
Abstract
Background:
Deep vein thrombosis (DVT) and pulmonary embolism (PE) cause significant morbidity and mortality following arthroplasty. A seasonal variation in the rate of PE in arthroplasty patients in the northern hemisphere has been reported. We hypothesized that there would be a similar seasonal variation in arthroplasty patients in Australia.
Methods:
We performed a retrospective review of all patients who received primary and/or revision arthroplasty of the hip or knee over a 15-year period (2000–2015) across Western Australia. We identified all patients who were diagnosed with DVT and/or PE according to International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification codes. The incidence of venous thromboembolic (VTE) disease was calculated as the proportion of operations that led to this complication per 3-month seasonal period.
Results:
A total of 12,507 total hip arthroplasties (THAs) and 8899 total knee arthroplasties (TKAs) were recorded during the study period. There was a total of 274 DVT and/or PE among the combined total of 21,406 hip and knee arthroplasties performed between 2000 and 2015. There was a significantly higher rate of VTE for females than males (odds ratio (OR): 1.33, 95% confidence interval (CI): 1.03–1.71, p = 0.0293), for TKA than THA (OR: 1.60, 95% CI:1.26–2.03, p < 0.0001) and in winter than other seasons (OR: 1.51, 95% CI: 1.14–2.01, p = 0.0047).
Conclusion:
There is a statistically significant increase in the incidence of VTE in arthroplasty patients during the winter months in Western Australia. This finding is the first of its kind for patients in the southern hemisphere and corroborates previous studies in the northern hemisphere.
Keywords
Introduction
Deep vein thrombosis (DVT) and pulmonary embolism (PE) remain significant causes of morbidity and mortality following arthroplasty of the hip and knee. The literature is replete with studies examining the venous thromboembolic (VTE) risk factors and documenting the development of effective prophylaxis and treatment regimes. The British Orthopaedic Association, American Academy of Orthopedic Surgeons and the Australian Orthopaedic Association all provide guidelines for pharmacological and mechanical prophylaxis of VTE based on an individual patient’s risk. 1 –3 These guidelines do not consider a potential seasonal variation of VTE risk for arthroplasty patients despite seasonal variation of both DVT and fatal PE having been documented in non-arthroplasty populations. 4,5 Previously, Wroblewski et al. have demonstrated a seasonal variation in the rate of PE in post-arthroplasty patients in the United Kingdom. 6 We hypothesized that, similar to the northern hemisphere, there would be a seasonal variation in the incidence of both DVT and/or PE in total hip arthroplasty (THA) and total knee arthroplasty (TKA) patients in Western Australia. The aim of this study was to investigate whether any seasonal trend in incidence of DVT or PE is identifiable, using data from THA and TKA patients over a 15-year period in five major teaching hospitals in Perth, Western Australia.
Patients and methods
All patients who are admitted to any hospital in Western Australia have details of their admission recorded centrally by the state Health Department. These records are routinely linked so that, since approximately 1980, all admissions for the same patient (across all different hospitals) are identified as belonging to the same person. Details of each admission include demographic data, initial diagnoses and comorbidities as well as details of any operations and subsequent complications. Diagnoses and procedures are coded according to the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM) and recorded on a single centralized database. Records selected for this study included admissions for THA and/or TKA at all public hospitals performing arthroplasty in Western Australia.
