
Abstract
The morphological characteristics associated with a diagnosis of femoroacetabular impingement (FAI) observed on plain radiographs can also be seen in subjects without hip joint symptoms. Therefore, the purpose of this study was to investigate whether sclerotic lesions on femoral head–neck junction (FHNJ) could be used as a supplemental diagnostic feature. A total of 128 hips from 119 patients (43 male and 76 female) diagnosed with FAI and 24 hips from 21 patients (2 male and 19 female) with other hip pathologies as control were compared in this study. Using standing frog-leg plain radiographs, the prevalence of sclerotic lesions on the FHNJ was established. Additionally, the pixel intensity (PI) of the sclerotic lesions between the FAI and the control groups were quantitatively compared. Sclerotic lesions were present in 96.1% of FAI hips (123 of 128) and only 37.5% of control hips (9 of 24) (p < 0.05). The ratio of PI in the FAI group was significantly higher (approximately 10%) than in the control group (p < 0.05). The evaluation of sclerotic lesions may be used as a supplement to aid in the diagnosis of FAI.
Keywords
Introduction
Femoroacetabular impingement (FAI), characterized by the premature colliding of the acetabulum and femur during hip motion, has been thought of as an important mechanism in the development of early hip osteoarthritis. 1 Previous studies have described specific anatomical morphologies characteristic of FAI, observed on various imaging modalities, such as large α angle, 2 a bump formation, 3 and pistol grip deformity 4 on the femoral head–neck junction (FHNJ). However, because these characteristics can also be seen in subjects without hip joint symptoms, 5 the development of additional diagnostic imaging may be necessary.
It is well-known that sclerotic lesions observed on plain radiographs occur in regions where mechanical compression stress is exerted, 6 such as the subchondral bony surface of the osteoarthritic knee. However, few studies have looked at the development of sclerotic lesions on the FHNJ. 7,8 In hips with FAI, when the femur is flexed, the FHNJ collides with the acetabulum which could potentially lead to the development of such lesions. Determining whether sclerotic lesions on the FHNJ are characteristic of FAI may provide additional information in distinguishing between patients with acetabular dysplasia (AD) who have clinical features of FAI and without. Although some researchers consider labral lesions in AD to be related to instability of hip joint, others have emphasized that there are AD patients who have symptoms of impingement similar to FAI patients. 9
The purpose of this study was to investigate whether sclerotic lesions on the FHNJ could aid in diagnosing FAI. For this purpose, preoperative plain radiographs of patients who previously underwent surgical treatment for FAI were used (1) to study the presence of sclerotic lesions, (2) to assess a key quantitative parameter for evaluating the sclerotic lesion, and compare it between FAI and control patient groups, and (3) to compare the key quantitative parameter between the AD patients of both groups.
Materials and methods
Patient population
With University of Utah Institutional Review Board approval (IRB# 71733) a retrospective chart and radiographic review was performed of patients who underwent hip arthroscopy surgery for the treatment of FAI between January and December in 2015 by a single high-volume orthopedic surgeon (SKA). In the university hospital, FAI was diagnosed from comprehensive assessment which consisted of patient history; physical examination such as anterior impingement test with range of motion 10 ; Beighton criteria for laxity evaluation 11 ; axial distraction test with checks of pain, toggle, and apprehension 12,13 ; Dial test 14 ; and FABER test for the symmetry check. 12 In the hip arthroscopy surgeries, the above author confirmed arthroscopic findings for FAI, which were fibrillation, delamination, or defect of cartilage at FHNJ, and/or labral tear, or delamination of transition area between the labrum and the acetabular cartilage. A total of 226 hip arthroscopy surgeries were initially reviewed. Patients were excluded if their radiographs were stored outside of the main electronic medical record (41), did not have preoperative radiographs or radiographs were obtained from an outside institution (24), or if they underwent revision hip arthroscopy (33). Included in the final analysis were 128 hips from 119 FAI patients (46 male and 73 female, mean age 36 (range 17–65) years). Additionally, 24 hips from 21 patients (2 male and19 female, mean age 36.2 (range 14–75) years) undergoing hip surgery for non-FAI related conditions (AD, gluteus–medius tears, ischiofemoral impingement, and hamstring tear) were reviewed as controls. Patient demographic information with age and gender are presented in Table 1.
