
Abstract
Background:
In vivo three-dimensional (3D) kinematics of the scapula after reverse total shoulder arthroplasty (rTSA) have been sparsely investigated. The aim of this study was to analyze static and dynamic kinematic alterations of the scapula after rTSA in vivo with the use of computer-aided 3D reconstruction program.
Methods:
A total of 15 patients with cuff tear arthropathy treated by rTSA participated. Scapulae with rTSA and the contralateral scapulae were evaluated with computed tomography scan data in 0° and 120° forward flexion positions of the glenohumeral joint. To examine static scapular kinematic alterations, the angular position and distance from the thorax were evaluated in the shoulder neutral position. 3D rotational and translational movements of the scapula in relation to the thorax were also measured during arm elevation to evaluate dynamic scapular kinematic alterations.
Results:
Scapulae with rTSA were more anteriorly tilted in the sagittal plane and more internally rotated in the axial plane than were the contralateral scapulae. However, no significant differences were observed in the upward rotated position in the coronal plane or in the distance from the thorax in any plane between the scapulae with rTSA and the contralateral scapulae. In dynamic analyses, upward rotational movement in the coronal plane, external rotation in the axial plane, and posterior tilting in the sagittal plane showed significant differences between the scapulae with rTSA and the contralateral scapulae during elevation. In contrast, translational movements in coordination revealed no statistical differences between the two scapular groups except for lateral translation.
Conclusion:
Data from the 3D reconstruction program showed that rTSA might result in static positional changes and dynamic movement alterations.
Level of Evidence:
Therapeutic, IV
Keywords
Introduction
Reverse total shoulder arthroplasty (rTSA) has been used widely in patients with irreparable rotator cuff dysfunction. 1 After rTSA surgery, several kinematic changes such as medialization of the rotation center and fulcrum movement during shoulder elevation have been observed in the shoulder girdle. 2 Because the scapula is the most important structure for normal shoulder function and stabilized movement of the glenohumeral joint, 3 kinematic alterations after rTSA surgery should be evaluated.
Scapular kinematic alterations may be associated with rotator cuff disease, glenohumeral instability, shoulder impingement syndrome, and frozen shoulders. 3 These alterations might affect normal scapulohumeral rhythm and thoracoscapular movement. In addition, patterns of scapular kinematic alterations differ under various conditions. 4,5
Several investigators have performed kinematic analyses on patients with rTSA by measuring the range of shoulder motion in vivo using electromagnetic tracking systems with marker cluster. 6 –8 However, obtaining accurate three-dimensional (3D) motion data with such a method can be difficult. Skin marker palpitation can interfere with dynamic motion measurement. 9,10 Furthermore, pinning the target bone for 3D motion tracking is an invasive procedure. 11 The scapula can also be evaluated kinematically with plain radiography; however, measurements of the 3D scapular position after rTSA could be difficult to obtain with two-dimensional plain radiography because of image distortion and superimposition of skeletal structures. 12 With the development of 3D printing technologies, computer-aided 3D reconstruction programs have become widely used in kinematic analysis. 3D reconstruction images obtained from these programs may be very useful in planning of the shoulder surgery and in investigating shoulder kinematics afterwards. 4,5,13
The aim of this study was to investigate both static and dynamic scapular kinematic alterations after rTSA in vivo with the use of computer-aided 3D reconstruction programs.
Materials and methods
Patients
This retrospective observational study was approved by the Institutional Review Board of our University Hospital (IRB No. KBSMC 2018-07-040), who waived the requirement for informed consent. A total of 15 patients (10 females and 5 males) with unilateral cuff tear arthropathy treated by rTSA from March 2014 to August 2018 were evaluated. The inclusion criteria were patients with (1) no osteoarthritic changes, stiffness, instabilities, or trauma history of the contralateral shoulder and (2) no rotator cuff tear or rotator cuff tendinopathy in the contralateral shoulder, confirmed by ultrasonography. All patients were able to perform a range of 0° to 120° glenohumeral joint forward flexion in both shoulders without pain or discomfort. The mean age of these patients was 74.6 years (range 62–82 years), and computed tomography (CT) scans were performed at an average of 12.2 months (range 11–14 months) after surgery to evaluate the scapular kinematic alterations. All procedures were performed by one orthopedic surgeon (EK) using an onlay short-stem reversed shoulder prosthesis (Aequalis Ascend™ Flex; Tornier Inc., Edina, Minnesota, USA).
Positions during CT session
CT images of all 30 shoulders of the 15 patients were obtained. In each patient, both the scapula with rTSA (rTSA scapulae) and the contralateral scapula (non-rTSA scapulae) were evaluated in 0° and 120° forward flexion positions of the glenohumeral joint. Using a goniometer (NutriActiva, Minneapolis, Minnesota, USA) before each CT session, one orthopedic surgeon (SWH) measured the extent of glenohumeral joint forward flexion. All CT sessions were conducted with the patient in a prone position with soft padding on the chest because the scapular kinematics could be interrupted by the CT table in the supine position (Figure 1). All patients were positioned with the elbow fully extended, the forearm in neutral rotation, and the palm facing the trunk. 14 The goniometer was aligned as follows: (1) The stationary arm was positioned parallel to the lateral midline of thorax, (2) the moving arm was positioned parallel to the lateral midline of the humerus toward lateral humeral epicondyle, and (3) the axis of the goniometer was located at the midpoint of lateral aspect of acromion process. 14 We evaluated the intra-observer reliability of the goniometric measurements by measuring the glenohumeral joint when the contralateral shoulder was in full forward flexion in all participants. These measurements were obtained 6 months before the study began.

