
Abstract
Background:
It is important to understand postoperative global sagittal spinal alignment after total hip arthroplasty (THA) to prevent not only the following hip complications but also progressing lumbar degeneration. The purpose of this study was to progress the analysis of the global sagittal spinal alignment between before and after THA in patients without large lower limbs discrepancy.
Subjects and methods:
The subjects were 87 patients with bilateral hip osteoarthritis (OA) before unilateral primary THA. We measured sagittal vertical axis (SVA), lumbar lordotic angle, sacral slope, pelvic tilt (PT), and pelvic incidence (PI) and compared the postoperative change of those parameters. Excluded criteria were Crowe classification types II, III, and IV and more than 10 mm of leg length difference, spinal scoliosis (Cobb angle > 25°), and lumbar kyphosis.
Results:
The correlation coefficient between preoperative factors and postoperative sagittal alignments revealed that postoperative SVA has correlation with age (r = 0.46, p < 0.008) and preoperative PT (r = 0.42, p = 0.015). Postoperative PT had a correlation with preoperative PI (r = 0.46, p = 0.007). The change of PT after operation had negative correlation to preoperative PT (r = −0.47, p < 0.01) and PI (r = −0.38, p = 0.03). Multiple regression analysis revealed that the change of PT = 4.979 − 0.235 × preoperative PT (p < 0.05). Therefore, when preoperative PT was less than 20°, the postoperative PT would become larger than the preoperative one.
Conclusion:
(1) In patient with hip OA without large lower limbs discrepancy, the postoperative PT after THA correlated with PI. (2) The postoperative change of PT was influenced by preoperative PT.
Keywords
Introduction
In aging society, the number of patients with hip osteoarthritis (OA) is increasing. Hip OA is a degenerative joint disease and one of the most common causes of disability in the elderly. The morbidity of hip OA in Japan was reported as 1.0–4.3%, 1,2 and secondary OA occurs in approximately 90% of the total patients as a response to primary disease such as acetabular dysplasia. 3 The pathogenesis of hip OA is genetic factors, involving age-related, environmental, and biomechanical factors as well as bone morphology. It has been recognized that one of the important mechanisms for the onset of hip OA is global spinal alignment which can be associated with the reciprocal influence between the spine and hip joint as adjacent organs. 4 Total hip arthroplasty (THA) is an established and excellent treatment for patients with OA of the hip. However, the relationship of global spinal alignment between before and after THA has been less discussed. 5 –9 The prediction of the global sagittal spinal alignment after THA is important to set the optimal acetabular cup. Optimal positioning of the acetabular cup is essential for preventing postoperative complications such as polyethylene wear, implant failure, and dislocations. Previous reports analyzed the relationship between pelvic tilt (PT) and cup angles; however, there was no mention about the influence of lower limbs discrepancy, and the characteristic of change in global sagittal spinal alignment is still unclear. The purpose of this study was to progress the analysis of the global sagittal spinal alignment between before and after THA in hip OA without large lower limbs discrepancy.