Utilizing this comprehensive database, we performed a retrospective review of all patients who received primary and/or revision arthroplasty of the hip or knee over a 16-year period from January 2000 to December 2015. We audited all patients who underwent THA or TKA and identified those patients who were subsequently diagnosed with and/or treated for either DVT or PE or simultaneous DVT and PE (VTE) (ICD-10-AM codes: I26.0, I26.9, I80.1, I80.2, I80.3, I80.8, I80.9) in the first 3 months following surgery. There were no exclusions. As this study was particularly aimed at examining any trend in DVT or PE incidence, we examined limited information from the database, including only the age and gender of the patient, the month and type of surgery (hip/knee), and date of hospital discharge. The overall incidence of DVT/PE or VTE was calculated as the proportion of operations that led to this complication per 3-month seasonal period. The seasons were defined by grouping the calendar months; spring: the transition months September, October and November; summer: the three hottest months December, January and February; autumn: the transition months March, April and May; and winter: the three coldest months June, July and August. 7 In symptomatic patients, diagnosis of DVT was made by venous ultrasonography; diagnosis of PE was made by ventilation perfusion (VQ) study or by computed tomographic pulmonary angiography; and routine post-operative screening of all post-arthroplasty patients was not undertaken. Rates of DVT, PE and VTE were calculated and presented in graphical form covering the study period as monthly difference in incidence consistent with previous studies. 8
Statistical analysis
Chi-square statistics were used to compare the rates of each of the outcomes between the levels of each of the independent variables. Independent variables included gender and age of the patient as well as the type (TKA/THA), season and year of the operation. Four separate year groups containing similar numbers of operations were formed (2000–2005, 2006–2009, 2010–2012 and 2013–2015). The rates of each outcome within