Computed tomography data obtained in the prone position. (a) A patient positioned prone and 0° forward flexion of the glenohumeral joint. (b) A patient positioned prone and 120° forward flexion of the glenohumeral joint.
Three-dimensional reconstruction with computed tomography
3D images of all shoulders were obtained by using the same CT machine, a 64-slice multi-detector CT scanner (Brilliance iCT 64; Philips Medical Systems, Amsterdam, The Netherlands). Imaging parameters were as follows: 120 kVp tube potential, 100 mAs tube current-time product, 32 × 0.625 mm section collimation, 0.4 ms rotation time, 0.282 pitch; 320 mm display field of view, and 1 mm section thickness. Sagittal, coronal, and axial images of both shoulders and the thorax were exported in Digital Imaging and Communications in Medicine (DICOM) file format. CT data in DICOM format were imported into a 3D reconstruction program (Bone Viewer™, Bone Simulator™; Orthree Co., Ltd, Osaka, Japan). With this program, CT images were reconstructed into 3D surface models and 3D locations of scapulae were evaluated in 0° forward flexion position to determine static scapular kinematic alterations.
Evaluation of scapular kinematic alterations
In each patient, two bone models made from 0° and 120° forward flexion positions of the glenohumeral joint were superimposed on the thorax to evaluate scapular kinematic alterations using a markerless surface registration technique. 15 A voxel-based registration was used to analyze the scapular motion. Rotation and translation of the scapulae were calculated in relation to the thorax using position vectors in 3D space, defined according to x, y, and z axes. These position vectors were calculated according to an anatomical orthogonal reference system modified from the scapular coordinate system of the International Society of Biomechanics. 16
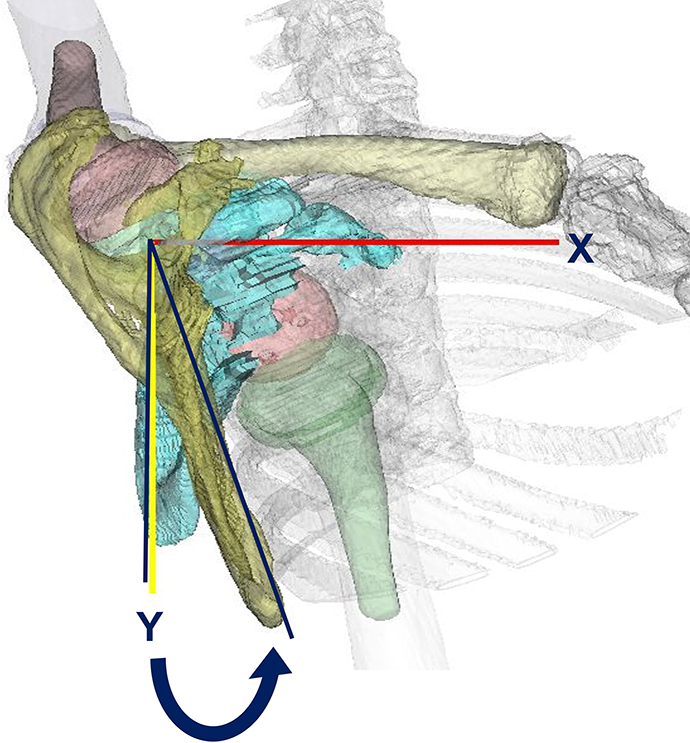
Three coordinate axes of the scapula were defined by analyzing 3D scapular motions as described in a previous study by Kim et al. 4,5 First, the Z axis was defined as the line connecting the trigonum spinae scapulae (TS, the midpoint of the triangular surface on the medial border of the scapula in line with the scapular spine) and the angulus acromialis (AA, the most posterolateral point of the acromion). Next, the X axis was defined as a line perpendicular to the plane formed by the Z axis (AA and TS) and the angulus inferior (AI, the most caudal point of the scapula) pointing from the AA. Finally, the Y axis was set as a line perpendicular to X and Z axes (Figures 2 and 3).
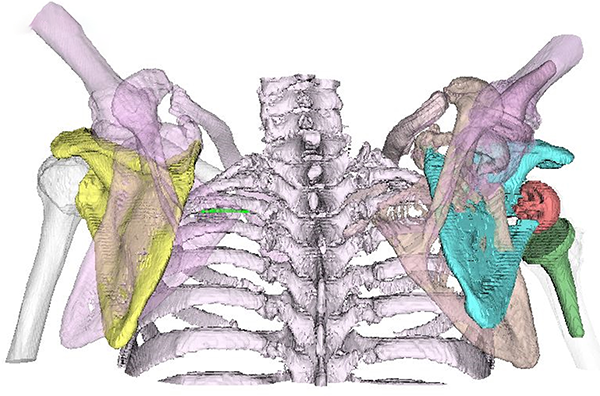
Three-dimensional scapular kinematic analysis model. Bone surface model including the thorax and contralateral shoulder generated by the software.