Materials and methods
The subjects were 87 cases (men 13 cases, women 74 cases; average 69.7 ± 11.2 years old; Table 1) of 120 cases with bilateral hip OA (Kellgren and Lawrence grades 3–4 10 ) before unilateral primary THA excluding the following criteria to focus on the relation between THA and the change of sagittal pelvic alignment: high degree of luxation, 10 mm or greater difference in leg length, Crowe classification types II, III, and IV, severe hip joint flexion contracture (above 20°), spinal scoliosis (Cobb angle > 25°), and lumbar kyphosis. Radiographs were taken in full spine lateral view standing position at the just before and 3 months after the operation. All the subjects underwent frontal and lateral radiography of the entire lumbosacral spine and the hip joints in standing positions. Whole spine anteroposterior and lateral radiographs were obtained using the digital slot-scanning radiography of a Sonialvision-safire fluoroscopy system (Shimadzu Corporation, Kyoto, Japan), with the entrance surface dose of 0.07 and 0.21 mGy, respectively. On marked X-ray images, the following radiographic parameters were measured by computer analysis as described previously: 11 (1) sagittal vertical axis (SVA) is defined as the horizontal distance between the C7 plumb line and the posterior superior corner of the superior margin of S1; (2) lumbar lordotic angle is the angle from the upper endplate of L1 to the upper end plate of S1; (3) sacral slope (SS) is the angle between the superior endplate of S1 and a horizontal axis; (4) PT is the angle between the line connecting the midpoint of the sacral plate to the axis of the femoral heads and the vertical axis; and (5) pelvic incidence (PI) is the angle between the perpendicular to the sacral plate at its midpoint and the line connecting the point to the middle axis of the femoral heads (Figure 1). The radiographs were measured twice by the first observer (a board-certified orthopedic spinal surgeon), then independently measured on different days by a second observer (a board-certified orthopedic spinal surgeon). Descriptions of the reliability of this method, including the intra- and interobserver agreements, were described in detail in a previous article. 11

Radiographic parameters of the sagittal hip–spine alignment. SVA: sagittal vertical axis; LL: lumbar lordotic angle; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
Patient anthropomorphic characteristics.

BMI: body mass index; OA: osteoarthritis.
Before performing this study, we obtained approval from the Hospital Ethical Review Board and written informed consent from all subjects. For statistical analysis, JMP software version 23 (SPSS, Chicago, Illinois, USA) was used. For analyzing statistical differences between the two groups, the t-test or Mann–Whitney test (risk rate 5%) was adopted, and the Spearman rank correlation coefficient was used to examine correlations among alignment parameters. To identify the preoperative crucial risk factors for postoperative PT change, risk factor analysis was performed by multivariate logistic regression with a forward stepwise procedure (p < 0.05 for entry). The occurrence of postoperative PT change was used as a dependent variable, with age, preoperative SVA, PT, and PI as independent variables.
Results
There was no significant change of those global sagittal spinal alignment between before and after THA (Table 2). However, the correlation coefficient between preoperative factors and postoperative sagittal alignments revealed that postoperative SVA has correlation with age (r = 0.46, p < 0.008) and preoperative PT (r = 0.42, p = 0.015). Postoperative PT had a correlation with preoperative PI (r = 0.46, p = 0.007) (Table 3). The change of PT after operation had negative correlation to preoperative PT (r = −0.47, p = 0.007) and PI (r = −0.38, p = 0.03) (Table 4). Multiple regression analysis revealed that the change of PT = 4.979 − 0.235 × preoperative PT (p < 0.05).
Sagittal balance analysis (preoperative and postoperative).

SVA: sagittal vertical axis; LL: lumbar lordotic angle; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
Correlation between preoperative and postoperative sagittal alignment.

Post: postoperation; SVA: sagittal vertical axis; LL: lumbar lordotic angle; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
a p < 0.05.
Correlation between preoperative and the change of postoperative sagittal alignment.
