
Abstract
Purpose:
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) patients significantly increase muscle strength after maximal strength training (MST) initiated soon after surgery. Owing to severe postoperative pain, knee patients are anticipated to be more limited in performing heavy load exercises than hip patients. The aim of the present study was to describe pain and load progression during early MST in THA and TKA patients.
Methods:
Explorative study based on secondary analyses from two randomized controlled trials: 26 THA and 16 TKA patients had their training sessions logged. They trained at 85–90% of their maximal capacity in leg press, and abduction/knee-extension of the operated leg (4 × 5 repetitions) for 8–10 weeks, initiated early postoperatively.
Results:
Knee patients experienced significantly more pain than hip patients during the training sessions (p < 0.03), however, pain before and after training was not different (p > 0.09). All patients significantly increased leg press training load until the last intervention week (p < 0.01).
Conclusion:
This study demonstrates that TKA patients experience more pain than THA patients during training following a MST program but not more than moderate levels during or after training. Pain before and after training is not different. Both groups significantly increased load progression during the intervention. These findings indicate that both THA and TKA patients might perform MST with extensive load progression early after surgery without compromising pain. The studies were registered at ClinicalTrials.gov.
Introduction
Muscle strength is substantially reduced before total hip arthroplasty (THA) and total knee arthroplasty (TKA) because of pain, reduced range of motion, and immobility and might last up to years after surgery. 1 –3 Regaining muscle strength early following surgery is imperative to obtain a normal gait pattern and to increase mobility during daily living activities. 4 After surgery, sore and painful muscles can result in disuse and immobilization. However, when patients are receiving multimodal opioid-sparing analgesia, pain has been found to have a limited influence on early functional recovery. 4,5
The significant impairment in muscle strength postoperatively is related to neural motor function and central neural drive, and a diminished ability to restore muscle strength during recovery might further reduce the neural drive and lead to a vicious circle of reduced muscle strength. 6,7 Adaptations in mechanical muscle function and improvements in muscle strength in the early phase of recovery are attributed foremost to neural adaptations and central neural drive. 8 A high load is required during training to achieve sufficient levels of neuromuscular activation to stimulate muscle growth and strength. 9,10 It has been demonstrated that maximal strength training (MST) with an emphasis on neural adaptations improves work economy, rate of force development, and maximal strength more than conventional strength training. 11 MST initiated soon after THA and TKA is feasible and safe to perform and has demonstrated considerable increases in leg muscle strength compared to conventional physiotherapy. 12 –14
TKA patients report higher levels of postoperative pain during hospitalization compared to THA patients. 15,16 TKA patients experience moderate–to-severe pain, in contrast to THA patients who only experience mild pain up to 1 month postoperatively. 17,18 Pain and stiffness have been found to reduce earlier in THA compared to TKA patients 19 and persistent pain (>3 months) is more common after TKA compared to THA. 20 Heavy strength training has not been found to exacerbate postoperative pain in THA or TKA patients 21,22 ; however, increased postoperative pain during strength training implemented shortly after TKA has been reported. 23 Concerns have been related to fear of pain following high intensity strength training and the feasibility to perform MST early after surgery, especially in TKA patients. In the current literature, there is a lack of information concerning pain responses related to strength training intensity and load progression during rehabilitation after hip and knee joint replacement surgery. The purpose of the present study is, therefore, to describe pain responses before, during, and after performing MST, and the muscle strength progression throughout the intervention period of 8–10 weeks in TKA and THA patients, initiated soon after surgery.
Materials and methods
Design
The present study is an exploratory study presenting secondary analysis from two previously published randomized controlled trials (RCTs). 13,14 The present study describes pain and training progression in TKA and THA patients, performing MST for 8 and 10 weeks after surgery, respectively.
