
Abstract
Background:
Juvenile hallux valgus (JHV) frequently results in an impaired quality of life because of pain and deformity. We used a validated clinical score to investigate the efficacy of lateral hemiepiphysiodesis of the first metatarsal base as a treatment for JHV.
Methods:
We conducted a prospective, nonrandomized, single center cohort study of children who underwent lateral hemiepiphysiodesis for 31-IV, with a clinical and radiologic follow-up of at least 2 years. The efficiency of the procedure was assessed with the Hallux Metatarsophalangeal Interphalangeal Scale (HMIS), the metatarsophalangeal angle (MPA), and intermetatarsal angle (IMA).
Results:
Twelve patients (22 feet) with JHV were treated by lateral hemiepiphysiodesis between 2012 and 2015. Average age at surgery was 10 years, and average follow-up was 3.5 years. The average HMIS score increased from an average of 56 at baseline, to 92 at last follow-up (p < 0.01). The average IMA decreased by 2°, from 13° preoperatively to 11° postoperatively. Average MPA decreased from 26° at baseline to 22° after surgery. No complications occurred in the immediate postoperative period, and no patient needed an additional procedure.
Conclusion:
The HMIS score was significantly improved after lateral hemiepiphyslodesis, with a clear improvement in pain and functional impairment at last follow-up. We noted a stabilization of the IMA and MPA, but the radiologic benefit did not reach statistical significance. Our data support the use of lateral hemiepiphysiodesis as an effective and safe treatment of JHV.
Keywords
Introduction
Juvenile hallux valgus (JHV) or bunion is a structural deformity in children of the first metatarsophalangeal joint with lateral deviation of the great toe and medial deviation of the first metatarsal bone. The etiology of hallux valgus is believed to be multifactorial in adults, but in juveniles, the marked preponderance of girls and the presence of a positive family history in two-third of cases suggest the influence of genetic factors. 1 –3
JHV can impair participation in recreational activities and affect quality of life because of pain, cosmetic deformity, and inability to fit some shoes in this young population. Numerous nonoperative and operative techniques have been described to treat hallux valgus in adults, 4 –7 but only one procedure has been proposed especially for JHV. Davids et al. first described lateral hemiepiphysiodesis of the first metatarsal in 1996 based on the well-known principle of intervention on the growth plate to obtain correction of skeletal deformity over time. 4,8 –11 To the best of our knowledge, this description of the technic is the only study reporting hallux valgus angles measurements. 9
The purpose of our study was to assess the efficacy of lateral hemiepiphysiodesis as a treatment for JHV using the Hallux Metatarsophalangeal Interphalangeal Scale (HMIS) and JHV angle measurements as primary outcome measures.
Methods
This prospective, single center, case cohort series included all children who underwent lateral hemiepiphysiodesis for JHV by one surgeon at our hospital, with a minimum follow-up of 2 years. All had pre and postoperative X-rays. Patients who underwent other operations for JHV were excluded. Surgery was offered to patients aged between 6 years and 12 years only, who complained of painful metatarsophalangeal first joint, with a mean daily Visual Analogic Scale of at least 4 of 10, and inability in sport activities. On the X-ray evaluation, the physis of the first metatarsal bone had to be open, signifying there was much bone growth expected until skeletal maturity, and the metatarsophalangeal angle (MPA) had to be at least 15°. If the patient complained of both feet, a bilateral procedure was offered.
To clinically assess the efficacy of the operative procedure, every patient was evaluated before the surgery by the operating surgeon, and at last follow-up by another clinician who did not take part in surgeries. The outcome measure was based on the American Orthopedic Foot & Ankle Society (AOFAS)—HMIS score which is a validated score used in forefoot pathologies. This objective score is composed of both objective and subjective criteria, as it assesses pain (40 points), function (45 points), and alignment (15 points). 12 –15 A general questionnaire administered at final follow-up included questions about reoperation and recurrence, whether the patients would recommend their treatment to others (Yes or No), and patient satisfaction from “very unsatisfied” to “very satisfied.” We also recorded postoperative complications such as severe pain, infection, hematoma, and excessive scar formation.