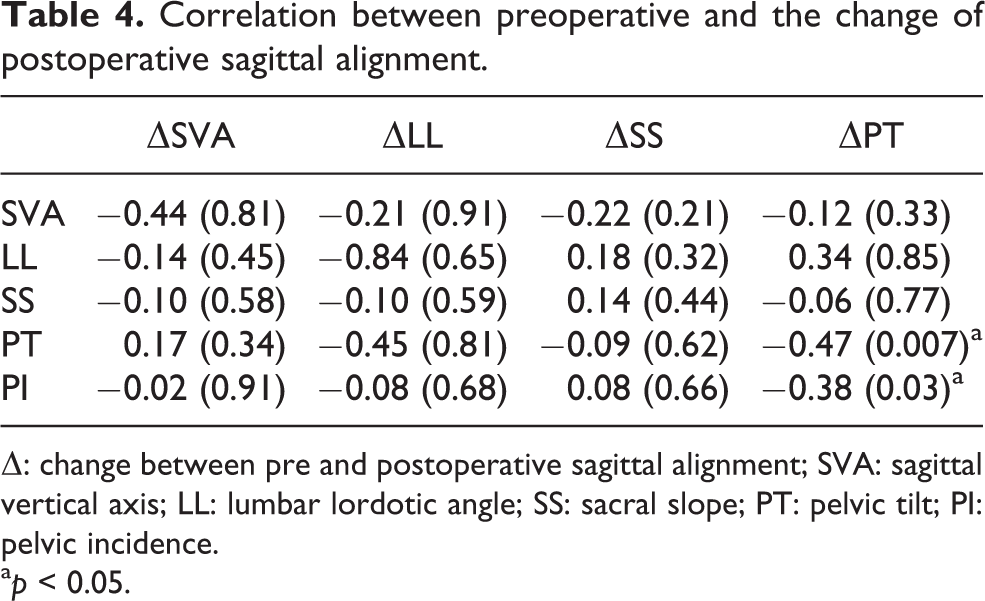
Δ: change between pre and postoperative sagittal alignment; SVA: sagittal vertical axis; LL: lumbar lordotic angle; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
a p < 0.05.
Discussion
As to lower limbs discrepancy, it was reported that rotation of the pelvis in the coronal plane during the acquisition of radiographs influences PI, PT, and SS measurements. The difference of lower limbs up to 50 mm appeared to have a negligible influence on PI, PT, and SS measurements. 12 Therefore, present study excluded severe cases with a difference in leg length of 10 mm or greater. Previous studies reported the close relationship between the preoperative sagittal spinal alignment and the postoperative change of THA. It was reported that no significant changes have been noted in radiographic spinal sagittal alignment postoperatively. 13
SVA has positive correlation with age and PT in asymptomatic volunteers 12 and our data showed the same results as the postoperative SVA has correlation with age (r = 0.46, p < 0.008) and preoperative PT (r = 0.42, p < 0.01). Therefore, SVA was less affected by THA. Legaye et al. mentioned that pelvic morphologic angle (PI) is a morphological constant taken as an independent measure of the pelvic spatial orientation and affects sagittal spinal alignment. 13 Thus, the concepts of hip–spine syndrome should be reinterpreted by considering the pelvic morphologic angle. The present study focused on analyzing the influence of PI and resulted that postoperative PT correlated with PI (r = 0.45, p = 0.009). Postoperative large PT is likely to be affected by large PI.
Regarding the postoperative change of PT, Okuda et al. showed that the preoperative anterior PT generally exhibited posterior changes in PT after THA, 5 while patients with preoperative posterior PT did not experience significant postoperative changes in PT. 8 Our results showed similar results in patients with secondary hip OA without large lower limbs discrepancy. Multiple regression analysis revealed that the change of PT = 4.979 − 0.235 × preoperative PT, which means that when preoperative PT was less than 20°, the postoperative PT would become larger than the preoperative one. The small preoperative PT cases and large PI cases tend to have large PT after the operation. In this context, care should be taken in excessive anteversion of acetabular cup and femoral stem due to potential anterior dislocation after THA.
This study had some limitations. First, the analysis of sagittal pelvic rotation by using PT is difficult after THA for the change in the height of hip center. The method of PT measurement is controversial in patients of lower limb discrepancy, and we had to decide the strict exclusion of THA case. After the exclusion, the number of subjects was relatively small, and we could not declare the constant tendency after THA. Second, the effects on hip and knee could not be analyzed. Third, the evaluation of long-term results could not be analyzed. Despite these limitations, our results could contribute to understanding the postoperative PT without large lower limbs discrepancy. In future studies, the effects of the lower limbs’ discrepancy to the sagittal spinal alignment and long-term follow-up results are to be addressed.
Conclusion
In patient with hip OA without large lower limbs discrepancy, the postoperative PT after THA correlated with PI.
The postoperative change of PT was influenced by preoperative PT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.