
Abstract
Background:
We intend to assess the efficacies and limitations of collagenase clostridium histolyticum (CCH) and fasciectomy in treating Dupuytren’s contracture, and the associated complications and rate of recurrences aiming to present a treatment algorithm.
Methods:
A literature search within the PubMed, Web of Sciences, Cochrane Library, and EMBASE databases was performed using the combined key words ‘Dupuytren, palmar aponeurosis contracture, collagenase clostridium histolyticum and fasciectomy’, including all possible studies with a set of predefined inclusion and exclusion criteria.
Results:
Thirty studies were assessed for eligibility from 215 identified records. Seventeen publications satisfied the inclusion criteria including 2142 joints in 1784 patients. The mean follow-up time was 18.0 months (3–60).
Conclusion:
Acceptable contractures release was obtained in both techniques. Severe complications associated with fasciectomy outrank those of CCH, whereas the low rate of recurrence favors the fasciectomy technique.
Introduction
Dupuytren’s contracture is a debilitating palmar-digital contracture that results from slowly progressive thickening and shortening of the palmar fascia, particularly of the metacarpophalangeal joint (MCPJ) and the proximal interphalangeal joint (PIPJ). 1 The condition is associated with all race but primarily affects individuals of Northern European descent, with a prevalence rate at 1–7%, 2 and a male predominance with associated risk factors, such as smoking, alcoholism, diabetes, among others. 3 Dupuytren’s contracture (DC) limits the patient’s normal function 4 which is the main cause of seeking treatment. 5 The disease can be classified into proliferative phase, an early onset of the disease where small nodules and lumps appear under the digits of the palmar crease 6 ; involutional phase, the phase in which the condition becomes more extensive and involves the fascia and the digits resulting in the development of cord 7 ; and the residual phase, the collagens proliferate and the cords tightens creating abnormal flexion of the digits and loss of extension. 8 The treatment modalities for DC range from nonsurgical interventions, such as steroid injection, imiquimod, botulinum toxin, needle aponeurectomy, and collagenase injection to surgical options such as partial fasciectomy, dermofasciectomy, radical fasciectomy, and total fasciectomy. 9 The recurrence of DC could be either bilateral 10 or unilateral following treatment or could appear at another anatomical site in the hand. 11 The varying nature of recurrence of the disease compels some patients to opt for further intervention. 12 Therefore, the development of a uniform set of measures to accurately assess functional impairment has proved challenging. 5,13 There are many reports on the treatment outcomes of DC, but treatment options remain controversial. 14 Surgery has been the traditional treatment of choice for patients with this condition for decades 15 from the mildest form to the most severe cases of palmar and digital contractures. 16 Until collagenase clostridium histolyticum (CCH), an injectable enzymatic nonsurgical treatment, was recently approved by the American Food and Drug Administration (FDA). 17 We aim to present the efficacies and limitations of both CCH and fasciectomy in the treatment of DC.
Materials and methods
A literature search was performed within the PubMed, Web of Sciences, Cochrane Library, and EMBASE databases according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The keywords ‘Dupuytren, palmar aponeurosis contracture, collagenase clostridium histolyticum and fasciectomy’ were used for the search to make sure all possible studies were included. Manual searches for references were performed to find potential relevant studies. Two authors separately extracted data from all the articles selected.
All papers reporting data on CCH-treated patient with entry flexion contracture range of ≥20° (20–100) at the MCPJ and ≥20° (20–80) at the PIPJ in the hand; prospective and retrospective case series on fasciectomy with flexion contractures of at least ≥30° at the MCPJ and PIPJ were included; papers comparing both CCH and fasciectomy with flexion contracture ≥20° (20–100) at the MCPJ and PIPJ as an entry criteria were also included. Nonetheless, papers reporting on DC in other parts of the body order than the hand, and those with titles that clearly showed that they were not relevant to the present study were excluded.
Our search was restricted in English, and the references from included articles regarding CCH and fasciectomy in DC management were searched for potential studies.