Ethics and consent
The RCTs were approved by the regional ethics committee, conducted in accordance with the Declaration of Helsinki and registered at ClinicalTrials.gov. All patients gave informed consent for study participation and were treated according to the standardized fast-track course for hip and knee arthroplasty patients at the hospital. The patients were instructed to use analgesics as recommended from the hospital when discharged. Details of the fast-track clinical pathway have been described previously. 24
Patients
Patients with primary hip or knee osteoarthritis, undergoing elective THA or TKA surgery, were included in the RCTs. All THA patients were operated on by the posterior approach and all TKA patients were operated on by the medial parapatellar approach with no replacement of the patella. Of these patients, those who completed the training intervention and for whom the training sessions were logged were included in the present study. Exclusion criteria for the THA patients were severe osteoarthritis of the contralateral limb, not being fully recovered from a previous THA surgery, having been discharged to a rehabilitation institute, or any illness or disorder that could influence the training and/or physical testing. TKA patients were excluded if they were aged over 75 years, had undergone a previous TKA surgery in the contralateral knee or had a travel distance of more than 30 min from the hospital. Both the THA and TKA patients were to be excluded if there were any communication difficulties; however, none were experienced. The patients’ characteristics are presented in Table 1.
Characteristics for the THA and TKA patients.a

THA: total hip arthroplasty; TKA: total knee arthroplasty; BMI: body mass index; SD: standard deviation: female; M: male.
a Data are presented as mean and range or mean and SD.
Intervention
All training sessions consisted of a one-to-one follow-up with a physiotherapist/exercise physiologist supervising the patients performing MST in leg press and abduction/knee-extension strength exercises, using the operated leg only. Three training sessions a week were scheduled for 8 to 10 weeks for the TKA and THA patients, respectively. The THA patients trained at a municipal physiotherapy institute, whereas the TKA patients visited the orthopedic research unit at the hospital as outpatients.
Training protocol
Prior to the training intervention, one repetition maximum (1RM, the maximum amount of weight a person can lift for one repetition) was determined for each patient to decide the initial weight load during the first training session. Leg press was tested in an ergometer device (Steens Physical, Ring Mekanikk AS, Norway). Abduction strength was tested in a pulling apparatus (Pivot 820, Sports Master, Norway) and knee extension was tested using a knee extension equipment (Body-Solid, Forest Park, Illinois, USA). The 1RM was determined by gradually increasing the weight until the patient was unable to perform the movement. The TKA patients trained in the same devices in which they were tested and the training intensity during the first session were calculated based on the 1RM test. The THA patients trained in devices similar to the testing apparatus and the training intensity were based on the 1RM test, and individually adjusted in the first training session to reach the goal of 5RM (the maximum amount of weight a person can lift for five repetitions). The protocol was identical for both the THA and TKA patients. Each training session started with a 10-min warm-up period consisting of walking or ergometer cycling. After the warm-up, patients performed four series of five repetitions, with a load of 85–90% of 1RM and a focus on high velocity in the concentric phase. Despite an intended high velocity in the concentric part of the movement, to stimulate the neural drive, the actual movement was relatively slow because of the heavy load. The series were separated by 1- to 2-min resting periods, and the load was increased when the patient could perform more than 5RM. First, both the THA and TKA patients performed leg-press seated in an ergometer device and were instructed to perform the leg-press movement starting from an extended position to flexion with a knee joint angle of 90°. Thereafter, the THA patients performed abduction in a pulling apparatus with the patient standing on the nonoperated leg, with a sling attached to the testing leg and instructed to perform the abduction with the toes pointing forward. After the leg-press exercise, the TKA patients performed knee-extension seated in an ergometer device and instructed to extend the leg from a knee joint angle of 90°.
Training log
Training load, sensation of pain, and analgesic consumption were registered and logged for each training session. The training load was recorded for all series in a training session and measured in kilograms (kg). The mean load for the four series in a completed training session was used in the analysis. Pain intensity was recorded immediately before, during, and after training and was assessed by the numeric rating scale (NRS) ranging from 0 to 10, in which 0 is considered “no pain” and 10 “the worst pain imagined.” The type of analgesic and the amount consumed within 2–3 h prior to training was recorded.
Statistical analyses
A general linear mixed model was used for data modeling, defining training session as repeated measurements. The preoperative value for the tested variable was included as a covariate in the analysis, representing a baseline control as well as correcting for the eventual initial imbalance between the groups. The statistical model used time (postoperative weeks) and joint (hip/knee) as fixed factors and included a random subject intercept. An interaction term with the joint and time was included as a factor to obtaining model plots of hip and knee scores at several time points. Sequential Bonferroni correction was used to adjust for multiple comparisons. Histograms were used to verify the normality of the model residuals. All figures represent model estimates, adjusted for covariates. The statistical analyses were performed using the software package IBM SPSS Statistics for Windows, version 25, IBM Corp. (Armonk, New York, USA).
