
Abstract
Isotretinoin, a vitamin A derivative, is known to induce premature epiphyseal closure. We report the case of a 9-year-old boy with neuroblastoma who demonstrated premature epiphyseal closure after 1 year of isotretinoin treatment (72.3 mg/m2/day). A bone bridge developed on the bilateral proximal tibial growth plate resulting in genu varum. We performed hemiepiphysiodesis on the bilateral proximal tibia in anticipation of the spontaneous resolution of the bone bridge. Genu varum on the left side was corrected with the resolution of bone bridge. For the remaining bone bridge on the right side, arthroscopy-assisted physeal bar resection was performed, and genu varum on the right lower extremity was also corrected. A regular review of the alignment of the upper and lower limbs is necessary to provide timely intervention in patients using isotretinoin, considering the possibility of premature epiphyseal closure.
Introduction
Isotretinoin is often used as the standard treatment for cystic acne and keratinization disorders. 1 It is also an effective anticancer drug that inhibits angiogenesis and oncogene expression of tumor cells and is used in pediatric cancer. 2 However, these systemic isotretinoin therapies are associated with acute and chronic toxicity. 2 In the 1940s, Caffey first described skeletal deformities that occurred after excessive vitamin A exposure in children. 3 If a premature epiphyseal closure occurs around the knee joint after administration of isotretinoin, angular deformity may occur in the coronal plane, such as genu varum or genu valgum, depending on the location of the bone bridge. 4 –7
Treatment may depend on whether growth remains. If growth is over, correction osteotomy may be required. If enough residual growth remains, resection of the physeal bar may be considered. 8 However, spontaneous resolution of the bone bridge has been reported in cases with residual growth. 9 –13 Correction osteotomy has been reported in a patient with complete growth for treatment of bilateral genu varum deformity following isotretinoin treatment of neuroblastoma. 4 However, treatment of the deformity after isotretinoin administration in patients with residual growth has not been reported.
We encountered a patient with residual growth presenting with bilateral genu varum deformity due to premature epiphyseal closure after neuroblastoma treatment using isotretinoin. We treated the case with hemiepiphysiodesis expecting spontaneous resolution of the bone bridge.
Case report
A 9-year-old boy was referred from the pediatric department owing to deformity of the lower extremity. On examination at the outpatient clinic, his height was 128.5 cm (17.8 percentile) and weight was 27.4 kg (21.7 percentile). He was diagnosed with retroperitoneal neuroblastoma with left humeral metastasis (stage IV) at the age of 6 years. He underwent four cycles of chemotherapy (cyclophosphamide, cisplatin, etoposide, and doxorubicin) and excision of retroperitoneal neuroblastoma. After surgery, he underwent additional chemotherapy using the same regimen. After 3 months of surgery, the first autologous peripheral blood stem cell transplantation was performed after the use of a conditioning regimen (topotecan, thiotepa, and carboplatin). Three months later, the second autologous peripheral blood stem cell transplantation was performed after the use of the conditioning regimen (melphalan, etoposide, and carboplatin). One month later, radiotherapy was performed on the abdomen and left humerus with 20 Gy and 10 fractions. Thereafter, subcutaneous interleukin 2 was injected 30 times with a 2-week interval. The patient then took 13-cis-retinoic acid (isotretinoin) 60 mg/day for about 1 year for tumor cell apoptosis.
On teleradiogram, the mechanical lateral distal femoral angle was in the normal range of 90.2° on the right side and 89.6° on the left side. However, the medial proximal tibial angle (MPTA) decreased to 76.5° on the right side and to 75.2° on the left side (Figure 1). On the anteroposterior radiographs of both knee joints, sclerotic changes were observed in the medial proximal tibia (Figure 2). Computed tomography (CT) revealed bone bridges on the bilateral medial proximal tibial growth plate (Figure 2). The size of the bone bridge of the bilateral medial proximal tibia was 1.3 × 0.4 cm2, similar in size and position. Multiple small bone bridges were seen in the bilateral lateral distal femur. In addition, magnetic resonance imaging (MRI) revealed a focal closure of the physis in the central portion of the left proximal humerus.

Teleradiogram of a 9-year-old boy treated with isotretinoin for neuroblastoma; genu varum is identified and the patient shows decrease in bilateral MPTA. MPTA: medial proximal tibial angle.