Included papers were evaluated for the ages of patients, the number of study subjects, the follow-up period, the preoperative and residual flexion contractures at the joints, the recurrence and complication rates. Clinical measurements (preoperative flexion contractures and postoperative extension deficit) and occurrence of complications for different studies were compared with an attempt to provide treatment algorithm of Dupuytren’s contracture at different stages. On the other hand, recurrence with the CCH technique was considered when there was a residual contracture of more than 20° in 3 months, while 12 months follow-up with a postoperative contracture of more than 30° was considered as recurrence for the fasciectomy technique. The random effect model of the meta-analysis was used to determine a summary effect of the two procedures in releasing contractures at the joints before and after treatment (Figures 1 to 4). Data collected on preoperative flexion contractures and postoperative extension deficit at the MCPJ and PIPJ were statistically analyzed and were assumed statistically significant when confidence intervals at 95% for the pooled results were less than 1. The χ 2 (and Fisher exact) test were used to compare the average mild and severe complication rates.
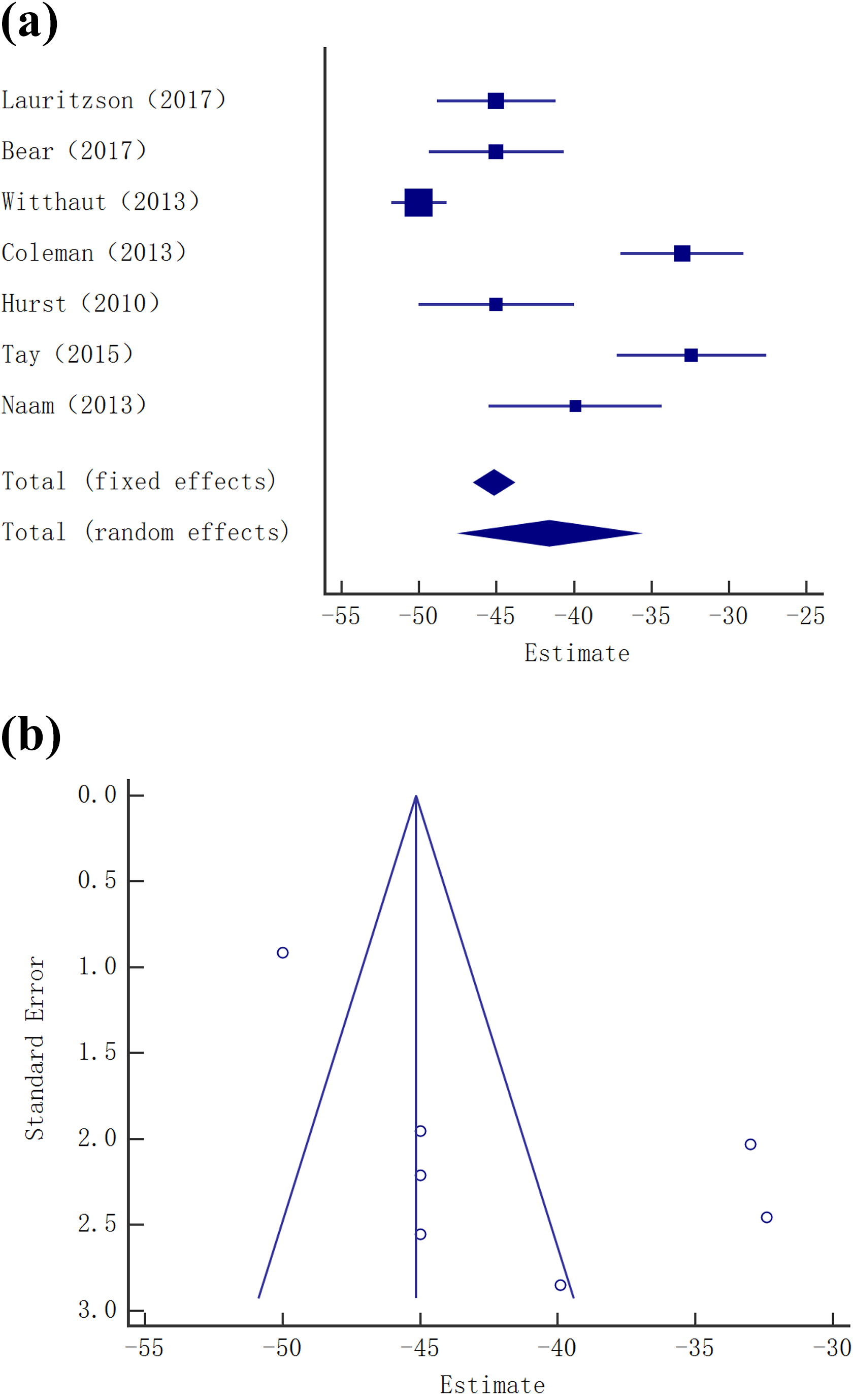
Funnel plot with pseudo 95% confidence limits showing differences between means of contractures at the MCPJ before and after CCH injection. Standard error on the X-axis and the standard mean difference (estimate) between studies on the Y-axis. Forest plot comparing the differences between means for ROM at the joints before and after treatment. CCH: collagenase clostridium histolyticum; MCPJ: metacarpophalangeal joint; ROM: range of motion.