The anatomical coordination system. Three-dimensional rotational motion relative to the thorax was calculated based on the coronal (YZ), sagittal (XY), and axial (XZ) planes and translational motion along the X, Y, and Z axes in the Euler space. TS: trigonum spinae scapulae; AA: angulus acromialis; AI: angulus inferior.
To analyze static scapular kinematic alterations, degrees of 3D angular rotation of the scapula around the reference axis in the static state were assessed first. The anatomical coordinate in the thoracic center was used as the reference axis to determine angular and translational positions of the scapula relative to the thorax. The coordinate at the central axis of the thorax in static kinematic alterations consisted of three axes: X′, Z′, and Y′. The X′ axis was defined as the axis passing horizontally from the suprasternal notch of the sternum to the center of the spinal canal. The Z′ axis was defined as the axis passing horizontally from the center of the spinal canal where the X′ axis passed. The Y′ axis was defined as the axis perpendicular to both X′ and Z′ axes at the center of the spine where the X′ axis passed. Each angular position of the scapula was measured relative to the central axis of the thorax in coronal, axial, and sagittal planes. In the coronal plane, we observed an upward angulation defined by the angle of Z and Z′, internal rotation by X and X′, and anteriorly tilted by Y and Y′ (Figures 4 to 6).

Static scapular kinematic alterations: rotational movement. The central thoracic axis of the static kinematic alterations: X′, Y′, and Z′. Upward angulation: upward rotation around the X axis in the coronal plane (YZ). SN: the suprasternal notch of sternum.

Static scapular kinematic alterations: rotational movement. Internal rotation in the Y axis in the axial plane (XZ). CSC: the center of the spinal canal.

Static scapular kinematic alterations: rotational movement. Posterior tilt around the Z axis in the sagittal plane (XY).
To analyze the translational position, distances of both scapular axes from the central axis of the thorax were measured. We defined distances along Y′, Z′, and X′ axes in the coronal plane as upward

Static scapular kinematic alterations: distance from the central axis. The central thoracic axis of the static dyskinesis: X′, Y′, and Z′. HD: The distance from the central axis to the Y′ axis in coronal plane (Y′Z′); U-DD: The distance from the central axis to Z′ axis in axial plane (X′Z′). HD: horizontal distance; U-DD: upward–downward distance.

Static scapular kinematic alterations: distance from the central axis. A-PD: The distance from the central axis to the X′ axis in the sagittal plane (X′Y′). A-PD: anterior–posterior distance.
To evaluate dynamic scapula kinematic alterations, rotational movement of the scapula relative to the thorax was calculated based on the anatomical coordinate system defined above. Rotational values were defined as follows: upward (+)/downward (−) around the X axis in the coronal plane (YZ), external (+)/internal (−) rotation around the Y axis in the axial plane (XZ), and posterior tilt (+)/anterior tilt (−) around the Z axis in the sagittal plane (XY) in 3D coordinates (Figures 9 to 11).