Results
Compliance
Thirty THA and 19 TKA patients were included in the intervention groups in the two RCTs. Two patients, one in each group, were lost to follow-up during the intervention period as they left the study due to personal reasons. One THA patient was lost to follow-up owing to pain not related to training and one owing to knee problems. One TKA patient was lost to follow-up owing to a deep infection and one owing to mobilization of a stiff knee. One of the THA patients who completed the training intervention, however, did not log the trainings and were excluded. Therefore, of the 27 THA and 16 TKA patients completing the training intervention, 26 and 16 had their training logged, respectively, and are included in the present study. Demographic variables for the patients are presented in Table 1. Training started at mean (SD) day 15 (4) for the THA, and 8 (0) for the TKA patients postoperatively. The average number of training sessions completed for the THA and TKA patients was a mean (SD) of 24 (4) and 23 (3), respectively.
Pain
Overall, TKA patients experienced statistically significantly more pain than the THA patients during the training sessions (p < 0.03). No statistically significant differences in pain were found between the THA and TKA patients before (p > 0.08) or after training (p > 0.09). The pain scores are shown in Figure 1.

Pain scores (NRS) for the total hip arthroplasty patients (blue) and total knee arthroplasty patients (red) from postoperative weeks 1–11. The panels present the pain (a) before, (b) during, and (c) after training. NRS: numeric rating scale.
Load progression
Both THA and TKA patients statistically significantly increased training load in leg press until the last intervention week (p < 0.01). THA patients statistically significantly increased abduction training load until the second last intervention week (p < 0.01), whereas knee extension training load statistically significantly increased until the last intervention week in the TKA patients (p < 0.04). The load progression for leg press and abduction/knee extension is shown in Figures 2 and 3, respectively.
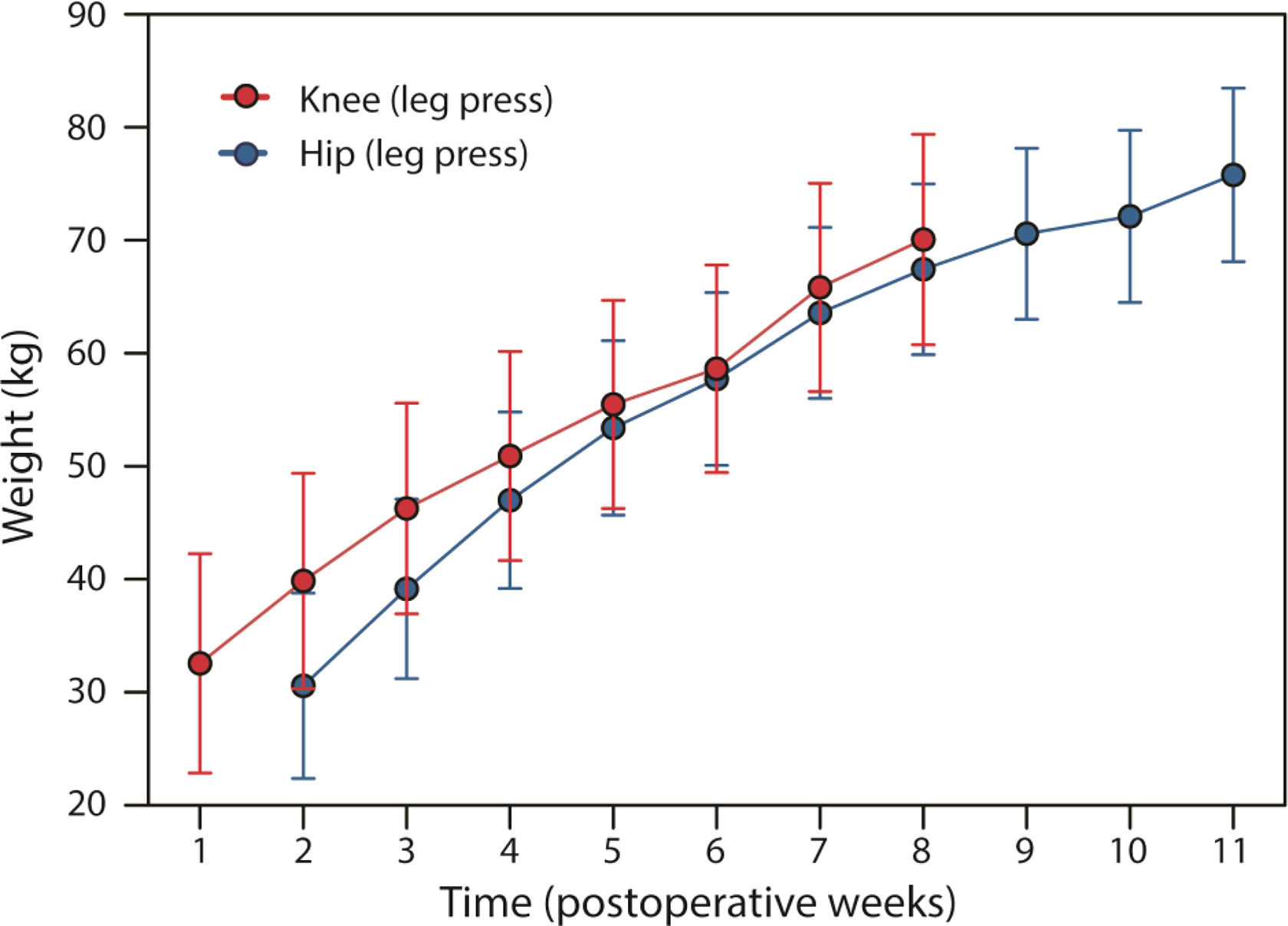
Training load while performing five repetitions of four series of leg press in the total hip arthroplasty patients (blue) and total knee arthroplasty patients (red) from postoperative weeks 1–11.

Training load while performing five repetitions of four series of abduction for the total hip arthroplasty patients (blue) and knee extension for the total knee arthroplasty patients (red) from postoperative weeks 1–11.