Funnel plots with pseudo 95% confidence limits showing the differences between means of contractures at the PIPJ before and after CCH injection. Standard error on the X-axis and the standard mean difference (estimate) between studies on the Y-axis. Forest plot comparing the differences between means for ROM at the joints before and after treatment. CCH: collagenase clostridium histolyticum; PIPJ: proximal interphalangeal joint; ROM: range of motion.

Funnel and forest plots with pseudo 95% confidence limit showing the differences between means of contractures at the MCPJ before and after fasciectomy. Standard error on the X-axis and the standard mean difference (estimate) between studies on the Y-axis. Forest plot comparing the differences between means for ROM at the joints before and after treatment. MCPJ: metacarpophalangeal joint; ROM: range of motion.

Funnel and forest plots with pseudo 95% confidence limit showing the differences between contractures at the PIPJ before and after fasciectomy. Standard error on the X-axis and the standard mean difference (estimate) between studies on the Y-axis. Forest plot comparing the differences between means for ROM at the joints before and after treatment. PIPJ: proximal interphalangeal joint; ROM: range of motion.
Summary of the CCH technique
CCH as the most effective nonsurgical treatment approved recently by the FDA is an injectable enzyme procedure which can be administered accordingly: a 0.58 mg dose of CCH injection in (0.9% sodium chloride/2 mmol/L calcium chloride) in 0.25 mL diluent for MCPJs and 0.20 mL diluent for PIPJs, and approximately 24 h postinjection, a finger-extension procedure is conducted to facilitate cord disruption. A single shot of the enzyme has adequate time to dissolve certain part of the collagen followed by a finger-extension procedure which consists of manipulation of the treated finger in an attempt to disrupt or distend the cord.