Dynamic scapular kinematic alterations: rotational motion relative to the thorax was calculated based on the coronal (YZ), sagittal (XY), and axial (XZ) planes. Upward/downward rotation around the X axis in the coronal plane (YZ).

Dynamic scapular kinematic alterations: rotational motion. External/internal rotation around the Y axis in the axial plane (XZ).
Dynamic scapular kinematic alterations: rotational motion. Posterior/anterior tilt around the Z axis in the sagittal plane (XY).
To evaluate the translational movement of the scapula along the three axes, the distance from the scapular axis of each scapula between neutral and 120° forward elevated positions was measured along X, Y, and Z axes. Translation was defined as posterior (+)/anterior (−) along the X axis, superior (+)/inferior (−) along the Y axis, and lateral (+)/medial (−) along the Z axis (Figures 12 and 13).

Dynamic scapular kinematic alterations: translational motion along the X, Y, and Z axes in the Euler space. LMT: The distance from the coronal plane (YZ) along the Z axis; SIT: The distance from the sagittal plane (XY) along the Y axis. LMT: lateral–medial translation; SIT: superior–inferior translation.

Dynamic scapular kinematic alterations: translational motion. Posterior–anterior translation: The distance from the axial plane (XZ) along the X axis.
Statistical analysis
Power analysis indicated that a sample of 15 patients for a paired t-test would provide 90% statistical power and a 0.05 significance level with a large effect size (d = 0.8). A Kolmogorov
Results
Static scapular kinematic alterations
The ICC (2, 1) for intra-observer reliability of the goniometric measurements of the normal shoulder was 0.77. Therefore, the intra-observer reliability was considered acceptable.
The rTSA scapulae were more internally rotated in the axial plane (rTSA group: 33.1° and non-rTSA group: 27.3°) and tilted more anteriorly in the sagittal plane (rTSA group: 19.3° and non-rTSA group: 6.7°) than the contralateral non-rTSA scapulae (Table 1, Figure 14). Both these differences were statistically significant (both ps < 0.05). However, both groups showed no statistically significant difference during the upward rotation in the coronal plane (rTSA group: 11.3° and non-rTSA group: 17.6°) or translational location to the central axis of the thorax (rTSA group: 27.8 mm and non-rTSA group: 36.7 mm on the X axis; rTSA group: 37.9 mm and non-rTSA group: 33.2 mm on the Y axis; and rTSA group: 169.7 mm and non-rTSA group: 171.1 mm on the Z axis) (Table 2, Figure 15). Differences in the central axes of the thorax or scapular axes along any axis were not significant.
Rotational position of the scapula, evaluated from the viewpoint of static scapular kinematic alterations.

SD: standard deviation; rTSA: reverse total shoulder arthroplasty.
a p < 0.05 by paired t-test.

Comparison of rotational position between scapulae treated with rTSA and the contralateral scapulae, in terms of static scapular alteration. rTSA: reverse total shoulder arthroplasty.
Distance between the axis of the central thorax and the scapula, evaluated from the viewpoint of static scapular kinematic alterations.

SD: standard deviation; rTSA: reverse total shoulder arthroplasty.

Comparison of axis distance between scapulae treated rTSA and the contralateral scapulae, in terms of static scapular alteration. rTSA: reverse total shoulder arthroplasty.
Dynamic scapular kinematic alterations
Scapulae with rTSA showed a significantly more upward rotation than contralateral scapulae in the coronal plane (rTSA group: 45.6 ± 7.6°, non-rTSA group: 36.2 ± 7.4°, p < 0.05), more external rotation in the axial plane (rTSA group: 21.7 ± 9.2°, non-rTSA group: 13.4 ± 8.9°, p < 0.05), and more posterior tilting in the sagittal plane (rTSA group: 41.0 ± 9.1°, non-rTSA group: 22.2 ± 8.0°, p < 0.05) (Table 3, Figure 16).
Three–dimensional rotational movement of the scapula, evaluated from the viewpoint of dynamic scapular kinematic alterations.

SD: standard deviation; rTSA: reverse total shoulder arthroplasty.
a p < 0.05 by paired t-test.