Discussion
TKA patients experience more pain than THA patients during training. However, pain before and after training does not differ between the groups. MST initiated soon after THA and TKA surgery significantly increases the strength and load progression during the intervention period.
It has been found that decreased muscle activation, rather than atrophy or pain, is a key factor for reduced muscle strength in TKA patients postoperatively, 25 owing to the failure of the central nervous system to activate the quadriceps muscle, 26,27 as a result of swelling, inflammation, and damage to joint afferents. 28 Therefore, rehabilitation should be initiated as soon as possible after surgery with a focus on intensive strength training and neuromuscular stimulation to increase the nervous activation and force output of the quadriceps muscle. 23,25,29 For practical reasons, TKA patients started training at day 8 and THA patients at day 15 postoperatively. The TKA patients were treated as outpatients in the hospital’s orthopedic research unit, while the THA patients were treated in outpatient physiotherapy clinics at municipal institutes, in accordance with the current clinical practice. Despite the different intervention settings, both groups produced significant increases in the training load and muscle strength, and as previously demonstrated, these were significantly greater than the respective control groups who performed conventional low-intensity strength training. 13,14 The training prescription for both studies was identical with regard to the intensity and frequency; five repetitions for four series at an intensity of 85–90% of 1RM three times per week. An important factor to consider when targeting neural adaptations is that all motor units, especially those at the high thresholds, should be stressed, to achieve maximal muscle activation. 30 MST induces neural adaptations by emphasizing heavy loads, few repetitions, and maximal mobilization of force through high intended maximal velocity in the concentric part of the movement. TKA patients were scheduled for 2 months and the THA patients for 3 months, in accordance with the standard clinical follow-up at the hospital. As the THA patients followed the standard clinical practice, the frequency and duration were not specified for these patients, in contrast to the TKA patients who were supervised in the hospital research unit. This resulted in a similar total number of training sessions performed by the two groups, that is, 24 and 23, respectively.
