
Abstract
Purpose:
Several radiographic parameters describe humeral head coverage by the acromion. We describe a new radiographic measurement, the acromion–greater tuberosity impingement index (ATI), and its ability to predict rotator cuff pathology.
Methods:
The ATI was measured with magnetic resonance imaging (MRI) and X-ray analysis in 83 patients with rotator cuff pathology and 76 patients with acute rotator cuff tears. The lateral acromial angle (LAA), acromion type, the acromion index (AI) and the critical shoulder angle (CSA) were measured to assess their correlations with the ATI. Receiver operating characteristic (ROC) curves were used to predict degenerative rotator cuff pathology. The change in the ATI after acromion surgery was evaluated in both groups.
Results:
According to the ROC curves, the ATI is a good predictor of degenerative rotator cuff pathology on both X-ray (cut-off, 0.865) and MRI (cut-off, 0.965). Patients with degenerative rotator cuff pathology had a significantly higher average ATI compared to the trauma group (p = 0.001 for X-ray and MRI). The degenerative group had a significantly lower LAA (p = 0.001) and a higher ratio of type III acromion (p = 0.035) than the trauma group. The ATI on X-ray was negatively related to the LAA and positively related to the AI, the CSA and acromion type (each p < 0.05). The ATI on MRI was negatively related to the LAA and positively related to the AI and acromion type (each p <0.05). More patients in the degenerative group than the trauma group needed acromioplasty or acromion decompression (p < 0.05). The ATI on MRI was significantly lower after acromion surgery compared to before surgery in both groups (p < 0.05).
Conclusion:
The ATI is a good predictor of degenerative supraspinatus tendon tears or subacromial impingement syndrome. The ATI on MRI is more accurate and can precisely guide acromion surgery.
Background
Acromial morphology is associated with shoulder pathologies and is an important theoretical cause of subacromial impingement, in which the rotator cuff tendons are chronically damaged. Impingement mostly occurs under the anterior and lateral portions of the acromion. 1 Studies have attached importance to the morphological appearance of the acromion on radiographs. In the sagittal plane, acromion type has been proposed as a risk factor for rotator cuff tears (RCTs). 2 In the coronal plane, the acromion index (AI), critical shoulder angle (CSA) and lateral acromial angle (LAA) have also been reported. 3 –5 Many studies have suggested that the morphological characteristics of the acromion are associated with RCTs, 6 –8 although not all studies support this view. 9,10
Previous acromial morphology parameters are isolated and not connected to the greater tuberosity of humerus, so they only predict RCT or subacromial impingement syndrome (SAIS) risk 4 but do not reflect the kinematics of the glenohumeral joint or the severity of the subacromial impingement. Moreover, these parameters have low sensitivity for predicting RCTs. 6 Although SAIS is usually caused by acromial morphology, little attention has been paid to glenohumeral motion or humeral greater tuberosity morphology. 11,12 A recent study found that the presence of a subacromial spur was related to the size of the greater tubercle of the humerus and to the humeral head ratio. 11 The morphology of the anterior and lateral acromion can be modified surgically when performing acromioplasty and subacromial decompression. 1 However, postoperative changes in the lateral acromion are not accurately reflected by the common coronal imaging parameters (AI, CSA and LAA).
We propose a new measurement, the acromion–greater tuberosity impingement index (ATI), which is calculated by dividing the distance from the rotation centre of the humeral head to the greater tuberosity of the humerus by the distance from the rotation centre of the humeral head to the undersurface of the acromion. We examined whether the ATI on X-ray and magnetic resonance imaging (MRI) predicts degenerative rotator cuff pathology, compared relationships between the ATI and other parameters to determine whether the ATI is more accurate and reliable, compared differences in the ATI between patients with degenerative and acute RCT and evaluated the role of the ATI in precisely guiding acromion surgery.
Methods
In our department, 392 patients with RCTs underwent arthroscopic surgery from June 2017 to January 2019. After reviewing patient data and surgical protocols, we excluded patients with a history of shoulder surgery, fracture, tumour, infection, glenohumeral osteoarthritis, frozen shoulder, irreparable RCTs and nonstandardized radiographs. This left 159 patients (77 females, 82 males; average age 63.8 years), including 76 with traumatic RCTs (trauma group) and 83 with degenerative RCTs or SAIS without trauma (degenerative group) (See Table 1).
Demographics of the patients for the traumatic and degenerative groups.a

RCT: rotator cufftear.
a Those results that reached statistical significance are in boldface to highlight these.
The trauma group were those who reported pain and loss of function within 3 months of trauma, such as a fall or stretch injury of the shoulder. The degenerative group were those who reported pain and loss of function without trauma. Patients presented with shoulder pain, a painful arc of abductive movement from 60° to 120°, and positive Neer and Hawkins tests. Both anteroposterior (AP) and outlet view radiographs and MRI were obtained before and after surgery. All patients in the degenerative group underwent conservative therapy for a minimum of 5 months.