Comparison of three-dimensional rotational movement between scapulae treated with rTSA and the contralateral scapulae, in terms of dynamic scapular alteration. rTSA: reverse total shoulder arthroplasty.
Differences in the lateral translational movement were not statistically significant between the scapulae with rTSA and the contralateral scapulae on the Z axis (rTSA group: 59.7 ± 14.2 mm, non-rTSA group: 50.9 ± 11.4 mm, p < 0.05). However, other translations along the coordination axis showed no significant difference between the two groups. (rTSA group: 32.3 ± 7.1 mm and non-rTSA group: 27.6 ± 8.5 mm on the X axis; rTSA group: 20.5 ± 12.0 mm and non-rTSA group: 27.2 ± 15.7 mm on the Y axis) (Table 4, Figure 17).
Three-dimensional translational movement of the scapula, evaluated from the viewpoint of dynamic scapular kinematic alterations.

SD: standard deviation; rTSA: reverse total shoulder arthroplasty.
a p < 0.05 by paired t-test.
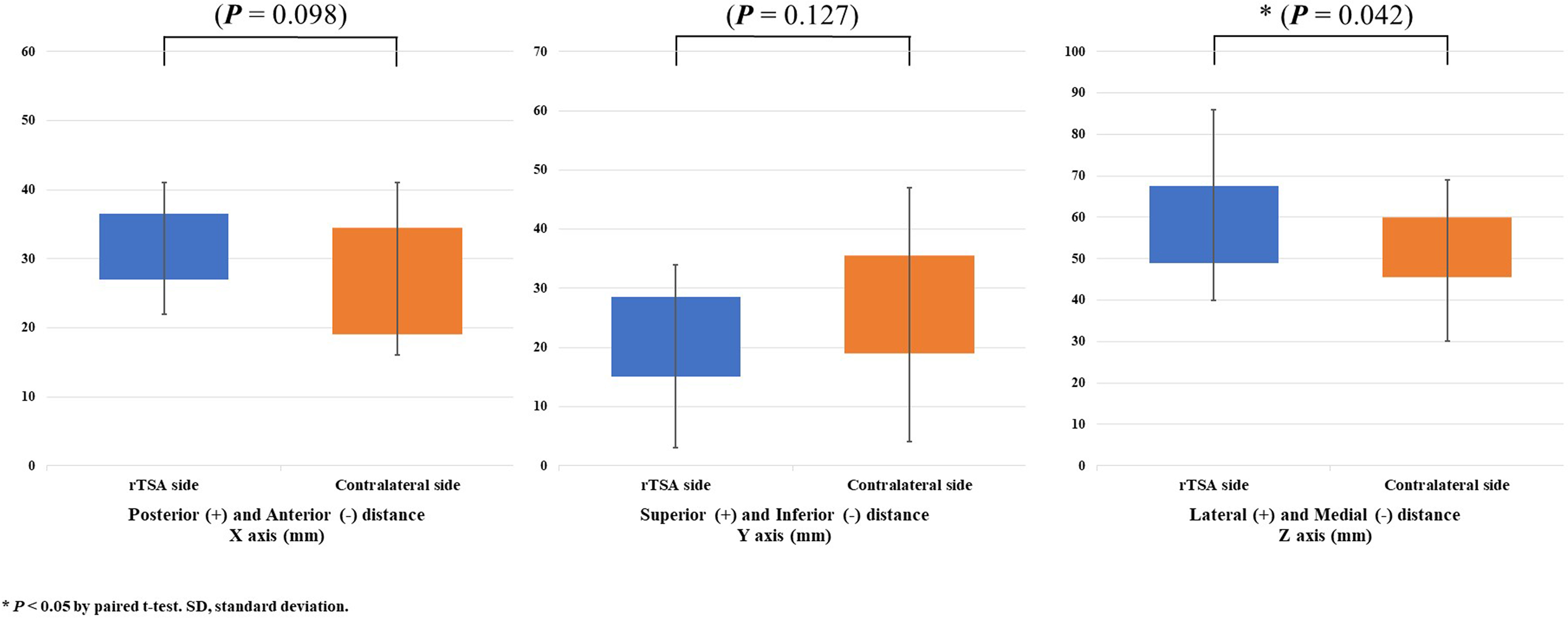
Comparison of three-dimensional translational movement between scapulae treated with rTSA and the contralateral scapulae, in terms of dynamic scapular alteration. rTSA: reverse total shoulder arthroplasty.
Discussion
Neer et al. 17 proposed the term “cuff tear arthropathy” to describe the relationship between massive rotator cuff tears and degenerative changes in the glenohumeral joint. Although rTSA is considered useful in affected patients for improvement of their quality of life and restoration of pain-free range of motion, it may alter the basic biomechanics of shoulder movement. 18,19 Several previous investigators have tried to reveal those kinematic changes in the shoulder joint after rTSA, 7 but the exact cause of the changes has not been elucidated.
The results of this study indicated both static and dynamic scapular kinematic alterations after rTSA. The anterior tilting and internal rotation of the scapula in static analyses were observed, that might be associated with increased deltoid muscle tension after rTSA. 20 The posterior portion of the deltoid usually originates from the posterior scapular spine and inserts at the deltoid tuberosity of the humerus located anteroinferiorly to the origin. 21 Therefore, increased deltoid muscle tension after rTSA might cause internal rotation of the scapula in the axial plane and anterior tilting of the scapula in the sagittal plane. Furthermore, it also might cause increased rotational movements in all coronal, axial, and sagittal planes in dynamic analyses. Therefore, we carefully suggest that the scapulothoracic movement may be increased after rTSA.
In patients who have undergone rTSA, dysfunction of the rotator cuff, which plays a role in deltoid muscle function, may be associated with reduced range of motion in the glenohumeral joint. 22 This may increase the relative contribution of the scapulothoracic joint to total arm motion, in comparison with the glenohumeral joint. Rotator cuff dysfunction might also increase scapulothoracic movement, as observed in this study. 23 Furthermore, alterations in scapular kinematics might be associated not only with changes in range of motion of the shoulder joint but also with shoulder pain. 24 Therefore, rehabilitation procedures, including parascapular muscle strengthening exercise should be considered for pain management after rTSA. 25
