
Abstract
Morquio syndrome is a relatively rare entity that is often associated with atlantoaxial instability from early childhood due to odontoid dysplasia based on a mucopolysaccharoidal disorder. Here, we present the case of a 55-year-old male patient with Morquio syndrome who developed cervical myelopathy, which is an extremely rare condition in the older population. Myelopathy developed gradually with upper-limb paresthesia and clumsiness of both hands. The patient had a characteristic “gargoyle-like” coarse face with a trunk shortening-type short stature. Imaging of the cervical spine demonstrated several problems, including diminutive structures called platyspondyly with small pedicles and fragile bone quality, hypoplasia of the C1 posterior arch that migrated into the spinal canal, and os odontoideum with atlantoaxial instability. With intraoperative navigation guidance, posterior decompression of C1 followed by occipito-cervico-thoracic spinal fusion was successfully performed in this complicated case. Clinical and radiographic outcomes were both excellent and have been maintained for 2 years postoperatively.
Introduction
Morquio syndrome, or mucopolysaccharidosis type IV (MPS IV), is a rare autosomal recessive hereditary disorder. Morquio syndrome is often associated with odontoid dysplasia, which tends to lead to atlantoaxial instability and spinal cord compression, causing cervical myelopathy from early childhood. We encountered an extremely rare case of Morquio syndrome in the 5th decade of life, with cervical compressive myelopathy due to atlantoaxial instability and indentation of the posterior arch of the atlas that required posterior decompression and occipito-thoracic fusion.
Case presentation
History and physical examination
A 55-year-old male visited our hospital with complaints of progressive clumsiness and numbness of both hands. He had been diagnosed with Morquio syndrome at another hospital when he was 3 years old. With age, the patient developed short stature, deformity of the chest, and walking difficulty. He walked using crutches due to the progression of deformity of his upper and lower extremities. He graduated from school and university without learning difficulties, and he has worked as a staff member of a securities company, suggesting his intellectual ability is normal. At the age of 54 years, he became aware of upper-limb paresthesia and clumsiness of both hands while typing at a keyboard during routine work. He was referred to our hospital by his personal physician for close examination and treatment.
On examination, body height was 130 cm and the patient had a trunk shortening-type short stature. Skeletal abnormalities were a severe thoracolumbar kyphosis, pectus excavatum, and bilateral genu valgum. A characteristic “gargoyle-like” coarse face with marked craniofacial proportion mismatch, thick lips, and a flat nose was observed. The patient had reduced sensory perception in the right forearm. Deep tendon reflexes were promoted in both upper and lower limbs bilaterally, and a 10-second grip and release test gave a result of only 10 times (normal: over 20 times) each for both hands. The Japanese Orthopedic Association (JOA) score for cervical myelopathy was 10.5 points (full score: 17 points). No data for the urinary mucopolysaccharide level were available.
Imaging studies
Full-length standing posteroanterior and lateral radiographs of the spine demonstrated a totally osteoporotic platyspondyly and an anterior beaking appearance of the thoracolumbar vertebrae, resulting in gibbus deformity (Figure 1). Hip, knee, and wrist joint radiographs showed severe arthritic changes with coxa valga, genu valgus, and Madelung-like deformity, which are all characteristic manifestations of Morquio syndrome (Figure 2). A flexion-extension lateral myelogram and subsequent computed tomography (CT) revealed kyphotic cervical malalignment with flattened vertebral bodies, small pedicles, hypoplasia of the C1 posterior arch that migrated into the spinal canal, and os odontoideum, showing atlantoaxial instability. Cervical kyphosis is reducible by neck extension (Figure 3). CT angiography confirmed a bilateral high riding vertebral artery (VA). T2-weighted cervical magnetic resonance imaging demonstrated compression of the spinal cord due to indentation of the posterior arch of C1 and intramedullary high-intensity changes at the C1–2 level (Figure 4).

Full-length standing posteroanterior (left) and lateral (right) radiographs of the spine on admission. A bell-shaped chest wall (left), totally osteoporotic platyspondyly, and anterior beaking of the thoracolumbar vertebrae resulting in gibbus deformity (right) were observed. The Cobb angle of the thoracolumbar (T11/L2) kyphosis was 83°. Note that the thoracolumbar kyphosis was compensated by flexion of the hip joints. These features are characteristic manifestations of Morquio syndrome.