The ATI was measured on both AP plain radiographs and coronal plane MRI (Figure 1). Using a ratio rather than absolute values allowed us to avoid magnification errors on radiographic images and to compare individuals of different sizes. The coronal MRI plane included the supraspinatus insertion and greater tuberosity of the humerus. The LAA, AI and CSA were measured on preoperative AP radiographs. Acromion type was evaluated on outlet view X-ray (Figure 2). The true radiograph was taken with the arm in a neutral position, the elbow extended and the thumb aimed anteriorly when the beam was aligned 20° caudally and 20° of internal rotation. According to the Suter/Henninger classification scheme, 13 the relative standardized radiographs (types A, B and C) were included and nonstandardized radiographs (types D) were excluded in the current study. MRI was performed with a 3.0-T closed-type scanner (Toshiba, Otawara, Japan). MRI scans were taken with the patient in the supine position with the arm in a neutral position, keeping the arm in 0° of abduction and the thumb aimed anteriorly.

A circle is superimposed which followed the contour of the articular surface of the humeral head, mainly recognizing the medial and upper cartilaginous surfaces in order to find its centre. ATI is calculated by dividing the distance from the rotation centre of the humerus head to the greater tuberosity of the humerus by the distance from the rotation centre of the humerus head to the undersurface of the acromion. The ATI measurements were performed both on a true AP X-ray (a) and coronal plane of MRI (b). ATI: acromion–greater tuberosity impingement index; AP: anteroposterior; MRI: magnetic resonance imaging.

(a) AI, (b) LAA, (c) CSA and (d) acromion type. AI: acromion index; LAA: lateral acromial angle; CSA: critical shoulder angle.
We measured the distances from the acromion to the glenoid (AG) and between the lateral part of the greater tuberosity of the humerus and the glenoid (HG). The AI was calculated as the ratio of AG and HG (Figure 2(a)). The LAA was the angle formed by a line parallel to the lateral surface of the glenoid and a line along the undersurface of the acromion (Figure 2(b)). The CSA was formed by line 1, which connects the superior and inferolateral points of the glenoid, and line 2, which connects the superior-most and inferolateral points of the acromion (Figure 2(c)). Acromial morphology was classified into types I to III (Figure 2(d)). 5
General anaesthesia and brachial plexus block were used for analgesia. Arthroscopy was performed through a standard posterior arthroscopic portal. Anterior and lateral acromioplasty was performed after clearing the subacromial bursa and releasing the coracoacromial ligament in the subacromial space, where approximately 5 mm of the anterior and lateral borders of the acromion were resected (Figure 3). A double row repair or the double-pulley suture-bridge technique was used to repair RCTs.
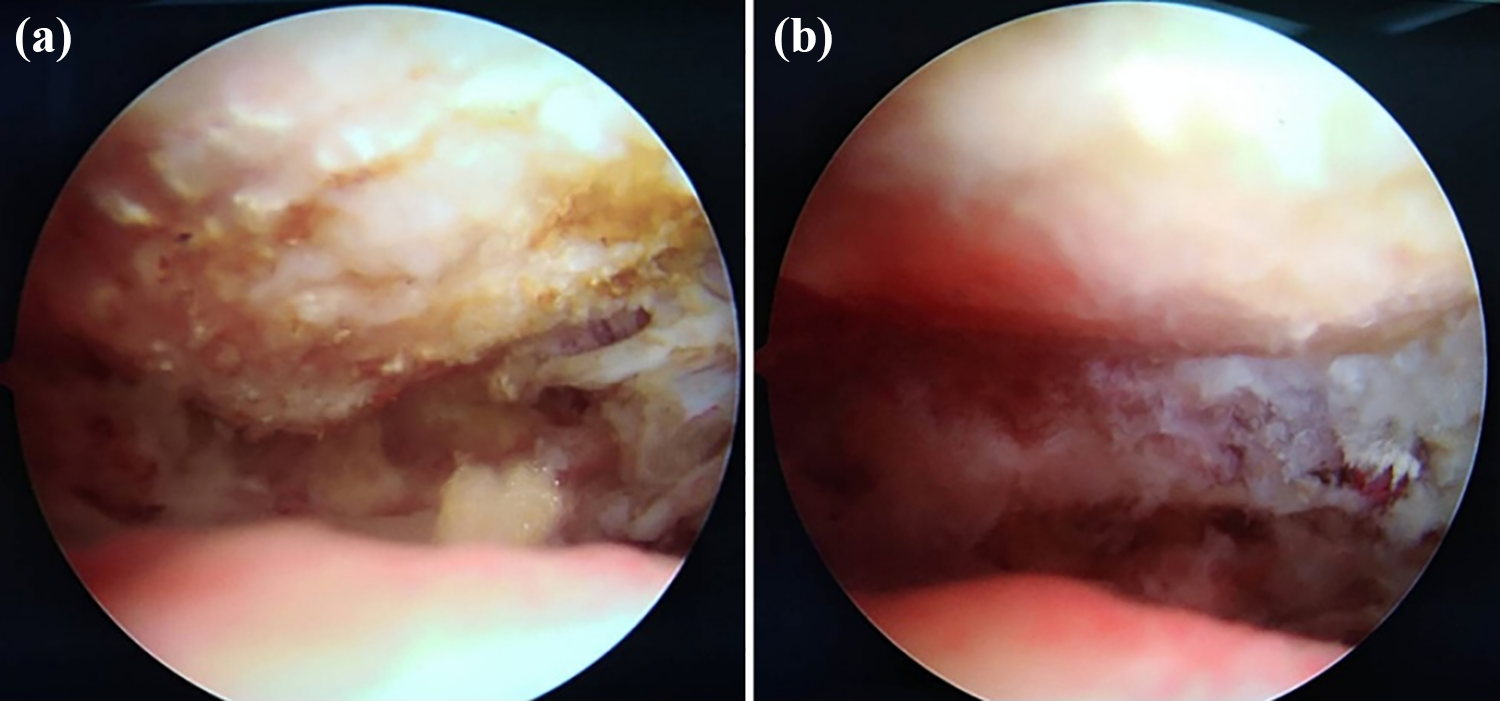
(a) Subacromial space after acromion decompression during the shoulder arthroscopy and (b) subacromial space after acromioplasty during the shoulder arthroscopy.