Summary of the surgical technique
Fasciectomy is performed with tourniquet exsanguination and loupe magnification under axillary block or general anesthesia in an operating theater. Cords are approached and excised after Bruner type or longitudinal incisions made along the volar aspect of the digit extending to the palm with Z-plasties. The digital neurovascular bundles are identified proximally, traced distally, and protected with vessel loops. The Dupuytren’s cord is isolated and dissected from proximal-distal, while making sure that the neurovascular bundles and the digital flexor tendon sheath are protected. After excision of the contracted fascia, tourniquet is released and once normal hemostasis is obtained compressive dressing is applied for 2 weeks followed by supervised program of hand therapy with instructed use of removable night splint for 3 months. However, most of these surgeries are associated with serious intraoperative and postoperative complications. 18
Results
A total of 30 studies were assessed for eligibility from 215 identified records. Seventeen publications satisfied the inclusion criteria (as illustrated in the PRISMA flow chart) including 2142 joints in 1784 patients. Of the 17 included studies, eight pertained to CCH, six fasciectomy, and three studies compared the two treatment methods. Four of the eight papers on CCH were randomized controlled trials, three retrospective case series, and one prospective cohort study. Five papers on fasciectomy were retrospective reviews and one prospective cohort study. All the comparative studies were retrospective reviews. The preoperative and postoperative flexion contractures of patients in the two interventions are summarized in Tables 1 and 2. The number of patients, mean ages, the follow-up time, mean preoperative flexion contractures, and mean residual flexion contractures were reported in all the papers. Fifteen (88.23%) of the papers reported rates for specific complications as listed in Tables 3 and 4. Eight (47%) papers reported rate of recurrence; 1678 joints were treated by CCH injection in 1345 patients, 464 joints were treated by fasciectomy in 439 patients. The mean preoperative flexion contractures and postoperative extension deficits in both CCH and fasciectomy studies are illustrated in Table 5. The random effect model summary results for contractures at the joints were −2.277 (95% CI −2.899 to −1.655) at the MCPJ, −1.742 (95% CI −2.387 to −1.096) at the PIPJ in the CCH group; −1.538 (95% CI −1.845 to −1.231) at the PIPJ, and 0.997 (95% CI −1.013 to 3.500) at the MCPJ in the fasciectomy group. Although most of the interval at the MCPJ in the fasciectomy group is below zero, indicating fasciectomy will be most effective at the MCPJ in most settings, the interval overlaps zero and so in some setting fasciectomy may actually be ineffective at the MCPJ. Figures 1 to 4 illustrate the forest and funnel plots of the preoperative flexion contractures and postoperative extension deficits at the MCPJ and PIPJ in both CCH and fasciectomy groups. The total of 1215 complications were recorded for the CCH procedures, 1213 mild and 2 severe complications, whereas 118 mild and 74 severe complications were associated with fasciectomy (p < 0.0001; χ 2 (and Fisher’s exact test)). 6.8% (92/1345) recurrence rate was associated with the CCH group, while 2.3% (10/439) recurrence rate in fasciectomy group (p = 0.0002; Fisher’s exact test) suggests a significant difference in the recurrence rate of the disease.
Number of study subjects, pre-op and post-op mean flexion contractures, study type, and follow-up time.

CCH: collagenase clostridium histolyticum; MCPJ: metacarpophalangeal joint; PIPJ: proximal interphalangeal joint.
Number of study subjects, pre-op and post-op mean flexion contractures, study type, and follow-up time.

CCH: collagenase clostridium histolyticum; MCPJ: metacarpophalangeal joint; PIPJ: proximal interphalangeal joint.
Comparison of severe complications of CCH and fasciectomy.
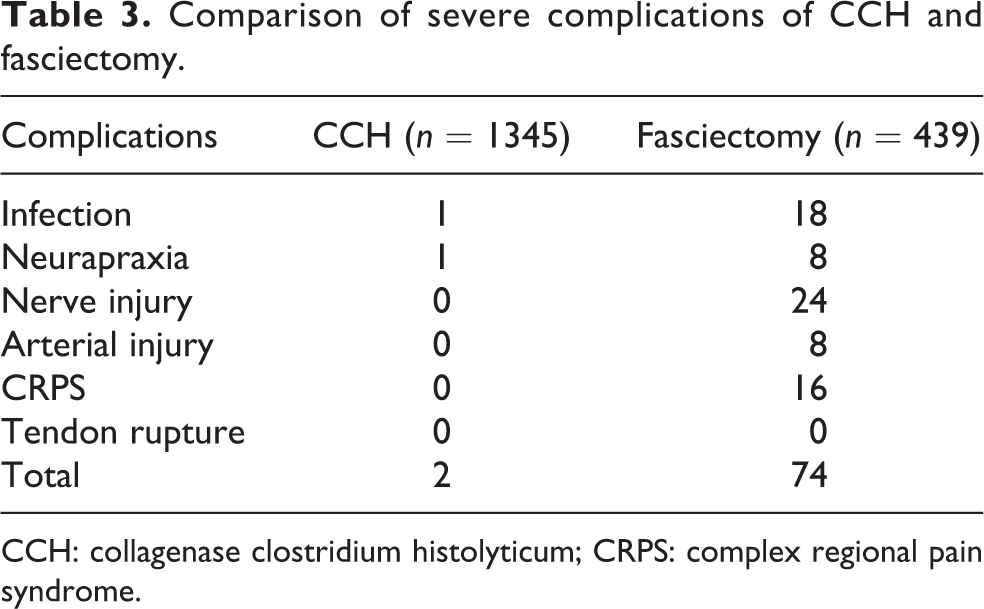
CCH: collagenase clostridium histolyticum; CRPS: complex regional pain syndrome.