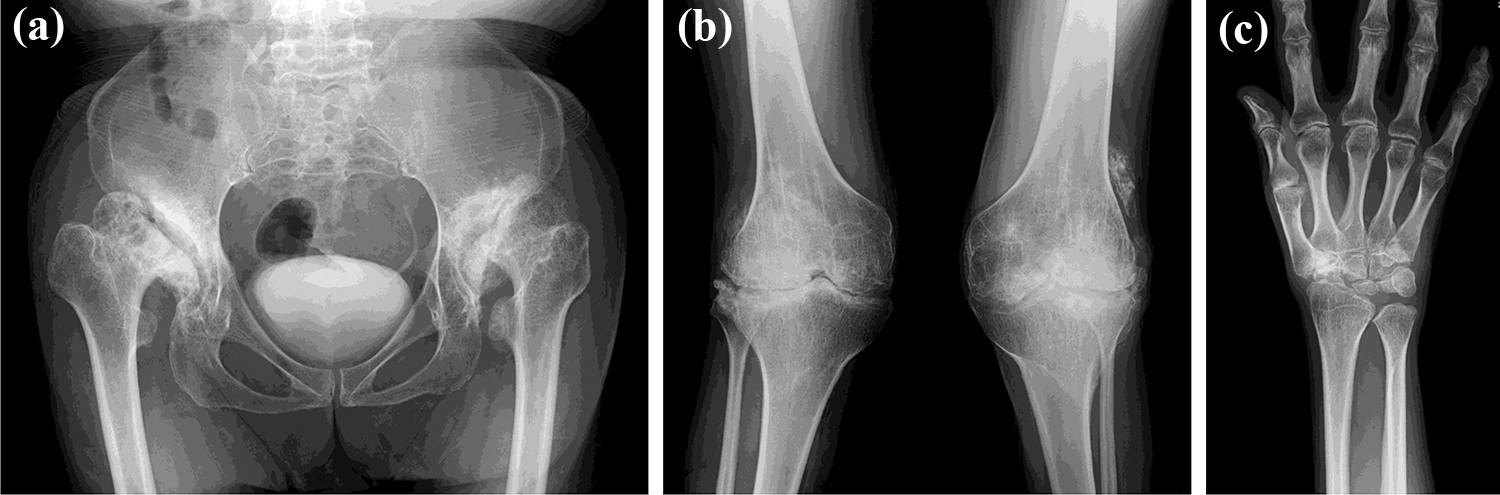
Plain radiographs of the hip (a), knee (b), and wrist joint (c) on admission. Marked osteoarthrosis with coxa valga (a), genu valgus (b), and Madelung-like deformity with irregular carpal bones (c) were observed, which are all characteristic manifestations of Morquio syndrome.
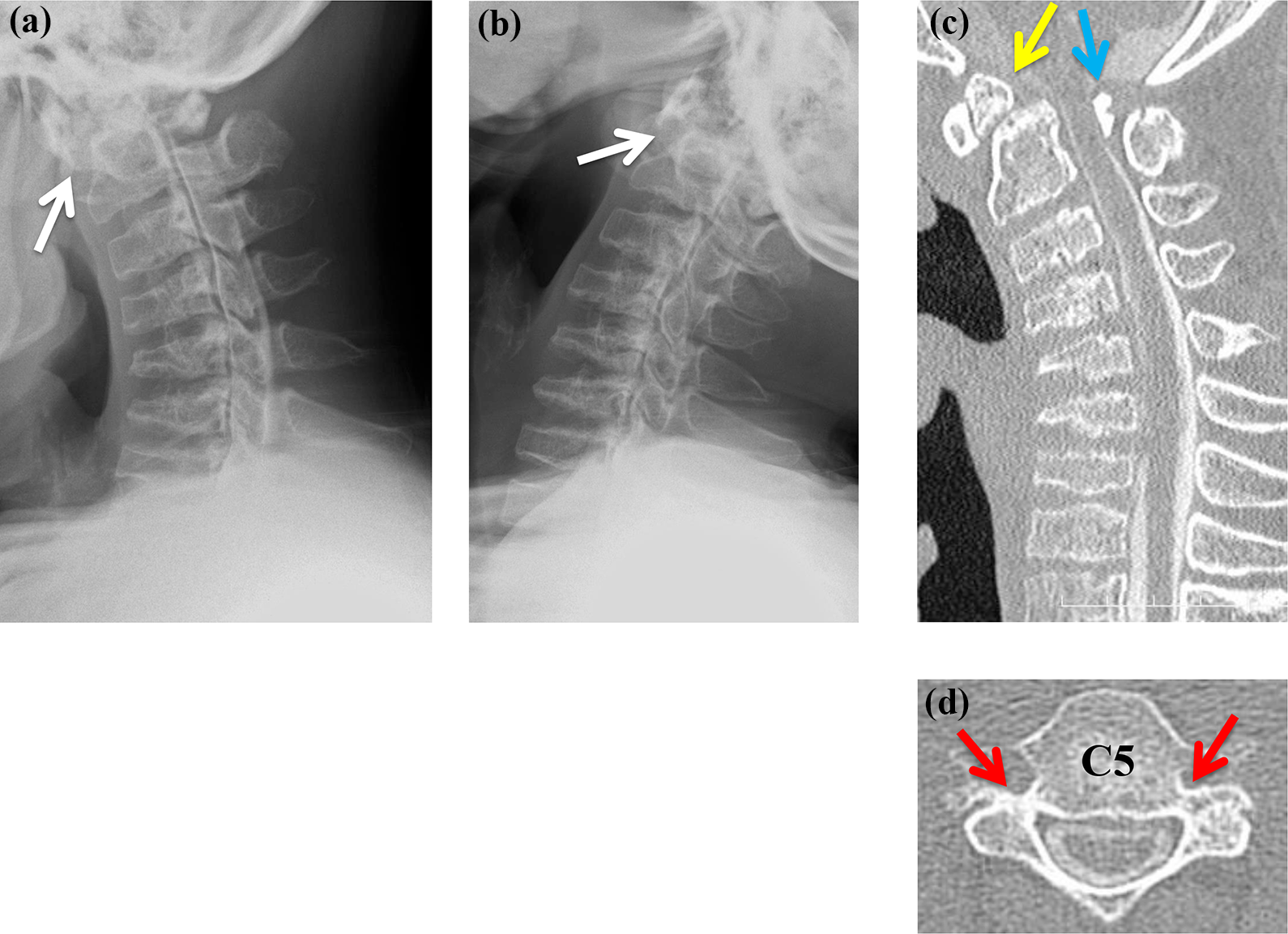
Flexion-extension lateral view on a myelogram ((a) and (b)) and subsequent CT ((c) and (d)) before surgery. (a) The ADI increased to 5 mm with forward bending. (b) ADI decreased to 2 mm with neck extension. White arrows indicate ADI. (c) A sagittal reconstruction CT myelogram clearly demonstrated kyphotic malalignment with flattened vertebral bodies, hypoplasia of the C1 posterior arch that indented into the spinal canal (blue arrow), and os odontoideum (yellow arrow). (d) Horizontal section of the CT myelogram at the C5 level. Red arrows indicate small and narrow pedicles. CT: computed tomography; ADI: atlantodental interval.

T2-weighted cervical MRI (left: mid-sagittal section, right: axial section of C1) before surgery. The red arrow indicates indentation of the posterior arch of C1 that compressed the spinal cord, and the intramedullary signal intensity at the C1–2 level was slightly high. Total platyspondyly of the cervical spine was also observed. MRI: magnetic resonance imaging.
Operative treatment and postoperative course