Anteroposterior radiographs and computed tomography imaging of bilateral knees: (a) white circles denote sclerotic changes in the medial proximal tibia And (b to e) white arrows show bone bridges on the right knee (b and c) and left knee (d and e).
Surgical treatment for genu varum correction was performed by hemiepiphysiodesis using a tension band plate (lockable hinge plate, BK Meditech Inc., Seoul, South Korea) on the bilateral lateral proximal tibia.
Fifteen months postoperatively, the patient’s height was 135.0 cm (12.7 percentile) and weight was 33.0 kg (23.9 percentile). MPTA was steadily decreased to 70.2° on the right side and improved to 90.2° on the left side, that is the genu varum on the left improved, while that on the right persisted (Figure 3). CT showed disappearance of the bone bridge of the medial growth plate on the left proximal tibia, but the bone bridge on the right side persisted with no change (Figure 4). Therefore, we planned for resection of the bone bridge on the right medial proximal tibia using arthroscopy-assisted physeal bar resection.
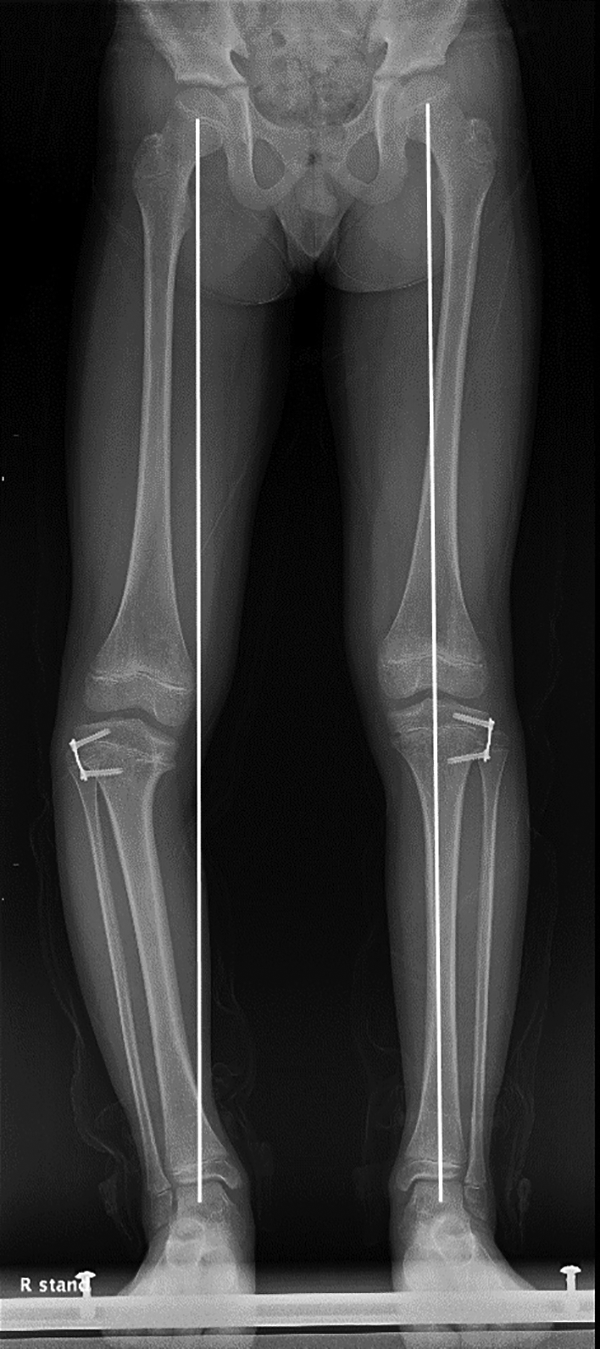
Fifteen months postoperative teleradiogram; genu varum on the left shows improvement but that on the right persisted.

Fifteen months postoperative computed tomography imaging: (a and b) bone bridge of medial proximal tibia on the right knee persisted and (c and d) bone bridge of medial proximal tibia on the left knee disappeared.