A number of studies about the relationships between rTSA outcomes and implant design have been conducted. Inclination, retroversion, and lateralization of the humeral component have been studied extensively in recent years. 26 –28 Inclination of the humeral component may play an important role in implant stability and in the incidence of scapular notching in rTSA. 26 A cadaveric study with implants installed in retroversion during rTSA showed changes in range of motion of the shoulder. 29 In contrast, Rhee et al. 27 reported no difference in range of motion in accordance with the degree of humeral retroversion. In those studies, only the association between shoulder range of motion and implant design was studied. The contrasting results might have resulted from the lack of consideration of the scapular kinematic alteration after rTSA.
The 3D reconstruction program used in this study could identify the accurate position of the scapula in the 3D manners. 3D positional evaluation with this program has also been performed after a clavicle or scapular fracture and after acromioclavicular dislocation with a hook plate without coracoclavicular ligament repair. 5,20 Previous studies that determined accurate scapular position on the 3D plane showed noticeable scapular kinematic alterations after a fracture or surgical intervention. Therefore, a 3D reconstruction technique with conventional CT data might be considered a useful method in evaluating in vivo scapular kinematic alteration after the changes of associated structures of the shoulder joint.
This study had several limitations. First, scapular motions in only two poses (i.e. 0° and 120° forward flexion of the glenohumeral joint) with the patient in prone position for comparative analysis were evaluated; the scapular motion at angles other than the measured positional angles were not analyzed. Second, although the CT images used were fewer than in standard protocol for general diagnostic purposes, risks of radiation exposure with CT could not be avoided. However, the radiation dose required for CT in this study was 1/30 of that required for conventional diagnostic CT with similar accuracy. 30 Third, several factors that could influence scapular kinematics, such as muscular volume and strength were not considered. Finally, although the power analysis indicated sufficient statistical power for the paired t-test, only a small number of patients were enrolled. Therefore, movement changes were not determined according to various implants or disease stages. In future studies, more cases should be studied using the latest two-dimensional and 3D techniques, such as standing CT scanning for various movements. In addition, more precise analyses in accordance with implant type and injury severity would be necessary to overcome the aforementioned limitations.
Conclusions
Data obtained from the 3D reconstruction program showed that rTSA might result in static positional changes and dynamic movement alterations. Internal rotation and anterior tilting in static analyses and upward and external rotation, posterior tilting, and lateral translation in dynamic analyses were detected. This might be associated with an increase in the relative contribution of the scapulothoracic joint to total arm elevation in comparison with that of the glenohumeral joint after rTSA. Orthopedic surgeons should consider kinematic alterations after rTSA for rehabilitation of the shoulder joint.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.