Based on the imaging findings above, we performed a posterior decompression and occipito-thoracic fusion under the assistance of intraoperative cone beam CT (Siemens, Arcadis Orbic 3D, Munich, Germany) and a navigation system (Medtronic Sofamor Danek, Stealth Station Seven, Memphis, Tennessee, USA). After C1 posterior arch resection, an occipital plate, C2 intralaminar screws, C4–5 lateral mass screws, and T1–3 pedicle screws were carefully placed bilaterally. Cervical pedicle screws were not used because all pedicles of the cervical spine including C2 were too small to pass through. Cervical kyphosis was corrected using tapered shaped rods with the application of a cantilever force, followed by enriched autogenous iliac bone grafting. Based on preoperative radiographic evaluation on a flexion-extension lateral myelogram (Figure 3), facetectomy was not performed because the cervical spine was considered flexible enough to obtain lordosis. No marked adverse event occurred on electrical neuromonitoring (both somatosensory-evoked and motor-evoked potentials) during surgery. On day 2 after surgery, ambulation using a wheelchair was achieved, and the patient started walking training 1 week after surgery. He was discharged from hospital walking with a crutch at 4 weeks after surgery and resumed his normal activities immediately. No cervical orthosis was used during the postoperative course. At the time of latest follow-up (2 years after surgery), the JOA score had improved to 14 points and motor skills such as typing and using chopsticks were improved, despite mild numbness remaining in the right fingers. Radiographs of the whole spine at 2 years postoperatively showed no mechanical or instrumentation failures such as rod breakage, screw loosening, or distal junctional kyphosis (Figure 5).