All patients agreed to take part in the study, and the parents of all patients provided oral and signed consent for the use of the collected, anonymous data in a scientific report. The signed consent of both parents was delivered after they had read an information document approved by the Institutional Review Board.
The pre- and postoperative X-rays were used to assess the extent of anatomic correction. The following angles were measured once by two independent radiologist, and the average of their measure was considered: the intermetatarsal angle (IMA) is the angle between the axis of the first and the second metatarsal bones, the MPAs defined as the angle between the axis of the first metatarsal bone and first phalange of the hallux, both being usual angles used to assess hallux valgus severity according to the AOFAS guidelines, the proximal metatarsal articular angle (PMAA) and the distal metatarsal articular angle (DMAA) defined, respectively, as the angle between the axis of the first metatarsal bone and the proximal and distal articular surface of the bone. 1,14 –17 Angle measurements were repeated three times by each radiologist, and the average of their measures was reported. At last follow-up, increased IMA and MPA angles were related to higher deformity and worse radiological result. Patients were evaluated 1 and 3 months after surgery and at yearly intervals thereafter. The results presented thereafter are those of the last clinical and radiological evaluation, with at least 2 years of follow-up.
Operative technique
The procedure was performed as described by Davids et al. 9 under general anesthesia. Fluoroscopy was used to localize the physis of the first metatarsal bone and its orientation. A tourniquet was used to minimize bleeding during the procedure. A 1-cm longitudinal incision was performed, centered over the lateral aspect of the physis. Dissection was carried down to the periosteum level with a Kelly clamp, to protect the anatomic elements in the soft tissue over the bone. A guide wire was placed on the lateral margin of the physis, guided by fluoroscopy. A drill and a curette were used to remove the lateral perichondrium and about 30% of the lateral portion of the physis (Figures 1 and 2). The incision was closed with simple skin sutures. A compression dressing was applied postoperatively for 1 h. No postoperative immobilization was required, and full weight bearing was allowed immediately. Crutches were prescribed if needed, for up to 1 week. Non-opiate analgesics were provided as needed.

Anteroposterior intraoperative fluoroscopy showing the curette ablating the lateral part of the physis.
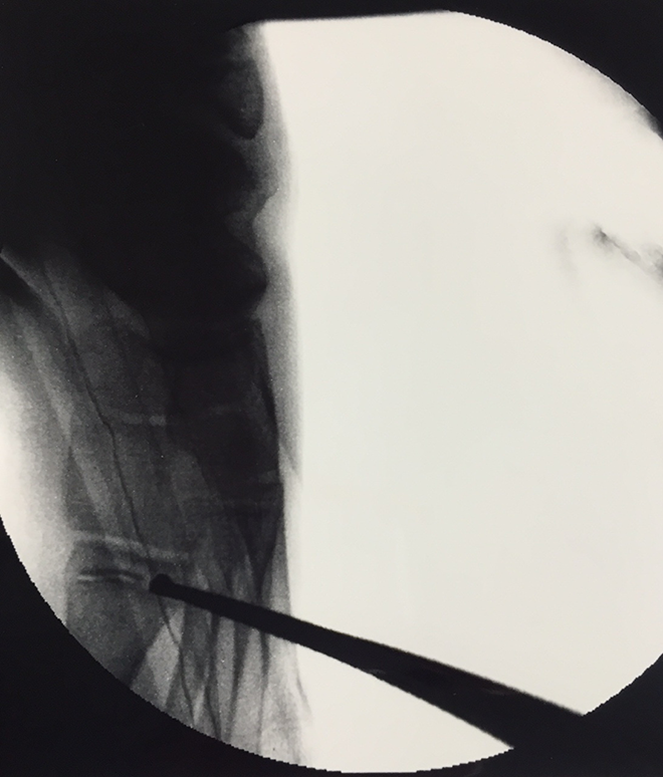
Lateral intraoperative fluoroscopy.
Statistical analysis
Data were analyzed with XLSTAT (Addinsoft 40, rue Damrémont 75018, PARIS). Statistical significance was defined as a p value less than 0.05. The unpaired Student’s t-test was used to compare the average values of functional outcome and radiological angles before surgery and at last follow-up.