Demographics of patients in this study.

FAI: femoroacetabular impingement.
Radiographic analysis
Standing frog-leg plain radiographs with the femur positioned slightly flexed, abducted, and rotated externally on a 10-cm tall foot board (Figure 1) were reviewed and analyzed by the lead author (TH) who is familiar with hip radiographs. 15

Patient positioning for obtaining the standing frog-leg view.
The area of the FHNJ was defined by first drawing a circle concentric to the center of the femoral head and with the best fit to the outline of the femoral bony head following the method proposed by Nötzli et al. 2 Next, a straight line was drawn parallel to the femoral neck axis passing through the center of the femoral head. Finally, FHNJ was determined as the area delimited by the first straight line intersecting the femoral head center perpendicularly and the second straight line tangential to the point on the circle where it crosses the femoral neck axis (Figure 2). This area is equal to the “superior extent of femoral neck” described by Jamali et al. 16

Determination of the area of femoral head–neck junction for detection of the sclerotic lesion and calculation of the pixel intensity of the sclerotic lesion. (a) The center of the femoral head is determined by making blue circle the best fit to the outline of the femoral bony head. White dotted straight line in the left side is drawn parallel to the femoral neck axis passing through the center of the femoral head. The area of the femoral head–neck junction is determined as the area delimited by the first straight line intersecting the femoral head center perpendicularly and the second straight line tangential to the point on the above circle where it crosses the femoral neck axis. (b) The area of the femoral head–neck junction is within the yellow line. The blue marked area indicates the sclerotic lesion in the femoral head neck junction.
Analysis of sclerotic lesion
The prevalence of the sclerotic lesions on the FHNJ was established by two authors (TH and SKA) independently examining all frog-leg radiographs in a blinded fashion. Intra-observer and interobserver variabilities were determined using κ coefficients with Fisher’s exact test. For the intra-observer variability (based on two measurements separated by a 3-week interval), the κ was 0.97. For inter-observer variability, the κ was 0.88. A quantitative evaluation of the sclerotic lesion was then performed. Using an open-source software (Image J: a Java-based image processing program developed at the National Institutes of Health), pixel intensity (or pixel value (PI)) of the sclerotic lesion on the FHNJ area was measured, including the bone cortex on the lateral side of the FHNJ. The PI is a single number that represents the brightness of the pixel. 17 The most common pixel format is the byte image, where this number is stored as an 8-bit integer giving a range of possible values from 0 to 255. In the radiograph, zero is taken to be black and 255 is taken to be white. To standardize this PI value in the sclerotic lesion, PI ratio was defined as the following:

Intra-observer and interobserver variabilities of this quantitative evaluation were investigated. The intra-observer error, which is difference of the PI ratio between the first and the second time measurements (based on two measurements separated by a 3-week interval) by one author (TH), was 0.12%, and the interobserver error, which is the difference of the PI ratio between both authors, was 0.13%.
AP radiograph in all 128 hips was used for evaluation of the lateral center edge angle in the following subcategory evaluation to extract dysplastic patients. AD hip (lateral center edge angle was <20°) and border line AD (lateral center edge angle was ≥20° and <25°) were extracted from both groups.
Statistical analysis
To evaluate the existence of the sclerotic lesions, the number of the hips with or without the lesions in both the FAI and the control groups were separated, then compared using a 2 × 2 contingency table. The PI ratios between the two groups were quantitatively compared using a Mann–Whitney U test. Additionally, the PI ratio of a subcategory AD patients (without and with border line AD) in both groups were analyzed using Mann–Whitney U test.
Results
Sclerotic lesions were more prevalent in the FAI group (96.1%; 123 of 128) compared to the control group (37.5%; 9 of 24) (p < 0.0001; Figure 3).