Surgery was performed using Langenskiold 8 and Peterson 14 techniques. Under general anesthesia, the bone bridge was identified using fluoroscopy, and a small incision was made in the metaphyseal area. A bur was used to approach the physeal bar and create a window through the physis. Thereafter, the cavity was checked with a 5-mm 30° arthroscope, and physeal bar resection was performed until the complete ring of cartilage was identified. 15 One year after physeal bar resection, genu varum on the right lower extremity was also corrected (Figure 5).

Twenty-nine months postoperative teleradiogram; the genu varum on both sides improved.
Discussion and conclusion
Premature epiphyseal closure is often caused by trauma to the physeal cartilage. 15 Rarely, vitamin A derivatives are known to cause premature epiphyseal closure. 3 –7 Retinoids bind to one or more retinoic acid receptors (RARs) and retinoid X receptors α, β, and γ, leading to premature epiphyseal closure by epithelial cell proliferation and differentiation. In addition, dose-dependent disruption of the proximal tibial epiphyseal plate was observed when RAR selective agonist was administered to guinea pigs. 16 In our case, a high isotretinoin dose, approximately 3 mg/kg//day, was administered, resulting in premature epiphyseal closure of the bilateral medial proximal tibia and lateral distal femur.
Chemotherapy may inhibit the proliferation of the growth plate chondrocytes leading to the growth plate thinning and longitudinal growth retardation. 17,18 In our case, the patient had a short stature (17.8 percentile), which might be due to chemotherapy. However, there has been no evidence regarding premature epiphyseal closure due to chemotherapy. Radiotherapy may also induce premature epiphyseal closure, as can isotretinoin. Ackman et al. reported physeal injury and genu valgum following radiation therapy after excision of epithelioid sarcoma on the right knee in a 5-year-old girl. 19 Matuszewskiand Rozbruch reported radiation-induced growth arrest in the pelvis and proximal femur after radiotherapy in a 22-year-old man who underwent surgery for rhabdomyosarcoma and in a 36-year-old man who underwent surgery for lymphoma. 20 In our case, metastasis of the left proximal humerus was confirmed by MRI, but premature epiphyseal closure was not initially observed. Radiotherapy of 20 Gy was performed in 10 fractions focused on the left humerus and abdomen. About 2 years later, MRI revealed focal closure of the physis at the central portion of the left proximal humerus. There were no abnormal findings in the right proximal humerus. Thus, the left proximal humerus was considered to have developed radiation-induced premature epiphyseal closure. On the other hand, we believe that the premature epiphyseal closure around the knee was due to isotretinoin because the knee joint did not undergo radiotherapy.
The presence of residual growth is an important consideration in premature epiphyseal closure as it influences the treatment choice. In our case, residual growth was present in a 9-year-old patient. Hence, we used a tension band plate for treating the genu varum deformity in anticipation of the spontaneous resolution of the bone bridge. Several studies have reported the correction of angular deformities due to the spontaneous resolution of the bone bridge in the distal tibia and proximal femur after trauma. Possible logical explanation for this is that persistent longitudinal growth of the surrounding normal growth plate induces distraction and breakage of the bone bridge. 10 –13 In our case, the spontaneous resolution of the bone bridge was observed on the left side, but not on the right. On the right side, we performed an additional arthroscopy-assisted physeal bar resection, and the varus deformity of both lower extremities was finally corrected. We believe that age and the size of bone bridge might be associated with spontaneous resolution of the bone bridge. However, so far, there has been no evidence to support this. Therefore, studies regarding the spontaneous resolution of the bone bridge and its associated factors are required. Physicians should be aware of the possibility of spontaneous resolution of the bone bridge without resection.
The effect of systemic isotretinoin therapy on bones usually appears over a long period. 21 Hence, skeletal deformities can be found after completion of growth, and more invasive treatments such as corrective osteotomy and distraction osteogenesis may be required. 4 Besides, late diagnosis results in the progression of angular deformity and development of a short stature. Therefore, the alignment of extremities should be closely monitored in pediatric patients using isotretinoin.
In this study, we reported a case in which a 9-year-old boy was successfully treated for bilateral premature epiphyseal closure due to isotretinoin by hemiepiphysiodesis and physeal bar resection. A regular review of the alignment of the upper and lower limbs is necessary to provide timely intervention in patients using isotretinoin, considering the possibility of premature epiphyseal closure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Written informed consent was obtained from the patient and his parents for this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT) (No. NRF-2019R1C1C1010352).