
Abstract
Purpose:
Total hip arthroplasty (THA) for high-riding hips is a complex procedure and the requirement for subtrochanteric osteotomy (STO) is an important decision that needs to be taken preoperatively. STO renders this complex surgery even more complicated and there are no guidelines to determine the STO requirement. In this study, the outcomes of THA for patients with high-riding hips were evaluated and a practical classification system is proposed to predict any osteotomy requirement.
Methods:
A retrospective evaluation was made of 79 hips of 76 patients who underwent THA for high-riding hip dysplasia. The amount of shortening in patients with STO and in patients without STO was compared. All patients were evaluated in respect of Harris hip score, operating time, erythrocyte suspension need, and actual limb length discrepancy. Preoperative radiographs were classified into four types according to the ratio of the distance between the lesser trochanter and the ischial tuberosity with pelvic height (LT-IT/P) to grade the degree of dislocation.
Results:
The mean follow-up was 30 ± 6.54 months. STO was applied to 47 (60%) hips and not to 32 (40%). There was no statistically significant difference between the groups in respect of the functional scores. STO prolonged the operating time and increased the need for blood transfusion (p = 0.026, p < 0.001, respectively). When the LT-IT/P index was <0.19 (type 1), no additional surgical approach was required for reduction, at 0.19–0.29 (type 2), the head can be safely reduced with additional reduction methods, and when >0.3 (type 3), a shortening osteotomy will most likely be required. The rate of complications is increased if LT-IT/P is >0.4 (type 4).
Conclusion:
STO adjunct to THA increases the rate of complications. This practical classification system may guide the surgeon in the decision of whether an STO should be added to the procedure or not.
Level of evidence:
Level III, clinical trial
Introduction
Total hip arthroplasty (THA) for high-dislocated hips is relatively more vulnerable to complications as a result of structural and biomechanical alterations such as muscle abnormalities, femoral deformities, and hypoplastic acetabulum. 1,2 Simply, the severity of dysplasia can be divided into two forms, which are high-centered or high-riding hips. High-centered hips have an oval and wide opening but a shallow acetabulum with near normal femoral morphology. THA with minimal modifications can be easily performed on these hips with secondary coxarthrosis. However, in high-riding hips, severe acetabular femoral morphological anomalies make THA more technically demanding. The classification system described by Jawad et al. is a relatively practical method to determine the degree of dislocation, in which types I and II are high-centered and types III and IV are high-riding hips. 3 It is the most commonly used classification system for dysplastic hips. More recently, Hartofilakidis et al. proposed a new classification using 3D computed tomography, which addresses the main limitation of the Crowe system, which is that acetabular deficiencies seen during surgical exposure cannot be detected. 4
It is widely accepted that THA for high-centered hips is less complicated, whereas THA for high-riding hips is more technically demanding. 5,6 For all Crowe types, implantation of the acetabular cup into the true acetabulum yields the best long-term functional results with lower rates of loosening due to relatively sufficient bone stock and optimal biomechanics. 7,8 However, many studies have mentioned the difficulty of reduction after placement of the acetabular cup into the true acetabulum because of considerable limb lengthening. 9,10 It is well-established orthopedic common sense that femoral shortening by subtrochanteric osteotomy (STO) not only facilitates the reduction and limb equalization but also restores the abductor lever arm and avoids iatrogenic nerve injury. This last point is particularly cogent as surgeons prefer a shortening osteotomy to be able to avoid sciatic nerve palsy, which has been well-documented in deleterious postoperative outcomes, especially when >4 cm of lengthening is predicted. 11 However, some surgeons avoid STO as an adjunct to THA in such patients because of the risk of nonunion, the prolonged operating time and increased bleeding, thigh pain, and conditions that can have a negative effect on the survival of the femoral stem. 12 –14 Rather than STO, these surgeons prefer methods, such as lowered neck osteotomy and lesser trochanteric cracking, pancapsular hip release, or iliopsoas and adductor tenotomies to facilitate the reduction.