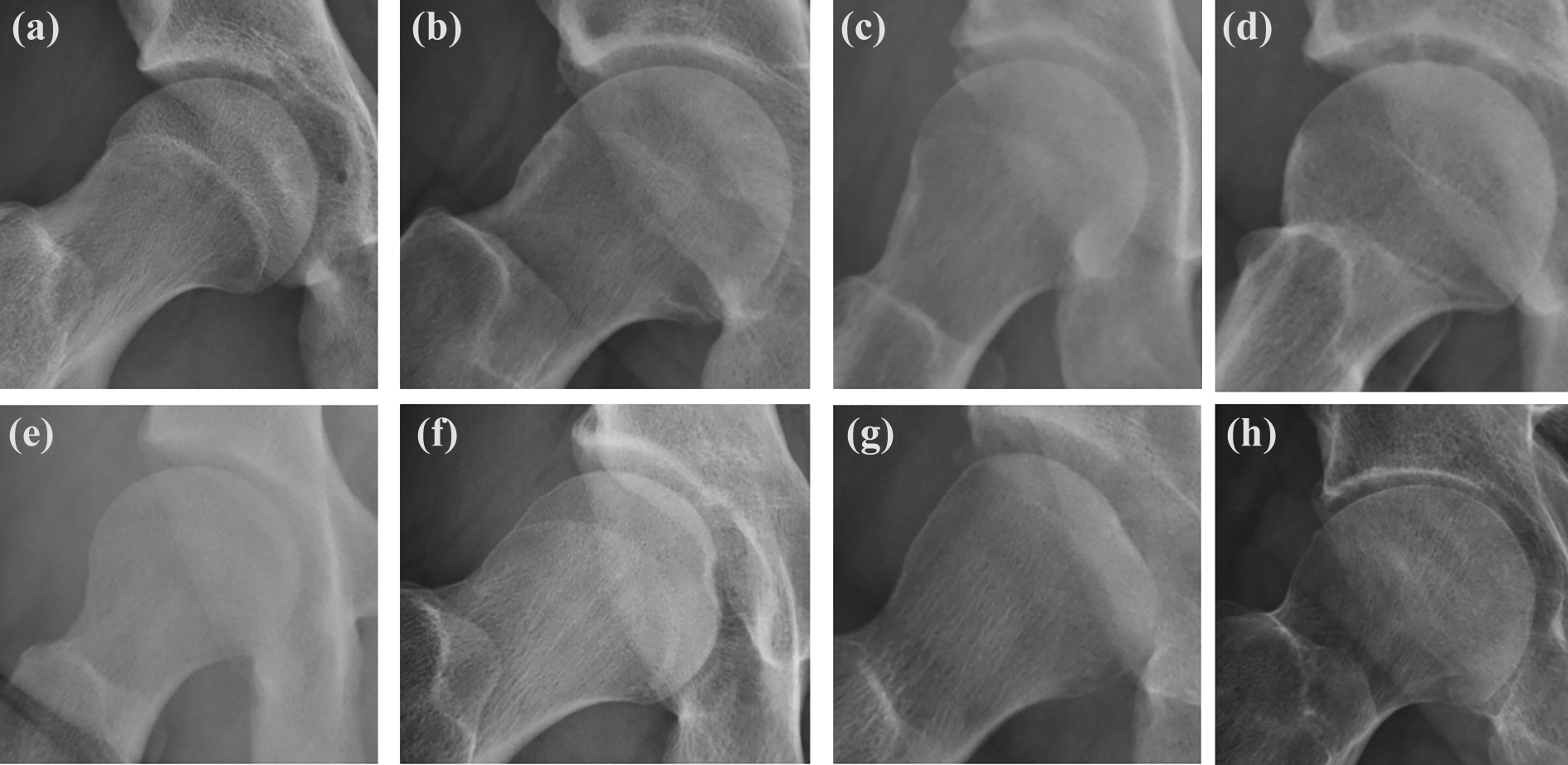
Sclerotic lesion of the femoral head–neck junction of representative cases in both FAI (a to d) and control (e to h) patients. FAI: femoroacetabular impingement.
The PI ratio in the FAI group (mean 110.1%, standard deviation (SD) 10.9%) was significantly higher than in the control group (mean 101.0%, SD 12.3%) (p < 0.0001). Among the subset of patients with dysplasia, the PI ratio in the FAI group was statistically significantly higher than the PI ratio in the control group (mean 111.3%, SD 19.6% vs. mean 97.6%, SD 10.4%) for AD hips (p < 0.0001). When the borderline AD hips are included in this analysis, its result was similar to the above one (mean 108.5%, SD 14.0% in FAI group vs. mean 99.7%, SD 9.5% in the control group) (p < 0.0001). While the FAI group had 10 hips with AD and 25 hips with borderline AD, the control group had 12 hips with AD and 5 hips with borderline AD.