Comparison of mild complications of CCH and fasciectomy.

CCH: collagenase clostridium histolyticum.
Comparison of mean preoperative flexion contractures and postoperative extension deficit between CCH and fasciectomy.a

CCH: collagenase clostridium histolyticum; MCPJ: metacarpophalangeal joint; PIPJ: proximal interphalangeal joint.aThe unpaired t test was used to analyze the mean preoperative flexion contractures and postoperative extension deficit. At 95% confidence interval, there was no significant difference in the two groups.
Discussion
The aim of this meta-analysis is to compare the efficacies and limitations of CCH and fasciectomy in releasing joints contractures and the associated rate of complications and recurrences, but it remains a challenge due to the heterogeneity of outcomes measures used for reporting the results of treatments for DC and the challenges faced when attempting to interpret data to determine best practice. 19 However, CCH as a recently developed nonsurgical treatment for DC shows a tremendous comparison to fasciectomy which has been the standard against which the results of all other techniques ought to be compared. 20 Determining a superior treatment method and an exact indication for the use of a specific treatment is controversial because different studies used different scoring measures for outcomes. 21 The scoring methods used in these studies included preoperative and postoperative flexion contractures, Disabilities of Arm, Shoulder and Hand (DASH) score, Quick DASH, patient evaluation method, Michigan Hand Outcomes Questionnaire, propensity score matching, visual analogue scale, and so on. 22 All studies included did not use the same scoring system and as a result direct comparison was not always possible. 23 However, the most popular scoring system was the preoperative and postoperative flexion contractures that was used by all studies and as such a direct comparison was possible 24 (Tables 1 and 2). The parameters of preoperative flexion contractures and postoperative extension deficits, occurrence of complications and rates of recurrence were the foci of comparison between these techniques. 25 Regardless of the disparities in complications evaluation, 26 DASH score was adopted for all the studies with statistical analysis of the complications, thus enabling comparison of severe and mild complications in both groups. 27 Zhou et al. in a comparative study of CCH and limited fasciectomy concluded that severe complications were non-transient or required an intervention and the mild complications were transient and do not required intervention. 1,28 The most common mild complications associated with both procedures were edema and contusion. 29 For the CCH injection, the occurrence of edema was 535 and contusion 340, while edema and contusion in the fasciectomy group were 51 and 42, respectively, illustrating no statistical difference. 30 However, the severe complications reported for the fasciectomy group were as high as 74, while 2 severe complications were recorded for the CCH group which indicates an increased rate in severe complications in fasciectomy. 31,32 For the CCH, postinjection manipulation will rupture the pathological cord but not the periarticular adhesion that is occasionally encountered in the PIPJ. 33 CCH is a simple and efficacious outpatient technique that has a low risk of severe complications but higher recurrence rate, as opposed to higher rate of severe complications and lower rate of recurrence with fasciectomy. 34 Eberlin et al. in their series of 11 patients with mean age 69 (52–76) reported recurrence of DC in all the patients after CCH treatment, but there was no recurrence in the same group of patients after fasciectomy at 16 months follow-up. The postinjection contractures were 42° at the MCPJ and 60° at the PIPJ, and postoperative contractures at MCPJ was 0° and 21° at the PIPJ emphasizes the point by Witthaut et al. when they suggested that CCH as a minimally invasive procedure is particularly effective when administered at joints with less severe contracture. 32 Nonetheless, the higher severe complication rate in fasciectomy is difficult to be avoided especially in the PIPJ because this joint is found in ‘no man’s land’ in zone II of the volar palm where the skin is tightly adhered to the underlying structures leaving them vulnerable to a higher risk of injury during the surgical procedure. 35 The most reported severe complications are nerve injury, arterial injury, complex regional pain syndrome, and infection, 36 while edema, contusion, pain, swelling, and hematoma were frequently reported mild complications. 7,23