Results
Twelve patients, eight girls and four boys, were treated by lateral hemiepiphysiodesis between January 2012 and January 2015 and followed for at least 2 years. The average age at surgery was 10 years old (9–12 years old). The average follow-up was 42 months (24–60 months), none was lost to follow-up. Ten of twelve patients (83%) presented with bilateral JHV, and among those who needed bilateral treatment, 9 (90%) had surgery on both feet in a single procedure. Therefore, 22 procedures were performed on 12 patients.
We observed significant improvement following surgery in the HMIS at last follow-up (Table 1). Average postoperative HMIS was 92 (83–100), compared to an average preoperative HMIS of 56 (49–67). The average gain on the HMIS was 36 points (p < 0.05). No patient had a lower HMIS score after surgery. Eleven patients (92%) were “very satisfied” with the procedure and 1 “satisfied.” All patients stated they would recommend the surgery to other patients.
Preoperative and postoperative HMIS score.

HMIS: Hallux Metatarsophalangeal Interphalangeal Scale.
No serious complications (hematoma, infection, fracture, and scar issues) were reported, and no patient needed additional procedures.
Analysis of the radiological criteria (Table 2) showed a mild improvement in both the IMA and MPA angle. Average improvement was 2° for the IMA and 4° for the MPA with no statistical significance for both angles. However, angles did not increase in any patient. Furthermore, PMAA and DMAA were stable over time with no statistical difference between the preoperative and last follow-up measures.
Radiologic outcomes.

MPA: metatarsophalangeal angle; IMA: intermetatarsal angle; DMAA: distal metatarsal articular angle; PMAA: proximal metatarsal articular angle.
Discussion
The purpose of our study was to assess the efficacy of lateral hemiepiphysiodesis as a treatment for JHV.
Percutaneous epiphysiodesis has been used since 1980 to correct bony deformities on long bones, as described by Bowen and Johnson. 18 The procedure is designed to induce asymmetric growth of the first metatarsal prior to puberty, which corrects the deformity because of residual growth. As this procedure is based on modifying bone growth, timing of surgery is crucial, and efficiency of epiphysiodesis should be evaluated at end of growth. The sooner the procedure is performed, the more correction you can expect.
In our series, surgery was proposed when the pain resulted in an impaired quality of life. Our patients had an average age of 10 years at surgery. This is younger than what would be suggested by the algorithm described by Green et al., based on the age, sex, and first metatarsal length. 19 Following their planification methods, the optimal time for surgery would be approximately 3 years later than ours. However, since all our patients presented an impaired daily life, and regarding our radiological results postponing the surgery would probably have led an insufficient result. In fact, as correction relies on bone growth, the later the procedure is performed, the less correction is to be expected since there is not much bone growth yet to come. In our series, end of foot growth was reached for most of our patients, considering that foot growth ends at the age of 14 years for girls and 16 years for boys. 20
Age and bone maturity were key point when identifying the patients who will benefit the most from the procedure. The principle of deformity correction with hemiepiphysiodesis lays on the residual bone growth. Surgery was offered to patients who had not reached skeletal maturity: 6–12 years old at maximum, with an open first metatarsal physis. Thus, deformity correction could be expected from those patients. Older patients, who had reached bone maturity presenting with a painful hallux valgus, were offered conventional hallux valgus surgery if necessary: scarf or chevron osteotomy. 3,7
The results reported in this series are comparable with previous published data for the same technique or other standard procedures such as scarf or chevron osteotomy and soft tissue release procedures. 1,3,14,17,21,22
We report a significant clinical statistical improvement on the HMIS score (AOFAS official scale for assessing forefoot pathology). Significant improvement was observed on pain and function sub-scores of the HMIS score (p < 0.05).
Alignment improved slightly but with no statistical significance (Figure 3). In our cohort, the main benefit from the procedure was functional, consistent with the prior report by Davids et al. 9 (average improvement of 2.3° on the IMA and 3.5° on the MPA). IMA and MPA improved in 55% of their feet, with no case of worsening angles. Regarding pain, in their series, no patients complained of the first metatarsophalangeal pain, but they did not use a validated score to assess the clinical result of the procedure. In our series, no patients reported increasing foot pain postoperatively and only one child with the highest pain score prior to surgery reported moderate pain in the joint with exercise.