each year group were calculated. By grouping the year of operation in this manner and treating the group as a category, there was no assumption made that any trend over time would be linear. A logistic regression model was used to explore any relationship between the season and the risk of developing DVT and/or PE, after adjustment for the all other independent variables (regardless of their significance on univariate analysis). The model was fitted firstly using DVT and PE as separate outcomes, then repeated using the combined VTE as the single outcome variable. The most parsimonious model for each outcome was identified using a ‘backwards-elimination’ strategy, whereby the least significant variable was dropped from the multivariate model (one at a time), until all variables remaining in the model were significantly associated with the outcome. Statistical analyses were performed using the SAS version 9.2 software (SAS Institute Inc, Cary, North Carolina, USA, 2008), and a p-value < 0.05 was taken to indicate a statistically significant association in all tests.
Results
There were 12,507 THAs and 8899 TKAs recorded during the study period in 13,074 females (61%) and 16,417 (76%) patients <80 years old (Table 1). There were 140 patients in whom a DVT occurred, 147 in whom a PE occurred and 274 in whom simultaneous DVT and PE (VTE) occurred; an overall prevalence of 1.28% of the 21,406 THA and TKA patients identified during the study period (Figure 1). Univariate analysis demonstrated significant differences in VTE rates between gender (females higher than males), operation type (TKA higher than THA) and season (winter highest, summer lowest) (Table 1).
Demographic characteristics and raw incidence data for DVT, PE and combined VTE.a
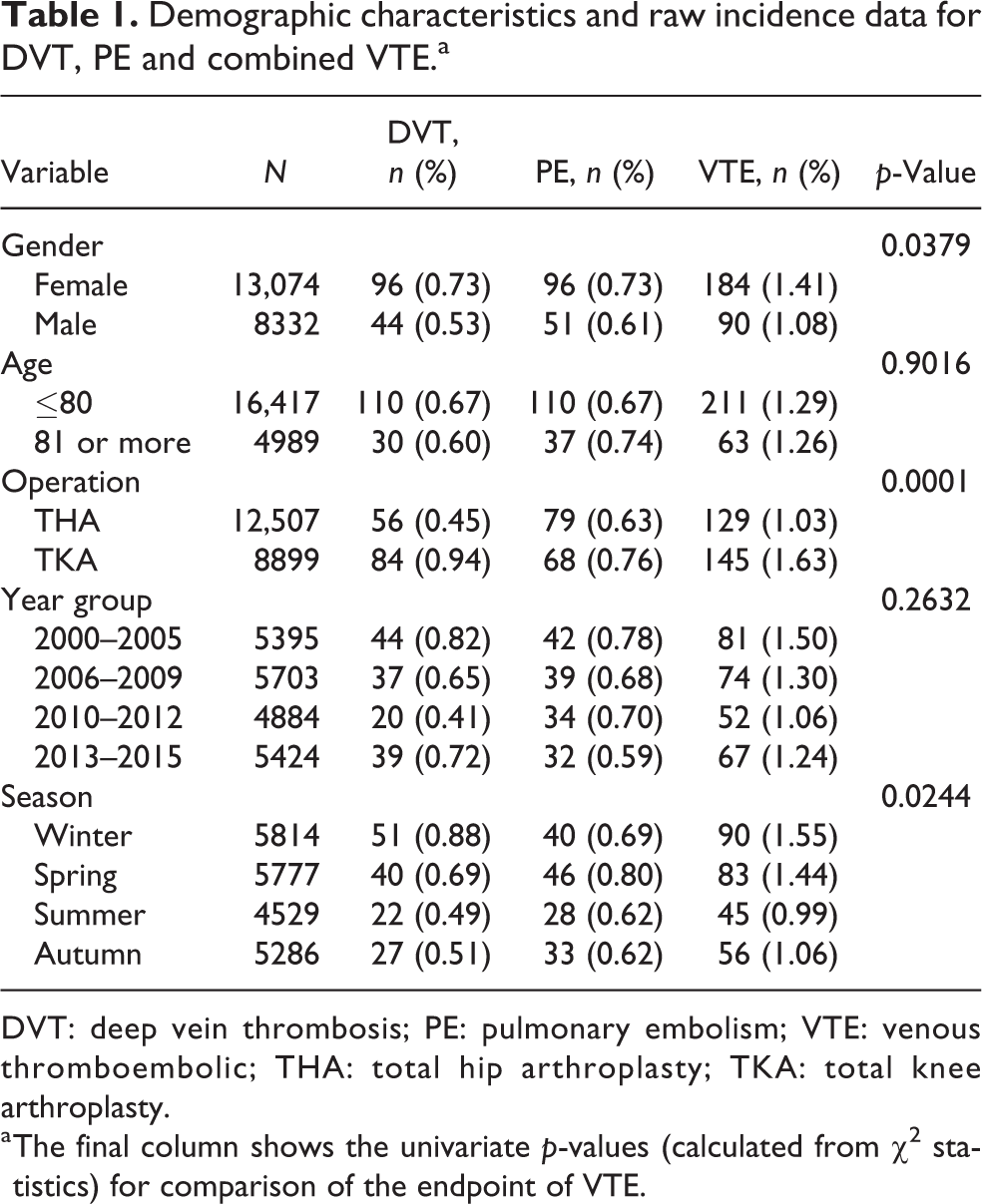
DVT: deep vein thrombosis; PE: pulmonary embolism; VTE: venous thromboembolic; THA: total hip arthroplasty; TKA: total knee arthroplasty.
a The final column shows the univariate p-values (calculated from χ 2 statistics) for comparison of the endpoint of VTE.