The decision of whether to perform STO is crucial and has not really been addressed by the existing classifications. The complex procedures for reduction and positioning the acetabulum can also be difficult. Therefore, this retrospective clinical study was planned to investigate the clinical outcomes and complications of THA in high-riding hips and to devise a classification system, which would be able to guide STO requirement based on preoperative radiological characteristics.
Methods
Patients
Approval for the study was granted by the Institutional Ethics Committee. A retrospective examination was made of patients who were applied with THA for high-riding hip between 2013 and 2018 in our clinic. The study initially included 84 patients diagnosed as Crowe types 3 and 4, with at least 1 year of follow-up. A total of eight patients were excluded because of previous surgery to the same hip (n = 3), severe contracture (n = 4), and exitus of one patient because of vascular injury. Thus, evaluation was made of 79 hips of 76 patients with complete data of clinical evaluations, surgical records, and postoperative clinical and radiographic examinations. The patients with STO were compared with the patients without STO in respect of functional results, operating time, amount of erythrocyte suspension replacement, amount of leg lengthening and true limb length discrepancy (LLD), and complications.
Clinical evaluation
The postoperative clinical results of the patients were evaluated using the Harris hip score (HHS). By measuring the distance between the spina iliaca anterior superior and the medial malleolus, the amount of leg lengthening and the true LLD were determined. The duration of surgery, the amount of erythrocyte suspension replacement, and postoperative functional LLD were recorded. Infection, dislocation, vascular nerve damage, and nonunion were recorded as complications.
Radiological measurements
Two fellowship-trained orthopedic surgeons evaluated both preoperative and postoperative radiographs and limb length measurements. For intraobserver reliability, radiographs were reassessed at a 4-week interval. Preoperative radiographs of the patients were classified according to the Crowe and Hartofilakidis classifications, which were A-P graphs that were taken after placing discrepancy blocks under the short extremity. In patients with STO, the amount of shortening was evaluated and in patients without STO, the need for an additional reduction method (lowered neck osteotomy, controlled femoral cracking) and the change in the center of acetabular rotation were questioned. The presence of a high center of rotation was evaluated by measuring the distance between the teardrop and the center of rotation, and positivity was accepted as >35 mm. 15
Definition of new classification
Preoperative radiographs were assessed and classified to grade the degree of dislocation. This was evaluated by calculating the ratio of the distance between the lesser trochanter and the ischial tuberosity with pelvic height ((LT-IT)/P; Figures 1 and 2), and patients were divided into four groups according to the ratio: type 1: ≤0.2, type 2: 0.21–0.3, type 3: 0.29–0.39, and type 4: >0.4.

The measurement method of LT-IT/P index. LT-IT: the distance between the apex of the lesser trochanter and the ischial tuberosity; P: vertical height of the pelvis.

A female patient with bilateral high developmental hip dysplasia. Right-side Crowe type 3 pelvis with a type 2 dislocation (LT-IT/P index of 0.23) treated without STO and left-side Crowe type 4 pelvis with a type 3 dislocation (LT-IT/P index of 0.32) treated with STO. (a) Preoperative radiograph and (b) postoperative radiograph. LT-IT: the distance between the apex of the lesser trochanter and the ischial tuberosity; P: vertical height of the pelvis; STO: subtrochanteric osteotomy.
Surgical technique
Preoperative provision for shortening was made for Crowe type 4, Hartofilakidis type C, and patients with >4 cm determined on templating. The operations were performed on a radiolucent operating table with the patient in the supine position under general anesthesia and using a direct lateral approach. A cementless press-fit acetabular cup was implanted into the true acetabulum and for additional rotational stability, fixation was augmented with two or three screws. A 40- to 50-mm acetabular cup with a 22-, 28-, or 32-mm femoral head was used. The requirement for STO and shortening were checked again intraoperatively by examining soft tissue tension under traction and the relationship of the true acetabulum to the femoral head. If required, the distance between two overlapped osteotomized segments determined the amount of shortening. The femoral stem was implanted after splitting the osteotomized segment into two parts and fixation of this segment with two cables as an intercalary graft around the osteotomy site. A distally fluted cementless, proximally porous-coated femoral stem with hydroxyapatite coating was used in patients with STO (Secur-Fit Plus Max Femoral Hip Stem, Stryker Orthopaedics, Mahwah, NJ).