Pain during training was significantly higher in the TKA patients compared to the THA patients; however, training was feasible, and the load progression increased during the whole training period. The total increase in the leg press training load was about 120% and 130% kg for the TKA and THA patients during the first 8 weeks of their respective intervention periods (Figure 2). This demonstrates an almost equally high load progression among the TKA patients, despite a higher pain sensation compared to the THA patients. These findings are in accordance with those reported by Dailiana et al., 19 who reported less pain and stiffness in THA patients compared to TKA patients soon after surgery. Despite the increased training intensity and the concomitant post-training pain response, pain was not increased above moderate values. An NRS score ranging from 1 to 3 is considered mild- and up to 6 as a moderate pain level. 31 A change of 1.5 on the NRS has previously been defined as being clinically relevant. 23 Even though pain was statistically significantly higher in TKA patients compared to THA patients during training, the pain was only moderate for the first month and thereafter reduced to mild pain. A clinically relevant higher pain level for the TKA patients of about 1.5 points on the NRS was only present in the first five postoperative weeks. It is reasonable to anticipate that MST with few repetitions may not aggravate pain, as our findings are in accordance with others, demonstrating that heavy strength training does not exacerbate postoperative pain in THA or TKA patients. 21,22 Even though both heavy load strength training and strength training with more repetitions performed to contraction failure early in the postoperative period have been found to increase knee pain, only the latter has been demonstrated to exceed what is defined as clinically relevant. 23
All patients in the present study were treated in accordance with the fast-track patient course in our hospital. 24 A focus in the fast-track clinical setting is to empower the patients through information, including the importance of taking an active part in the rehabilitation process. Findings from a qualitative study 32 report that the TKA patients were able to cope with pain in the postoperative phase, as a pain sensation was expected and they had learned that training was necessary and important. All patients in the present study were informed in beforehand that MST testing and training is feasible and safe to perform and were closely supervised and motivated during each training session. In accordance with the study by Bandholm et al., 23 pain increased during training but diminished shortly after training. The THA patients experienced only mild pain during training throughout the training period, while the TKA patients did not reach a mild pain level until the fifth postoperative week. TKA patients had more pain than the THA patients during training; however, pain before and after training was not different. These results are partly in line with the findings from others that have demonstrated that TKA patients experience more pain in the first postoperative month and that THA only induces mild pain. 9,17 The clinical impact from the present study is that pain does increase in relation to high-intensity strength training, but most importantly, not more than moderate levels during or after MST training. Even though TKA patients experience more pain than the THA patients during MST training, only moderate pain levels are demonstrated. MST is well tolerated by TKA patients and does not provide more pain than THA patients before or after MST training initiated soon after surgery. These findings give valuable information to future patients, physiotherapists, and physicians and could improve current practice by encouraging patients to start high-intensity strength training as soon as possible after hospital discharge, demonstrating that it is feasible to perform MST without the fear of perceiving high pain levels both in THA and TKA patients.
There are some limitations to be considered in the present study. First, it is an explorative study with a relatively small number of participants and the results should be interpreted concluding that “there are signs that.” Second, analgesic consumption reporting was incomplete for the THA patients and is therefore not included in the analysis. However, all patients were recommended to follow the standardized regimen prescribed by the hospital, 24 giving the patients optimal pain relief. Third, the THA patients started training 1 week later than the TKA patients and the two studies were conducted in different settings. As the groups were treated in different centers, it might be speculated that this would confound the results, however, all training followed the exact same defined methodological design, which minimized this confounding factor. All patients had a close one-to-one follow-up with either an exercise physiologist or a physiotherapist at all training sessions. This supervision ensured that the training protocol was completed and that the reporting was correct. Despite a different number of intervention weeks, the total number of training sessions was about the same for the TKA and THA patients, 23 and 24 sessions, respectively. Further studies should focus on initiating intensive strength training as soon as possible after surgery for both THA and TKA patients to diminish the vicious cycle of reduced muscle strength experienced in these patients postoperatively. Both hip- and knee arthroplasty patients should be encouraged to initiate heavy load strength training as soon as possible after surgery.
Conclusion
This study demonstrates that TKA patients experience more pain than THA patients during training following an MST program initiated early after surgery but not more than moderate levels during or after training. Pain before and after training is not different. Both groups significantly increase load progression during the intervention period. These findings indicate that both TKA and THA patients might perform MST with extensive load progression early after surgery without compromising pain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.