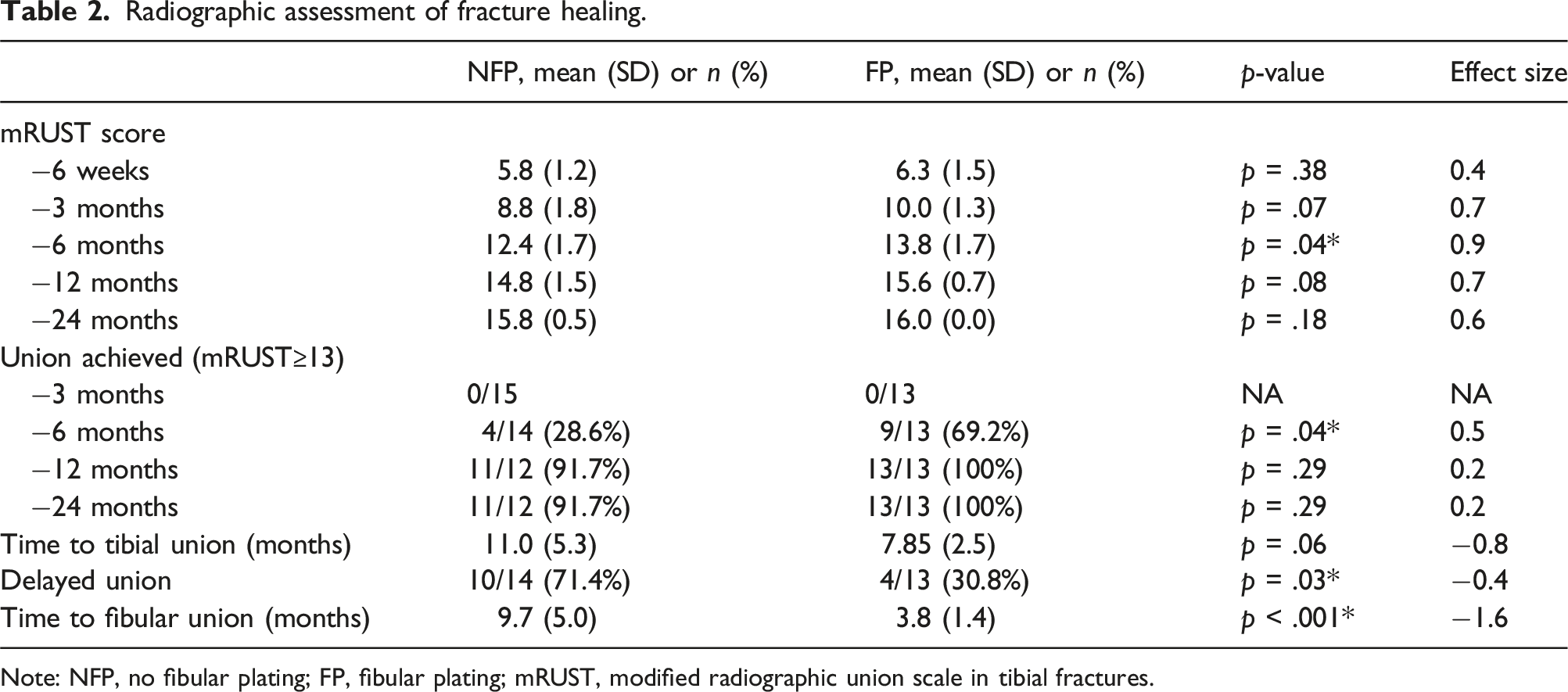
Note: NFP, no fibular plating; FP, fibular plating; mRUST, modified radiographic union scale in tibial fractures.
Intra-operative and peri-operative details.

Note: NFP, no fibular plating; FP, fibular plating; NWB, nonweightbearing; WB, weightbearing; WBAT, weightbearing as tolerated.
Radiographic assessment of fracture alignment at 2-week follow-up.

Note: NFP, no fibular plating; FP, fibular plating.
Summary of patient-reported outcome measures throughout the 24-month study follow-up.

Note: NFP, no fibular plating; FP, fibular plating; VAS, visual analogue scale; AOFAS, American Orthopaedic Foot and Ankle Society; HSS-KDS, Hospital for Special Surgery Knee Disability Scale.
Summary of complications.

