
Abstract
Purpose:
Perioperative swelling and edema are the main factors that influence the time to definitive operative care, healing rate, as well as postoperative infection rate. Device-based negative pressure treatment is a new method to reduce post-traumatic and postoperative swelling of the upper extremities. The objective of this study was to evaluate a new negative pressure treatment with LymphaTouch® (Helsinki, Finland) to reduce perioperative swelling in upper extremity injuries.
Methods:
We analyzed 45 patients (26 female and 19 male) after operative treatment of upper extremity injuries. A predefined treatment algorithm of 30 min using LymphaTouch® was performed on the patients every day for five consecutive days. Swelling was measured according to the neutral-zero method with six points of measurement.
Results:
A total of 16 patients underwent an operation on their upper arm. An average of 3.5 measurements was performed per patient, with the start of therapy at a mean of 5.13 days after the operation. All of the measured circumferences except the elbow and 10 cm below the elbow were reduced from day 0 to 3. The percent reduction of swelling (relative to day 0) was 10.36%, 11.35%, 17.34%, and 3.25% for days 1–4, respectively. The greatest reduction of circumference was obtained in the metacarpus (−51.6%) and wrist (−33.1%).
Conclusion:
The LymphaTouch® system and a 30-min treatment program can reduce postoperative swelling of the upper arm, wrist, and hand on the first 5 days after surgery. The ease of learning and self-applicability of LymphaTouch® makes it interesting for further controlled randomized trials.
Introduction
Preoperative edema and swelling are limiting factors in surgical treatment, especially for injuries affecting extremities in which a local gain of circumference limits the time to definitive operative care. Due to the risk of infection and wound dehiscence, soft tissue swelling needs to be preoperatively reduced until fixation for tension-free wound closure, leading to an average delay of 7 days until definitive surgery. 1 –3 Reduction of perioperative swelling and edema has not been thoroughly examined, and prospective trials are rare. The only broadly conceived reviews and meta-analyses deal with lipedema, lymphedema, and treatment of cancer-related edema. 4 –6 Similarly to a preoperative gain of circumference, postoperative swelling increases the wound complication risk and infection rate, thus outlining a major dilemma in traumatology. Whether compression therapy or cooling is superior and whether the evidence for their superiority is sufficient still remains controversial. 7 –9 For adequate postoperative reduction of swelling, manual lymphatic drainage (MLD) is often performed, which lacks a satisfying basis of evidence since randomized controlled trials have failed to depict its effect on swelling, while pain and movement can benefit. 10,11 Due to the clinical impact of swollen upper extremities and the delay of operative treatment, we aimed to establish a therapeutic solution for painless and easy reduction of distended extremities. One factor that the health system permanently lacks is personnel, which is why innovative methods by which patients can complete physiotherapy and MLD on their own are desperately sought. 12,13
Subsequently, we aimed to develop innovative devices for simple, self-trainable, and safe swelling reduction perioperatively. After a Finnish negative pressure suction apparatus, LymphaTouch® (Helsinki, Finland), had revealed promising preliminary results, we decided to perform a prospective study using this device. 14
The objective of this prospective study was to determine whether the LymphaTouch® method was sufficient to reduce post-traumatic and postoperative edemas in the upper extremities after trauma and surgery on the upper limbs.
Ethics
The local ethics committee approved this study (DOK_185_2016).
Materials and methods
Patient cohort
Patients with pre- or postoperative swelling of an upper extremity who were admitted to our hospital (level 1 university trauma center) from 2016 to 2017 were prospectively (nonrandomized and nonblinded) investigated.
Inclusion criteria
The inclusion criteria were pre- or postoperative swelling of one extremity in comparison to the other, injury of one extremity, age >18 years, and written informed consent.
Exclusion criteria
The exclusion criteria were no possibility of informed consent, further injury (e.g. spine), MLD after operation, acute inflammatory disease (e.g. erysipelas), open wound, painful hematoma, acute eczema in the edema area, chronic lymphatic edema, acute phlebothrombosis/thrombophlebitis, tumor/malignoma in the region to be treated, decompensated cardiac insufficiency, advanced peripheral arterial disease, and acute severe asthma.
Measurements
After information was collected and photographic documentation, the circumferences were measured exactly at defined positions according to the neutral-zero method.
15
The upper extremities were measured in the sitting position with the arms hanging down. For documentation, the following circumferences were measured: CUA15: Upper arm, 15 cm below the humeral head (palpable tuberculum majus), CEJ: Elbow joint, CFA10: Forearm, 10 cm below the elbow joint, CWR: Wrist, CMC: Metacarpus, CFi: Greatest distance between first and fifth finger (width of one hand).
The measurements were carried out every day before treatment. The patients did not stay longer in hospital just for the treatments; in case of earlier discharge, the measurements were stopped.
Treatments
Patients were subjected to a standardized negative pressure treatment protocol with LymphaTouch® for half an hour post-traumatically or postoperatively (Figure 1). This program was carried out for a maximum of five consecutive days.