Discussions
FAI has been recognized as a hip disease, which leads to osteoarthritis. Previous studies have described various imaging modalities useful in diagnosing FAI. 18 –20 However, because some asymptomatic subjects also have morphological features consistent with a diagnosis of FAI on imaging, additional tools to aid in the diagnosis FAI are necessary. The current study investigates whether the sclerotic lesion on lateral side of FHNJ on standing frog-leg plain radiographs is evidence of FAI.
According to the result of the current study, 96.1% of FAI patients had a sclerotic lesion detected on the lateral side of FHNJ. Previous reports have described the presence of a “herniation pit” on computed tomography or magnetic resonance imaging as a feature of FAI patients. 9,19,20 This pit or lesion forms under compressive forces. This phenomenon is very similar to what occurs to the subchondral area of tibia in knee osteoarthritis, which is affected by the compression between the distal femur and the proximal tibia. 6 The results of the current study show the evaluation of the sclerotic lesion may aid in the diagnosis of FAI in addition to plain radiographs.
PI was used as a quantitative evaluation of the sclerotic lesion. Although the PI is a gray scale from 0 to 255, it has been used as a key parameter of bone quality or bone density, 17 with one report showing an association between PI value and a sclerotic lesion. 21 In the current study, the PI ratio at the lateral side of FHNJ was statistically higher in the FAI group than in the control group.
Another important finding in the current study is the usefulness of the sclerotic lesion in detecting AD with FAI. While the labrum in FAI patients is damaged by the impingement, labral lesions also exists in AD patients due to load transfer and/or instability issues. The anterior impingement test is an important diagnostic test during the physical examination, however, the test cannot distinguish between labral lesions from FAI or AD. 22 The results of the current study found the PI ratio to be higher among FAI patients with AD compared to control patients, indicating that some therapies for FAI might be prioritized.
There are several limitations in the current study. First, the patients who underwent surgery for FAI were not diagnosed according to whether they had the sclerotic lesion. As we mentioned, FAI in the current study was diagnosed from the comprehensive assessment. Then, one or several hip lesion(s) was detected in the hip arthroscopy surgeries. However, there is no criterion so far to divide into subchondral bone with and without bony sclerosis at the FHNJ under arthroscopy. Therefore, we could clarify neither the positive nor the negative predictive value of the sclerotic lesion. Second, a genuine control group of individuals free from hip-joint diseases was not analyzed. This current study is one retrospective study. Therefore, the authors had to identify some patients with an issue around hip joint as control because they were taken hip X-rays. Ideally, for a further study, asymptomatic subjects should be recruited as control in a prospectively interventional study. Third, we did not evaluate the anatomical position of the sclerotic lesion in patients with and without FAI. Nonetheless, the only existence of the sclerotic lesions may play an effective role as an adjunct characteristic in the diagnosis of FAI.
In conclusion, the sclerotic lesion which is detected on the lateral side of FHNJ can aid in the diagnosis of FAI in addition to plain radiographs. The sclerotic lesion on the FHNJ may also aid in distinguishing between FAI patients with and without clinical features of AD.
Supplemental Material
Supplemental Material, 20200321_Answers_to_the_reviewers - Sclerotic lesions of the femoral head–neck junction for diagnosis of femoroacetabular impingement
Supplemental Material, 20200321_Answers_to_the_reviewers for Sclerotic lesions of the femoral head–neck junction for diagnosis of femoroacetabular impingement by Takehito Hananouchi and Stephen Kenji Aoki in Journal of Orthopaedic Surgery
Footnotes
Acknowledgement
The authors would appreciate Ms Temitope Folashade Adeyemi for English editing of this manuscript.
Authors’ note
The authors already had the poster presentation about the contents of this article in the annual meeting of Japanese Society for Hip Arthroscopy in 2017. This article was evaluated as the best poster award.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.