DC is a progressive condition that can be classified into three stages. 15,18 Each stage being associated with specific characteristic that makes one treatment technique a better option. Treatment protocol varies at different stage of the disease. In an early stage of the disease, a single shot of the enzyme is adequate, but 2–3 injections spread over months are required when the disease has advanced. Notwithstanding, surgery as the traditional treatment technique can become a controversial issue on when it is necessary in terms of joint contracture. It has been reported that a contracture of ≥30° at the MCPJ and any contracture at the PIPJ warrant a surgical intervention, on the contrary, McGrouther had different view and he stated that it is better to “rely on functional difficulty and the rate of progression of the disease as an indication for surgery, rather than choosing a set amount of joint contracture.” 37 The aim of this treatment approach is to remove the diseased fascia and obtain acceptable function of the hand with the hope of avoiding recurrence of the disease, but a successful surgery does not guarantee that there will be no associated complications. In stage I (the proliferative phase), the disease is characterized by a painless nodule in the palmar surface of the hand. 27 This stage is difficult to diagnose because in most patients it has no effect on hand function and the Hueston table top test is always negative and the disease is often not treated. 10,26 The disease is only treated in stage I if the patient’s function is impaired, and CCH is more favorable at this stage than a complicated open surgical procedure. Stage II (the involutional phase), the disease spread into the fingers resulting in the development of a cord. Myofibroblasts are the predominant cell type during this stage and they align themselves along tension lines within the nodules. 17,29 The disease is diagnosed by the positive Hueston table top test. The rates of complication and recurrence at this stage are minimum making CCH the better option. 16 Tightening of the cord which creates the abnormal digital and palmar contractures usher in stage III of the disease which is confirmed by a positive Hueston table top test. 16,19 Stage III is an indication of both treatment methods. Fasciectomy, on the other hand, is a better treatment option of the disease when joint contracture is severe and if there is a recurrence of the disease after failed CCH treatment. 38,39 Based on the reporting data, CCH, a nonsurgical enzymatic injection that can be administered as an outpatient procedure, is indicated at any stage of the disease but can be more effective to joints with less severe contractures rather than the delayed treatment for DC until contracture becomes severe enough to prompt traditional surgical intervention. 32,38,39 CCH and fasciectomy provide acceptable contracture release at the joints, notwithstanding, less occurrence of severe complications favors CCH technique while low rate of recurrence favors the fasciectomy technique. 12,13
This review like many others has limitations that have to be considered when evaluating the information and conclusion drawn. The heterogeneity of outcome measures and the lack of enough comparative studies, and the high disparity in population size is notable.
Conclusion
Both techniques show acceptable results in releasing DCs. However, the CCH technique is associated with low rate of severe complications but high recurrence rate, while low risk of recurrence favors the fasciectomy at the expense of high rate of severe complications.
Footnotes
Acknowledgements
The authors thank Dr Mandika Chetry for English revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Zhejiang Provincial Natural Science Foundation of China (grant no. LY18H060010) and the Project of Administration of Traditional Chinese Medicine of Zhejiang Province of China (2018ZB079).