LymphaTouch® device for negative pressure therapy on upper extremities with changeable suction heads.
No patient who received LymphaTouch® treatment received additional MLD. Standardized active and passive physiotherapeutic treatment was allowed. Most treatments were performed within the first days after the operation/trauma.
LymphaTouch® treatment for upper extremities (Table 1): The protocol was designed in a bottomed-up approach with a rising intensity in either pressure or duration. The beginning with 1 min and a low intensity is at the point of most lymphatic glands (supraclavicular fossa region), followed by 1 min of low intensity in the armpit. After that, for 2 min, an 80–180 mmHg pressure around the shoulder is followed by a longer period of 3 min with the same pressure of the entire upper arm and ends with the highest pressure (preoperatively) of 50–150 mg in the elbow area. Additionally, the negative pressure treatment follows a clear path downwards from the supraclavicular fossa to the elbow (Table 1).
Treatment algorithm for LymphaTouch®.

Data analysis
Statistical analyses and graphical assessments were performed with GraphPad Prism (version 5.04, GraphPad Software, La Jolla, California, USA). After validation of the Gaussian distribution by the Shapiro–Wilk test, the t-test for parametric and Wilcoxon test for non-parametric distributions were performed. The level of significance was 5% (p < 0.05*, p < 0.01**, p < 0.001***). The data are shown as the mean values with the standard error of the mean (SEM).
Results
The collective consisted of 45 patients (26 female and 19 male), of whom 16 underwent an operation on their upper arm, 16 on their shoulder, 4 on their elbow, 7 on their forearm, and 2 on their hand (Table 2).
Distribution of patients who received a treatment of their upper extremities.

The average age of the patients was 63.30 years (±2.43), and the average number of measurements per patient was 3.53 (±0.14). On average, treatments were performed 5.13 (±1) days after the operation for five consecutive days.
Most patients were operated on their upper arm and shoulder, for which four treatment days could be achieved, with the longest number of postoperative days on hand-operated patients. The average number of days for LymphaTouch®-therapy was five (Table 2).
Regarding the swelling of the upper extremities, from day 0 to day 3, all circumferences were reduced (Table 3). On the final day (day 4), the circumferences of EJ (elbow), FA10 (forearm 10 cm below the elbow joint), and Fi (width of one hand) increased again relative to the day before, possibly due to the reduced number of measurement points (Tables 3 and 4).
Reduction of swelling of the upper extremities (all patients who received upper extremity operations).
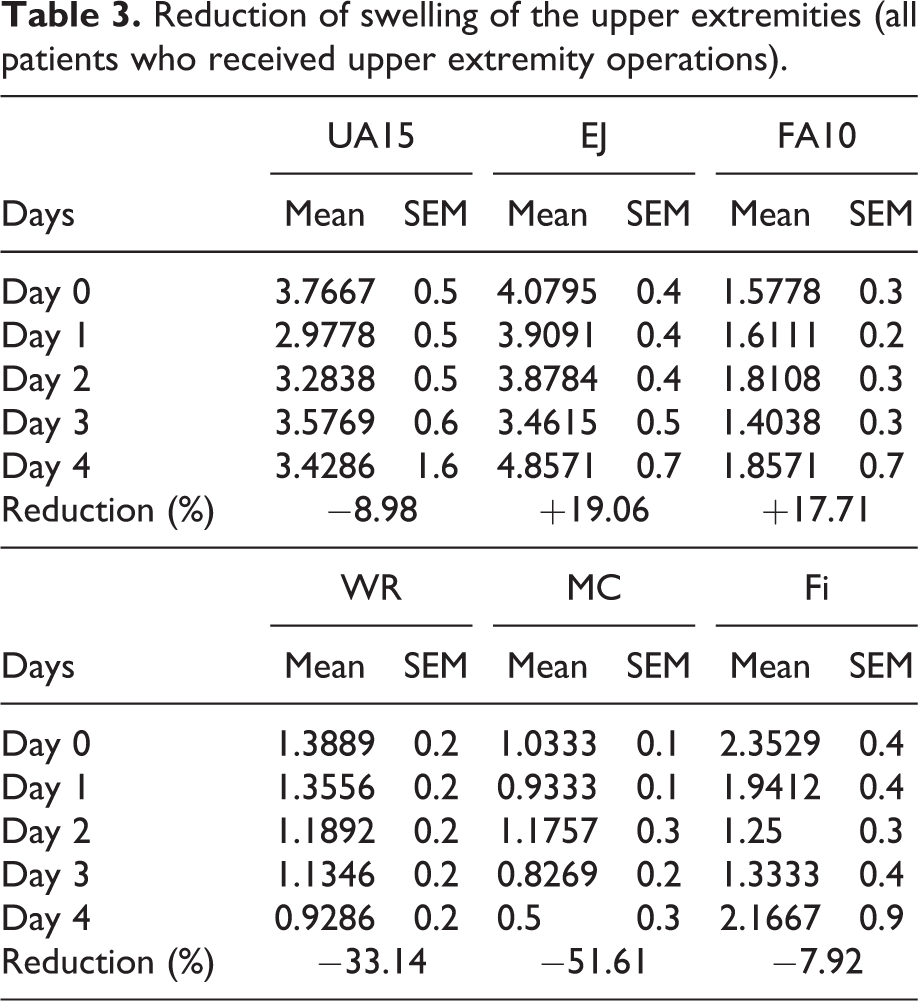
Results with the percent reduction of swelling relative to day 0..