Full-length standing anteroposterior (left) and lateral (right) radiographs of the spine 2 years after surgery. Although gibbus deformity remained without aggravation, no instrumentation failures such as rod breakage, screw loosening, and distal junctional kyphosis were observed around the fusion area.
Discussion
Morquio syndrome is a rare lysosomal disease that is classified into MPS IV. This syndrome manifests as N-acetylgalactosamine-6-sulfate sulfatase-deficient type A and β-galactosidase-deficient type B. 1 The incidence of MPS IV varies in different reports from one out of 76,000 to 450,000 people, and the life expectancy in patients with the severe form is as short as 20 or 30 years. 2,3 Rarely, patients with a more slowly progressing phenotype survive beyond 60 years, and symptomatic treatment is generally provided according to the severity of each case due to the lack of consensus treatment for the disease. 4
The incidence of odontoid process dysplasia associated with Morquio syndrome is relatively high 2,4 and is well correlated with atlantoaxial instability. 5 The mechanism of the cervical cord disorder in patients with Morquio syndrome is multifactorial and includes thickened soft tissues around the odontoid process caused by atlantoaxial instability, accumulation of glycosaminoglycan around the odontoid process, and flaccid spinal ligaments. 3,6 –8 Under these circumstances, repetitive minor trauma of the cervical region during activities of daily living may gradually affect the cervical cord. 9 In cases in which cervical cord disorder is thought to be caused by atlantoaxial instability, posterior fusion may be effective. 10
A literature search showed mostly good results for posterior occipito-C2 fusion and external fixation without use of spinal instrumentation because most of these surgeries were performed in pediatric patients. 10 –18 This tendency might be related to the short life expectancy of patients with Morquio syndrome due to respiratory or cardiac failure, which is chronically aggravated by paralysis of the respiratory muscle. 3,4 To the best of our knowledge, there is no report of a surgically treated cervical pathology in patients with Morquio syndrome older than 50 years. We speculate that atlantoaxial instability and spinal canal stenosis in our patient were relatively mild, and thus degenerative changes of the cervical spine and spinal cord damage might have developed gradually until his 50s.
In cases in the literature, almost all surgically treated patients had halo-vest fixation for a few months postoperatively. 10 –18 However, there are some drawbacks of long-term rigid external neck fixation, including muscle atrophy, neck contracture, and mental distress. Current surgical techniques for the cervical spine and contemporary spinal implants make it possible to avoid the use of a halo-vest postoperatively. Consequently, we performed posterior decompression and internal fixation under intraoperative navigation guidance. Given that our patient had a high riding VA, flattened cervical vertebra with small and narrow pedicles, and poor bone quality, it was difficult and risky to insert pedicle screws as rigid anchors in cervical vertebrae. Therefore, alternative intralaminar and lateral mass screws were used, and the fusion area was extended to the upper thoracic spine to avoid serious screw complications. Using this approach, we successfully performed surgery in this technically demanding case without any complications. This may largely be due to improvement of the navigation system and intraoperative image quality, but careful observation and evaluation of preoperative imaging details were also important.
Conclusion
We experienced a rare case of Morquio syndrome, in which cervical cord disorder developed in late middle age. Diminutive and soft osseous structures make instrumentation surgery technically challenging in a patient with Morquio syndrome. However, modern technology for spine surgery and development of spinal instruments with the use of an intraoperative navigation system allowed us to perform a complicated surgery safely and to obtain a favorable clinical outcome.
Footnotes
Consent
The patient gave informed consent to submit this manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.