Season variation in the incidence of DVT, PE and VTE (combined), trends analysed according to the percentage monthly difference for 5-year time periods: (a) 2000–2005, (b) 2005–2010, and (c) 2010–2015. DVT: deep vein thrombosis; PE: pulmonary embolism; VTE: venous thromboembolic.
Multivariate logistic regression analysis demonstrated no association between the age and the rates of DVT, PE or VTE and no apparent trend changes emerging over time when analysed by year group; consequently, these variables were dropped from the model. Likewise, there was no difference in the rate of VTE between summer and autumn, so these groups were amalgamated. Consistent with the univariate analyses, the final multivariate model showed that there was a significantly higher rate of VTE for females than males (odds ratio (OR): 1.33, 95% confidence interval (CI): 1.03–1.71, p = 0.0293), for TKA than THA (OR: 1.60, 95% CI: 1.26–2.03, p < 0.0001) and in winter than summer/autumn (OR: 1.51, 95% CI: 1.14–2.01, p = 0.0047) (Table 2).
Multivariate logistic regression analysis.a
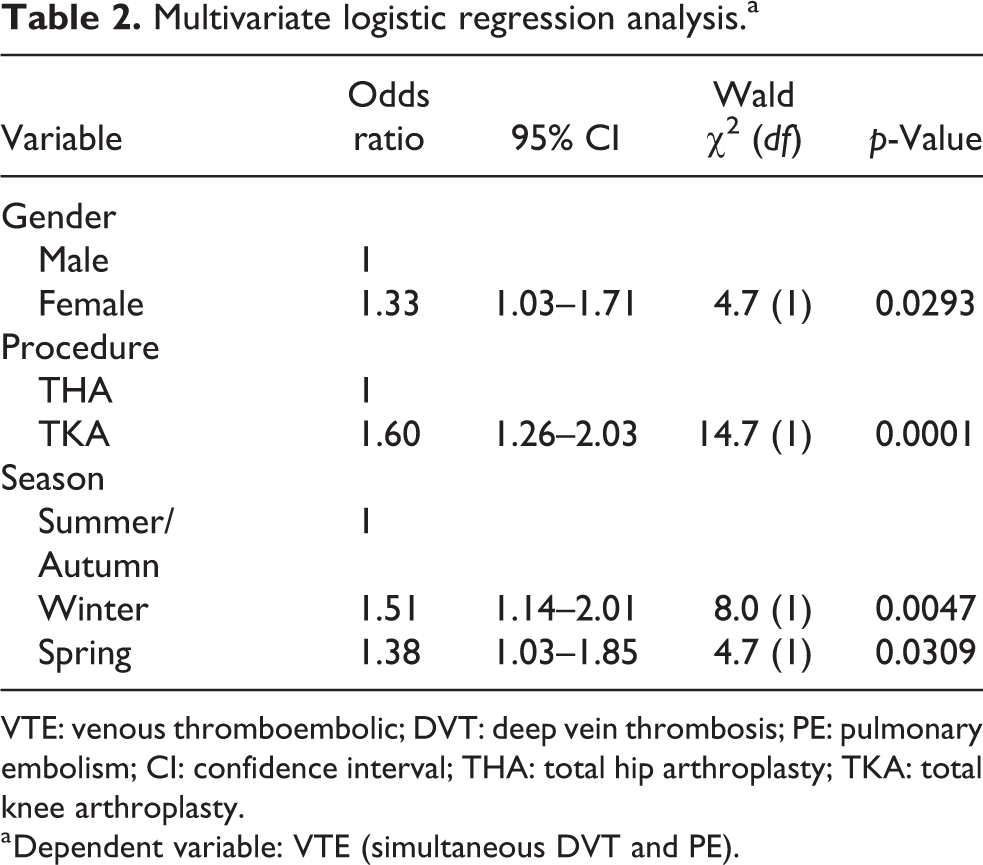
VTE: venous thromboembolic; DVT: deep vein thrombosis; PE: pulmonary embolism; CI: confidence interval; THA: total hip arthroplasty; TKA: total knee arthroplasty.
a Dependent variable: VTE (simultaneous DVT and PE).
Logistic regression analysis for DVT alone demonstrated a similar result to the VTE analysis (Table 3), with a near significant higher rate of DVT for females than males (OR: 1.43, 95% CI: 1.00–2.04, p = 0.0511) and a significantly higher rate of DVT for TKA than THA (OR: 2.15, 95% CI: 1.53–3.02, p < 0.0001) and in winter than all other months (OR: 1.56, 95% CI: 1.10–2.20, p = 0.0123) (Table 3.). Logistic regression analysis of PE as a separate endpoint showed no statistically significant association between any independent variables; the incidence of PE was similar for males versus females, for both THA versus TKA and across all seasons.
Multivariate logistic regression analysis.a
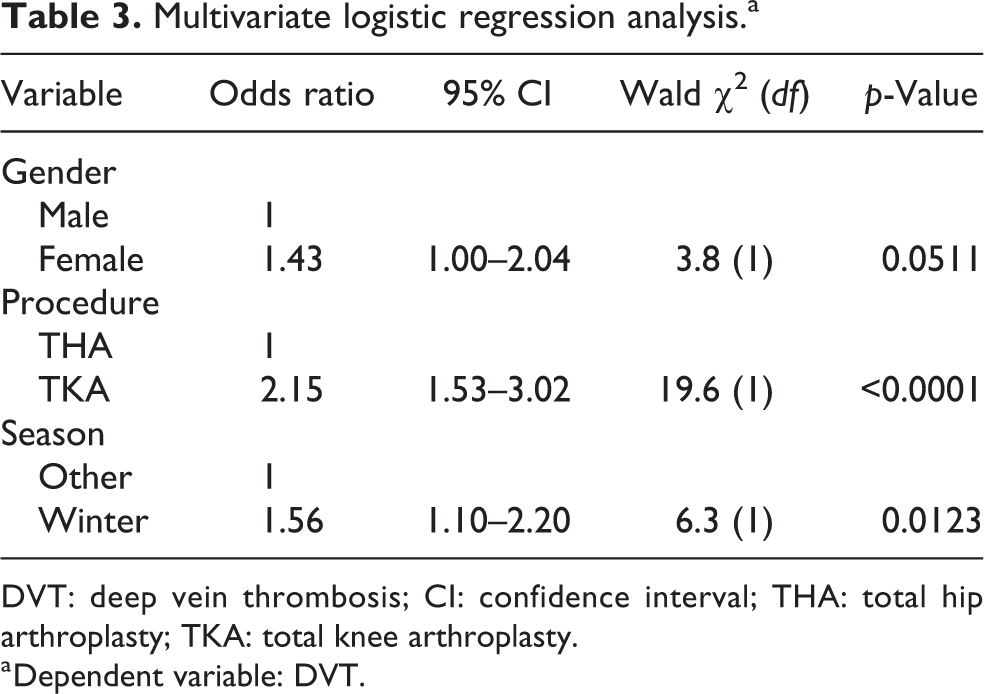
DVT: deep vein thrombosis; CI: confidence interval; THA: total hip arthroplasty; TKA: total knee arthroplasty.
a Dependent variable: DVT.