For the patients without a need for STO, the additional reduction methods were applied as required, including lowered neck osteotomy and/or controlled femoral cracking after the application of a single prophylactic cable immediately below the osteotomy. Following reduction, joint range of movement and the relationship of the tensor fascia with the iliopsoas were evaluated again. In cases with over-tension, tensor fascia release and iliopsoas release were performed. A Taperloc stem (Biomet, Warsaw, Indiana, USA) was used in the patients without STO.
Follow-up
Patients were mobilized on postoperative day 1. The patients without STO were mobilized with partial weight-bearing on the first day and full weight-bearing was permitted at the end of the first month. Patients with STO were mobilized with nonweight-bearing on postoperative day 1, were permitted partial weight-bearing after the first month, and full weight-bearing was permitted at the end of 3 months if full union was obtained.
Statistical analysis
Data obtained in the study were analyzed statistically using SPSS v.22 software and at a confidence interval of 95%. Qualitative data were stated as frequency distribution and quantitative data were stated as mean, minimum, and maximum values. Interobserver and intraobserver reliability were assessed using the interclass coefficient. The HHS values of patients with and without STO were evaluated with the Mann–Whitney U test. The complications of the groups were compared using the χ 2 test. In the evaluation of the HHS, according to additional surgical procedures, the Kruskal–Wallis test was applied. The correlation between the LT-IT/P index and the surgical application was assessed with frequency distribution and the Spearman’s correlation test.
Results
The patients comprised 71 females and 5 males with a mean age of 54 ± 9.04 years. The mean follow-up period was 30 ± 6.54 months (range 12–56 months). The demographic data of the patients are presented in Table 1. The measurements of both limb lengths and the LT-IT/P index were determined to have very good to excellent interobserver and intraobserver reliability. The hips were classified as 58 (73.5%) Crowe 4 and 21 (26.5%) Crowe 3. STO was applied to 47 (60%) hips and not applied to 32 (40%) hips. The mean amount of shortening in the group applied with STO was 3.2 ± 0.7 cm. In the patients without STO, lowered neck osteotomy and controlled femoral cracking were applied to 16 (50%). In six (16%) of the patients without STO, the center of rotation was observed to be high (mean 0.9 ± 0.1 mm). Acetabular graft from the femoral head was applied to a total of six (16%) patients, all from the group without STO.
Demographic data of the patients.

BMI: body mass index; STO: subtrochanteric osteotomy.
Functional outcomes
HHS was determined as 90.1 ± 9.6 (range 78–100) in the STO group and 88.1 ± 6.4 (range 84–99) in the non-STO group (p = 0.560). When the HHS was evaluated according to the reduction method in the non-STO group, mean HHS was 87.4 ± 5.2 (range 84–93) in the patients applied with controlled femoral cracking and 88.3 ± 5.7 (range 86–99) in those not applied with femoral cracking (p = 0.740). In the patients applied with acetabular graft, HHS was determined as 86.3 ± 4.2 (range 84–91), and in those where no graft was used, 89.3 ± 9.7 (range 78–100) (p = 0.380). HHS was 89 ± 2.1 (87–91) in patients with high acetabular center of rotation and 89.5 ± 9.4 (range 78–100) in those where the center of rotation was preserved (p = 0.864). The mean lengthening obtained in the non-STO group was 3.2 ± 0.8 cm (range 1–4.2 cm) and mean LLD was determined as 0.9 ± 0.8 cm (range 0–2.5 cm). In the STO group, mean LLD was 1.8 ± 0.9 cm (0–3.6 cm). LLD of <2 cm was observed in 29 (91%) patients without STO and in 28 (59%) of those with STO.