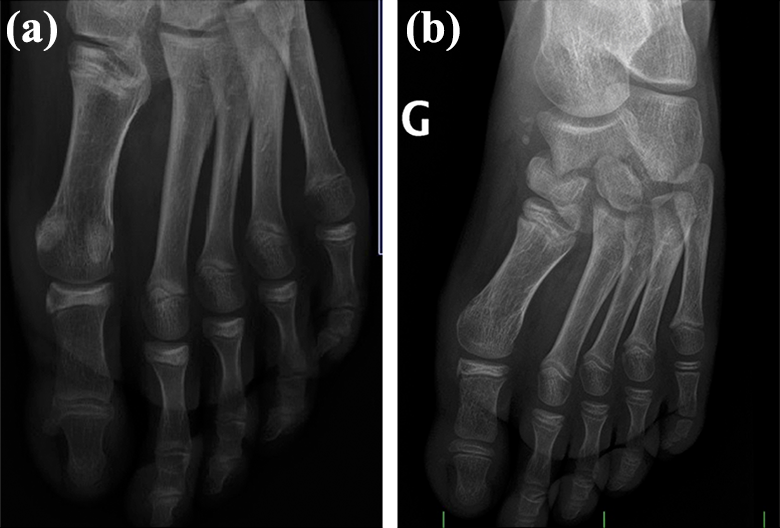
Pre (a) and postoperative (b) X-rays of a male patient operated at 8 years old. Preoperative MPA and IMA were 26° and 10°, respectively. Postoperative MPA and IMA were 17° and 4°, respectively. MPA: metatarsophalangeal angle; IMA: intermetatarsal angle.
Even though functional score improved significantly and that radiologic measures did not worsen over time, the deformity correction was not significant in our series. In JHV, the asymmetrical growth of the first metatarsal bone creates high asymmetrical constraints on the metatarsophalangeal joint, especially in the lateral part, responsible for the pain. After surgery, bone growth in the lateral part of the first metatarsal bone is supposed to be stopped. Thus, the pressure on the first metatarsal joint is distributed more evenly between the lateral and medial parts of the articular surfaces, decreasing the pain. This explains how we obtained a clinical improvement, without a significant radiologic correction.
Several reports of osteotomies procedures performed on adults or kids have reported slightly better radiological results than ours. 2,3,7,9,14,15,21,23 Jeuken et al. obtained an average improvement of 5° and 11° for the IMA and MPA, respectively, with the chevron osteotomy, and an average improvement with the scarf osteotomy of 4° and 7° for the same angles. 23 In these procedures, bony correction is performed under direct vision during the procedure allowing the surgeon to achieve the desired correction more easily.
However, high recurrence rates of up to 70% following osteotomies have been reported. 9,19,23,24 In contrast, our results improved over time and eventually stabilized once skeletal maturity was reached. Although we did not achieve a significant correction of the angles, we had no patient presenting worsening of deformity. Finally, the hemiepiphysiodesis at least prevents worsening of the angles in JHV. No patient needed additional procedures for hallux valgus correction at the last follow-up. However, we plan to follow our patients into adulthood since our follow-up is not long enough to exclude eventual late-stage recurrence.
Moreover, on the opposite of osteotomy procedures, being cause of a high rate of complication (delayed union, stress fractures, secondary tilt of the first metatarsal, persistent dorsiflexion due to postoperative soft tissue contracture, or excessive shortening of the first metatarsal), 6,17 lateral hemiepiphysiodesis is a percutaneous procedure and the rate of soft tissue or bone complication is lower. No postoperative complication of any type occurred in our series, supporting the overall safety and efficiency of this procedure.
The only potential pitfall in our approach is that if an insufficient portion of the growth plate is fused, the outcome may be suboptimal (Figure 4). Therefore, we recommend intraoperative monitoring with fluoroscopy to assure ablation of 30% of the growth plate.

Pre (a) and postoperative (b) X-rays of a female patient operated at 9 years old. The correction obtained and the rate of physis fusion are higher on the right foot.
Conclusion
Lateral hemiepiphysiodesis is a simple and effective treatment for JHV, providing significant pain relief and cessation of progression of the JHV. Functional improvement and patient and parental satisfaction were high, suggesting that this procedure can be widely recommended in JHV.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.