Discussion
There have been no previous reports documenting seasonal variation in the incidence of VTE either in temperate climate zones or in the southern hemisphere. Previously, Boulay et al. analysed hospital admissions for the incidence of DVT and PE in France over 4 years and demonstrated that clear seasonal variations exist with an increased incidence in the winter months. 8 Likewise, Dentali et al. conducted a systematic review and meta-analysis examining the seasonal and monthly variation in the incidence of VTE; they analysed 17 studies including in excess of 35,000 patients, finding a seasonal variation in 12 studies and a monthly variation in 10 studies; none of which were conducted in the southern hemisphere. Their meta-analysis demonstrated a significantly increased incidence of VTE in winter (χ 2 = 146.04, p < 0.001), with a relative risk (RR) of VTE of 1.143 (99% CI: 1.141–1.144), and a significantly increased incidence of VTE in January (χ 2 = 232.57, p < 0.001) with an RR of VTE of 1.194 (99% CI: 1.186–1.203). 9 In the arthroplasty-specific setting in the United Kingdom, Wroblewski et al. retrospectively examined 18,104 patients post Charnley hip arthroplasty demonstrating a significant difference between the incidences of fatal PE during the colder months (1%) in comparison with the remainder of the year (0.42%). 6,10
O’Reilly et al. examined the prevalence of VTE after hip and knee replacement surgery in Australia using ultrasonography to examine all patients undergoing THA, TKA or bilateral TKA in a large orthopaedic centre. 11 All patients received both mechanical and chemoprophylaxis and all patients (both symptomatic and asymptomatic) were screened prior to discharge. From their cohort of almost 6000 patients, the pre-discharge prevalence of DVT was 8.9% for THA, 25.6% for TKA and 36.9% for bilateral TKA. The prevalence of symptomatic non-fatal in-hospital PE was 1.9%, while the prevalence of fatal in-hospital PE was 0.05%. No mention of a variation in the seasonal or monthly incidence was reported. 11 The primary explanation for the larger incidence of VTE in the previous cohort may be methodological; as detailed earlier, this study screened all patients using ultrasonography following THA and TKA thereby detecting both symptomatic and asymptomatic patients. 11 By comparison, routine post-operative screening of all arthroplasty patients was not performed on our cohort, and only symptomatic DVT/PEs were detected, which may underestimate the true incidence in our study population.
These data demonstrate a seasonal variation in the incidence of post-arthroplasty VTE in the southern hemisphere. In the northern hemisphere, the cause of a seasonal variation in VTE incidence has been hypothesized to be due to a complex interplay of factors including colder temperatures potentially leading to vasoconstriction in the lower limbs and/or shorter daylight hours that can lead to a reduction in the amount of physical activity. 6,10 As the climate in Perth, Western Australia is considered warm temperate and/or Köppen climate-type warm-summer Mediterranean, the seasonal trend identified in hypercoagulability may be independent of the effect of colder northern hemisphere temperatures. Seasonal fluctuations in coagulation, possibly due to the influence of community acquired upper respiratory tract infections, are currently areas for further study. 7,12
Limitations
Utilizing pooled, centralized, retrospective data from the state health service combines information from multiple providers and enables large numbers of patient records to be interrogated for this study. However, the quality of the data depends ultimately on the correct diagnosis being made by treating physicians. Underreporting of asymptomatic, misdiagnosed or missed presentations may therefore have limited the overall number of patients; however, it is unlikely that these limitations would have a seasonal variation component. Likewise, across the multiple sites and institutions during the study period, there was no standardized state-wide anticoagulation prophylaxis regimes, measure of baseline activity or rehabilitation programs for post-operative management of THA or TKA arthroplasty patients. Finally, the overall incidence of VTE is relatively low, such that a statistically significant difference in seasonal incidence may not translate to a clinically meaningful difference.
Conclusion
This study demonstrates a statistically significant increase in the incidence of VTE in THA and TKA patients during the winter months in Perth, Western Australia. This finding, in a temperate climate region of the southern hemisphere, confirms the findings of previous studies in the northern hemisphere. These results may have implications for high-risk patients who may require consideration for either the timing of surgery or additional mechanical or chemical thromboembolic prophylaxis during the higher risk season. Further studies with prospective data aimed at elucidating the complex multifactorial aetiology of this now established phenomenon are indicated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.