Note: NFP, no fibular plating; FP, fibular plating.
Discussion
The role of fibula-first fixation in extraarticular distal third tibia/fibula fractures is controversial. The primary goal of this pilot randomized controlled trial was to evaluate the effects of fibular fixation on tibial fracture healing in patients with same-level distal third tibia/fibula fractures. There was a modest benefit in tibial fracture healing time, as shown by higher mRUST scores at 6 months and a lower rate of delayed union, and a considerable reduction in fibular time-to-union in patients who underwent fibular fixation. Similar to previous studies, we found no difference in fracture alignment in the coronal or sagittal planes. Fibular fixation resulted in a shorter time required to pass the tibial guidewire, but a longer total operative time. Patients in the fibular fixation group had higher pain scores at 6-week follow-up, but no difference in complication rates including infection, wound healing, or implant removal.
Time to union and the incidence of delayed union were quite high in both of our patient groups. Mean time to union was 11.0 and 7.9 months for NFP and FP, respectively, with corresponding incidences of delayed union of 71.4% and 30.8%. Our findings are similar to those of Mundi, et al., 30 who reported a mean time to union of 9.5 months, with only 26% of patients achieving union by 6 months. Numerous studies have demonstrated substantial variations in time to union and incidence of delayed union and nonunion in patients with tibia fractures.31,32 The large variations, and differences in definition of union, as well as the use of radiographic scores makes comparison between studies difficult.
Given the challenges of obtaining anatomic reduction of same-level tibia/fibula fractures in the meta-diaphyseal region, adjuncts such as percutaneous and open reduction are often needed. There is considerable disagreement among individual studies regarding the benefits of fibular fixation with respect to reduction of the tibia fracture. Although our study did not show any difference in the rates of closed versus percutaneous versus open reduction, we found that FP resulted in significantly shorter time to pass the ball-tipped guidewire, suggesting that FP likely aids in tibial reduction.
Previous studies have reported worse outcomes following fibular fixation, including higher rates of infection, revision surgery, and malalignment.6,14 In our study there was no difference in infection, implant removal, or alignment between patients in the FP and NFP groups, consistent with the majority of the literature.7,13–15,17,19 Regardless of management, the presence of a fibula fracture has been shown to result in an increased risk of tibial nonunion. 4 Previous studies have evaluated the effect of fibular fixation on tibial nonunion; however, they have either not used radiographic union scores or not provided their definition of nonunion.6,8,15,26 Some authors report no effect on tibial union, while others report lower 33 or even higher 14 rates of nonunion. Recent systematic reviews suggest that fibular fixation does not impact tibial fracture healing but does result in improved rotational alignment.3,13,16 There continues to be debate surrounding the effects of fibular fixation on coronal and sagittal plane alignment and rates of complications. Although our study looked specifically at same-level distal third tibia and fibula fractures we had similar findings with respect to alignment, although we did not examine rotational alignment. Unlike previous studies, our study used the mRUST score to quantify tibia fracture healing over time. Use of a radiographic score allowed us to more precisely assess healing and it likely responsible for the modest benefit with respect to rate of tibial fracture healing observed in the FP group.
Based on existing literature there is a lack of consensus regarding the role of fibular fixation in same-level distal third tibia and fibula fractures. The primary benefits appear to be a modest improvement in tibial alignment and fracture healing time, as well as improved rates of fibular union. This may come at the cost of a slight increase in the risk of infection,3,6 and the potential for delayed tibia fracture healing with supra-syndesmotic fibula fractures, as a result of the fixed fibula preventing compression across the tibial fracture 14 ; however, neither of these complications were observed in our study. Additionally, fibular fixation may increase the risk of tibial malalignment, especially with malreduction of a complex fibula fracture, 6 but again, this was not encountered in our study.
The strengths of this study include strict inclusion and exclusion criteria, a randomized-controlled design, long-term follow-up, and the breadth of intraoperative, perioperative, and long-term outcomes recorded. In contrast to previous studies, our use of a radiographic scoring tool (mRUST) allowed us to more accurately quantify healing over time, which facilitated comparison between groups. With the exception of operative time, previous research has not focused on intraoperative variables, such as reduction techniques required, ease of passing the guidewire, and reaming time. 15 This randomized-controlled trial is the first to evaluate these intraoperative variables. We found that fibular fixation resulted in less time required to pass the tibial guidewire, suggesting that fibular fixation aided in tibial reduction and provided inherent stability during the surgery. Despite the reduction in time to pass the wire, we did not show a difference in the use of closed, percutaneous, or open reduction techniques.
This study does have several limitations. Given that tibial nonunion occurs in up to 14% of patients, 1 our sample size of only 30 participants limits our ability to comment on the true effect of fibular fixation on nonunion. In order to reduce the burden on participants we chose to measure healing at standard clinical follow-ups. As a result, we are limited in our ability to accurately determine the exact time of union during the study follow-up. Multiple surgeons participated in this study, which may have affected our intraoperative measures, especially duration of operation. Although this is a limitation, this is the first study to evaluate the effect of fibular fixation on intraoperative metrics. Finally, use of three-dimensional computed tomography would have allowed more accurate quantification of alignment and healing and specifically allowed assessment of rotational alignment; however, this would expose patients to considerable additional radiation.
Conclusion
Fibular fixation resulted in a slight improvement in the rate of tibial fracture healing, and a considerable reduction in time to fibular union in patients with same-level distal third tibia/fibula fractures. Fibular fixation resulted in longer operative time, but significantly shorter time to pass the tibial guidewire. There were no differences in the incidence of complications including nonunion, infection, secondary surgery, or malalignment; however, patients in the FP group had higher postoperative pain scores at the 6-week follow-up. Our results suggest that fibular fixation may result in slightly faster tibial fracture healing and facilitates surgical fixation of the tibia in patients with same-level distal third tibia/fibula fractures. Further studies with larger samples sizes are needed to determine the clinical relevance of these findings and to help determine specific indication criteria for fibular fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.