UA15: upper arm; EJ: elbow joint; FA10: forearm; SEM: standard error of the mean; WR: wrist; MC: metacarpus; Fi: width of one hand. Overall, a reduction of circumference could be achieved. In relation to day 0 measurements, a reduction of 10.36% on day 1, 11.35% on day 2, 17.34% on day 3, and 3.25% on day 4 could be detected. The greatest reduction was seen on day 3, with a reduction of 17.34%. On the final day of measurement, the number of measured points was reduced by 84.11% to only 41 (whereas on day 0, 258 points were quantified; Table 4).
Discussion
Pre- and postoperative swelling as risk factor for wound dehiscence and infection remains a major clinical dilemma about operative treatment of the upper extremities. 16 The underlying causes of postoperative swelling are increased tissue pressure and consecutive ischemia with tissue necrosis and imminent compartment syndrome. 17 Hence, decongestant measures are urgently needed. In clinical practice, cooling and MLD are often conducted, and the former is based on several randomized controlled trails for knee or general joint arthroplasty. 18 –20 The latter is less standardized; for 3 days in the early postoperative period after total knee arthroplasty (TKA), MLD improved knee flexion and ankle girth postsurgery but not midpatella, thigh, or calf girth. 11 After five treatments of MLD, swelling was not significantly reduced after TKA, but the pain level was reduced immediately. 10
Generally, large meta-analyses or systematic reviews regarding postoperative swelling are rare, and the existing ones deal with lymphedema of the limbs. 21 In a retrospective analysis that included 286 patients, postoperative swelling was most pronounced on days 3–5 after TKA. 22 Based on this result, in the present study, treatment with LymphaTouch® was performed 5.13 days after surgery. Similar studies on the effect of vacuum-driven systems on swelling of the upper extremities are rare. For the reduction of preoperative swelling, the “A-V Impulse ‘in-cast’ system” has been demonstrated to be beneficial in prospective randomized controlled studies with 60 and 64 patients and is superior to cool packs for swelling of the lower extremities. 23,24 The superiority of pneumatic compression over ice and elevation was also demonstrated in another prospective study of 30 patients: 15 were randomized into splints, ice, and elevation and 15 received pneumatic pedal compression therapy for preoperative ankle fractures. The latter group decayed significantly faster than the splint/ice/elevation group. 25 Compression therapy after ankle fracture has a beneficial effect on edema reduction and pain, but whether the effect on wound healing and length of time is similar remains inconclusive after multiple reviews. 1,26,27
For reduction of acute and chronic swelling after trauma and surgery of the foot and ankle, a pneumatic intermittent impulse compression device was demonstrated to be effective. 28,29 We demonstrated that swelling of the overall upper extremity was mostly reduced on day 3, with a reduction of 17.34%. While the reduction of swelling was most pronounced on the upper arm, the wrist, metacarpus, and fingers, elbow and forearm could not be reduced in circumference after five consecutive treatments with LymphaTouch®. One possible explanation for this diverging effect in elbow and upper forearm could be the loss of follow-up. On day 3, 151 measurements have been done while on the fourth day, just 41 could be performed resulting in a greater variance (and a higher SEM on day 4).
To date, no comparable studies regarding the effect of negative pressure devices on perioperative swelling of the upper extremities have been published. The only randomized controlled clinical trial compared manual edema mobilization with the traditional edema technique on subacute hand/arm edema after a fracture of the distal radius and found no difference after 30 min of treatment for multiple weeks. 30 General manual lymph drainage, however, seems to be beneficial after external fixation of the hand/forearm. 31 This small prospective pilot study reveals the beneficial effect of 30 min of therapy on perioperative edema after operative treatment of the upper extremities.
Conclusions
Altogether, the measured circumferences except the elbow and 10 cm below the elbow were reduced from day 0 to 3 after treatment with the LymphaTouch® system. Further randomized controlled trials are necessary to dissociate the effects of the LymphaTouch® system from the natural course of detumescence and against MLD.
Footnotes
Declaration of conflicting interests
DS, A-CF, and WL declare that no conflicts of interest exist that could affect this article. Additionally, no funding was obtained to support this manuscript.
KD declares that after the study, he became a medical adviser for LymphaTouch®.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.