Complications
Nonunion was observed in three (6%) patients with STO. Osteosynthesis with plate and autograft was applied to these patients 6–9 months postoperatively and full union was then observed in the follow-up period. Major vascular injury (external iliac vein) developed in two patients, who had Crowe type 4 dislocations, and acute repair was performed by cardiovascular surgeons. Early postoperative dislocation was observed in six patients. Of these, reduction stability was provided with constrained acetabular cup revision in four cases, and in two patients revision with cage-cemented polyethylene insert. In one patient with cemented acetabular cup, permanent sciatic nerve damage developed postoperatively. Sciatic nerve exploration in this patient revealed that the cement was in close proximity to the sciatic nerve, and fibrotic changes developed in the sciatic nerve in this area. Therefore, the sciatic nerve damage was determined to have developed as a secondary effect. Infection developed in four patients, which was superficial in two and recovered with antibiotherapy within 2 weeks. Deep infection with wound leakage in the other two patients was treated with irrigation and debridement, change of insert and 6 weeks of (iv) antibiotherapy. Infection was totally resolved in these patients.
In the patients without STO, dislocation was observed in two patients, both of whom were treated with closed reduction in the early period and no periprosthetic infection was observed. Permanent sciatic nerve palsy developed in one patient despite emergent surgical exploration and release of the peroneal nerve at the level of the fibular head.
At the end of 18 months, tendon transfer because of drop foot was applied to the patients from both groups with permanent sciatic nerve palsy. The complication rates, operating times, and requirement for erythrocyte suspension transfusion are provided in Table 2. There was no statistically significant dislocation and infection rates were higher (25% and 15; p = 0.108 and p = 135; respectively) in patients with Crowe type 4 hips or in those with TM-TI/P ratio >0.4.
Comparison of data obtained from patients’ follow-up.

LT-IT: the distance between the apex of the lesser trochanter and the ischial tuberosity; P: vertical height of the pelvis; STO: subtrochanteric osteotomy.
Interpretation of the classification
Patients with Crowe 3 or 4 hips had either ≥0.3 or <0.3 LT-IT/P ratio. The mean LT-IT/P was determined to be 0.377 ± 0.18 (range 0.7–0.3) in patients with STO, 0.2 ± 0.15 (range 0.125–0.29) in patients without STO, 0.23 ± 0.08 (range 0.29–0.19) in patients with controlled femoral cracking, and 0.275 ± 0.1 (range 0.29–0.23) in patients with high center of rotation (Figure 3). Additional reduction methods, such as lowered neck osteotomy and controlled femoral cracking, and soft-tissue lengthening (n = 16, 50%) were needed when the LT-IT/P ratio was between 0.2 and 0.3, and in patients with Crowe 2 hips, there was seen to be increased acetabular center of rotation. There was no need for femoral cracking or increase in center of rotation in patients with LT-IT/P <0.19 and all had Crowe 1 hips (Table 3). The number of complications of dislocation (25%) and infection (%15) was higher for types 4 but not statistically significant (p = 0.135, p = 0.108, respectively). No statistically significant difference was determined in HHS, but as these are mainly affected by pain and function, this could explain the high HHS in both groups, which can be attributed to the success of the arthroplasty itself.
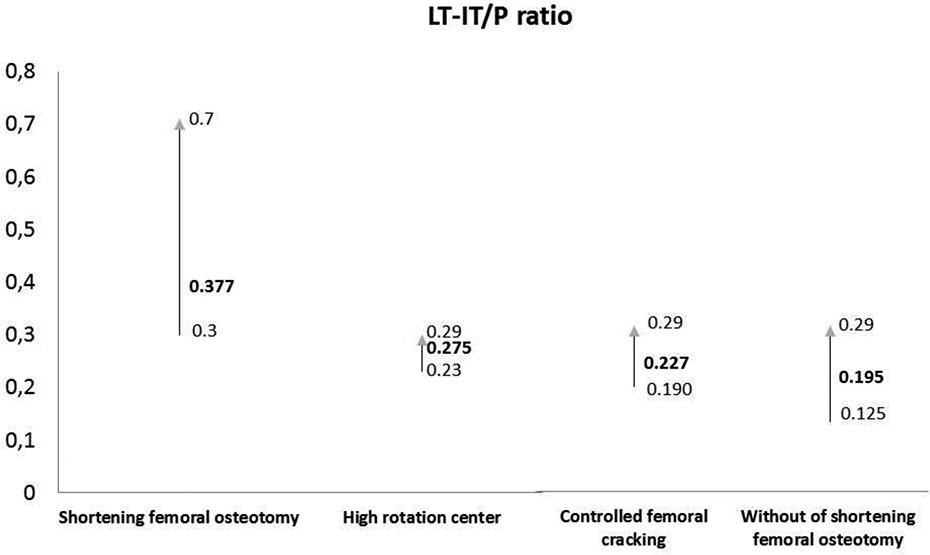
The relationship between LT-IT/P index and STO requirement, high rotation center, and controlled femoral cracking requirement. LT-IT: the distance between the apex of the lesser trochanter and the ischial tuberosity; P: vertical height of the pelvis; STO: subtrochanteric osteotomy.
Comparison of dislocation types with regard to LLD, infection, dislocation, and Harris score.

LLD: limb length discrepancy.
a Kruskal–Wallis test.
b χ 2 test.
Discussion
Although numerous classification systems have been described for Developmental Dysplasia Hip (DDH), the complex array of pathology seen in high-riding hips does not lend itself to these systems and thus, the classifications cannot direct decision-making about the need for a STO. Previous studies have reported the need for a cutoff value for femoral shortening osteotomy. 12,16,17 In this study, it was determined that in patients with type 3 or 4 dislocations, STO should be added to THA. In patients with type 2 dislocations, the likelihood of soft-tissue lengthening, the need for controlled cracking of the femur, and elevation of the center of rotation increase. If a patient has a type 1 dislocation, the need for both controlled cracking and the increased height of the center of rotation is eliminated. If there is a type 4 dislocation, the complication rate and the risk of LLD are further increased.
Although STO is often used on the femoral side to facilitate the reduction and to prevent the development of sciatic nerve palsy, STO alone can cause a series of complications. In contrast to lower rates of erythrocyte transfusion and a shorter operating time for patients without STO, higher rates of dislocation, infection, and vascular damage have been seen in patients with STO. 18,19 Li et al. evaluated the results of shortening osteotomy in a similar group of patients with Crowe type 4 hips. 20 A high rate of recovery was observed in both groups, and no significant difference was determined between the groups with or without STO. Similarly, in the current study, a significant increase was found in the functional scores of both the STO and non-STO groups compared to the initial scores, and there was no significant difference between the groups. In the patients applied with controlled femoral cracking for reduction and those with increased height of the center of rotation, there was a significant increase from baseline but lower scores were determined and no significant difference was observed between the groups.
Femoral shortening osteotomy is a more invasive procedure, and following the osteotomy decision, dangers expected during the surgery include increased bleeding, problems of femoral component stability, postoperative hip joint stability, and nonunion problems in the osteotomy line. In the current study, STO prolonged the operating time and increased the need for blood transfusion. The most feared complication is the development of sciatic nerve palsy, which can develop due to the lengthening. 12,14,21 Nerve damage in THA is observed most often in the peroneal section at the rate of 90% and is caused by the change in the relationship of the sciatic nerve in the peroneal branch with the piriformis. 22 Although it is accepted that surgeries without shortening may increase the risk of sciatic nerve injury, in current literature, damage to the sciatic nerve has not been reported to be as frequent as expected. 23 Additional reduction methods were used in those studies, such as additional shortening of the femoral neck, additional soft tissue loosening, and the administration of additional rocuronium to provide full muscle relaxation. 13,14,24 In the current study, sciatic nerve damage developed in one patient in the non-STO group. This low rate of sciatic nerve damage can be explained by the application of STO to patients with >4 cm lengthening expected preoperatively. Whether or not lengthening is applied, attention must be paid to exposure, retraction, and the placement of retractors during THA to prevent sciatic nerve damage.
In high-dislocated hips, the correction of LLD without disrupting either the component or joint stability is another problem. Appropriate femoral offset and equal leg length is very important for restoration of the hip biomechanics. 25 LLD in THA is one of the most common reasons for litigation. However, it has been accepted that LLD may not be able to be fully corrected in these types of hips. 26,27 Furthermore, the amount of LLD that may be acceptable is not clear. In the current study, in patients without STO, mean leg lengthening was 3.2 cm and full limb length equality was obtained in 29 (91%) patients. In the STO group, mean lengthening of 2.9 cm was obtained but LLD of >2 cm was observed to continue in 19 (41%) patients. Correction of LLD in high DDH has been reported to be difficult. This subject must be explained to patients, especially those for whom shortening is planned. In the patients with LLD, height correction with footwear was only required in one patient. The continuation of this condition may not disturb patients postoperatively as they have become physiologically accustomed to LLD in high DDH. Another reason could be that all patients were preoperatively informed about this subject and patients were not operated on because of LLD only but for severe and disabling pain due to coxarthrosis.
The dislocation rate has been reported to be high for high-riding hips. 10,15 This change in dislocation rate is attributed to variations in anatomy, the use of a small acetabular cup and femoral stem, and difficulties in femoral stem stability. In the current study, dislocation was observed in eight (9%) hips, six of which were applied with STO. It is noticeable that studies that have found high rates of dislocation are those that have usually used shortening osteotomy procedures. Dislocations can be related to insufficient soft tissue balance and insufficient femoral stem stability in STO applications. Similar complication rates have been reported for infection. In the current study, infection was determined in four (6%) patients and all of these were in the STO group. This increased infection rate can be attributed to the greater exposure, longer operating time, and greater blood loss in the STO group.
As in all retrospective studies, this study has some inherent limitations. A prospective randomized study should be performed to compare complications and functional outcomes related to osteotomy and to evaluate the efficacy and reliability of this new classification. The final decision to perform an osteotomy was dependent on the surgeon, and the necessity for osteotomy varied according to the reduction method used. All the cases were operated on by a single surgeon with more than 15 years of experience of such cases, and this strengthened the findings of the study. Statistical power may not have been strong enough because of the small sample size, and no post hoc power analysis was conducted, as there is controversy about its usefulness. For example, the difference in HHS scores between the STO and non-STO groups (90.1 vs. 88.1) had a p-value of 0.560, and so the power analysis of the test would have been at too low a level due to the characteristics of the two cohorts. Pelvic obliquity or spinal flexibility was not evaluated in this study. Although it has been reported that flexibility of the lumbosacral junction is an important determinant for equalization of leg lengths, the fixed characteristics of the lower lumbar spine precludes equalization, especially in patients with STO. 6 Finally, in this particular case series, it would have been very useful while comparing patients with and without STO to use a more precise gait analysis, but due to the retrospective nature of the study, it was not really feasible. However, that is something which could be incorporated in future studies.
Conclusion
STO is a complex surgical procedure that is vulnerable to complications. With prolonged operating time and a greater need for erythrocyte suspension replacement, STO increases complication rates such as dislocation and infection. This new classification can be used in preoperative planning in lieu of other classifications for guidance of surgical procedures adjunct to THA, such as controlled femoral cracking and/or soft tissue lengthening (for type 2) and femoral shortening osteotomy (types 3 or 4). Further, large-scale studies are required to address the feasibility of the use of this classification for guidance in respect of femoral shortening osteotomy during THA of high-riding hips specifically.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.