All statistical analysis, including mean values and standard deviations, were performed with the use of SPSS, version 17.0 (SPSS Inc., Chicago, Illinois, USA). The χ 2 tests were used for discrete variables, such as sex, shoulder side, acromion type, surgical type and size of the RCT. The reproducibility of the ATI measurements was assessed with intraclass correlation coefficients for interrater reliability (two observers) and intrarater reliability (two measurements at different time points by one observer). Independent t-tests were used to evaluate differences in parameters (e.g. age, ATI, AI, LAA and CSA) between the degenerative and trauma groups. Pearson’s correlation coefficients were used to calculate correlations between the ATI, AI, LAA and CSA. Spearman correlation coefficients were used to calculate correlations between the acromion type and the ATI, AI, LAA and CSA. Receiver operating characteristic (ROC) curve analyses were used to determine the cut-off values for significant parameters. The values of p < 0.05 were considered statistically significant.
Results
In terms of demographic variables, sex, dominant side and size of the RCTwere matched between the trauma and the degenerative groups (p > 0.05; Table 1). However, age was not matched, because degenerative shoulder disease usually affects the elderly (p < 0.05). The intrarater (0.975, 0.952) and interrater (0.931, 0.923) reliability of the ATI measurements was excellent for the ATI from X-ray and MRI, respectively. In terms of concentric motion of the glenohumeral joints, the ATI was a good parameter for predicting degenerative supraspinatus tendon tears or SAIS on both X-ray and MRI. When comparing the ATI between the trauma and the degenerative groups, we found that patients in the degenerative group had a significantly higher average ATI on X-ray (0.89 vs. 0.85, p = 0.001) and MRI (0.99 vs. 0.96, p = 0.001) than the trauma group (Table 2).
Comparison of each parameter between traumatic and degenerative groups.a

ATI: acromion–greater tuberosity impingement index; AI: arcromial index; LAA: lateral acromial angle; CSA: critical shoulder angle; MRI: magnetic resonance imaging.
a Those results that reached statistical significance are in boldface to highlight these.
Types I and II acromions were common in trauma and degenerative cases (98.7% vs. 90.4%), whereas type III was rare in trauma cases (1.3% vs. 9.6%). We compared the other radiographic parameters of acromial morphology (AI, CSA, LAA and acromion type) between the trauma and the degenerative groups. This showed that only the LAA and acromion type were associated with degenerative rotator cuff pathology. The degenerative group had a significantly lower LAA (71.83° vs. 75.02°, p = 0.001) and a higher proportion of type III acromions (8 of 83 vs. 1 of 76, p = 0.035) than the trauma group. There were no significant differences in the AI (0.75 vs. 0.74, p = 0.211) or CSA (37.72° vs. 36.94°, p = 0.17) between the two groups (Table 2).
ROC curves for the three parameters (ATI on MRI and X-ray and LAA) were assessed. Nonsignificant parameters (CSA and CI) and acromion type were excluded. The ROC curve analyses demonstrated that the ATI on MRI with a cut-off value of 0.965 discriminated between the presence and the absence of SAIS (area under the curve (AUC), 0.739; sensitivity, 0.771; and specificity, 0.566), and the ATI on X-ray with a cut-off value of 0.865 discriminated between the presence and the absence of SAIS (AUC, 0.756; sensitivity, 0.687; and specificity, 0.697; Figure 4). The cut-off value of the LAA was 68.65° with an AUC of 0.630. An AUC between 0.9 and 1 is considered excellent, 0.8–0.9 is good, 0.7–0.8 is fair, 0.6–0.7 is poor and 0.5–0.6 is failed. The ATI on X-ray and MRI showed fair accuracy and was more accurate and reliable than other parameters for predicting degenerative rotator cuff pathology.
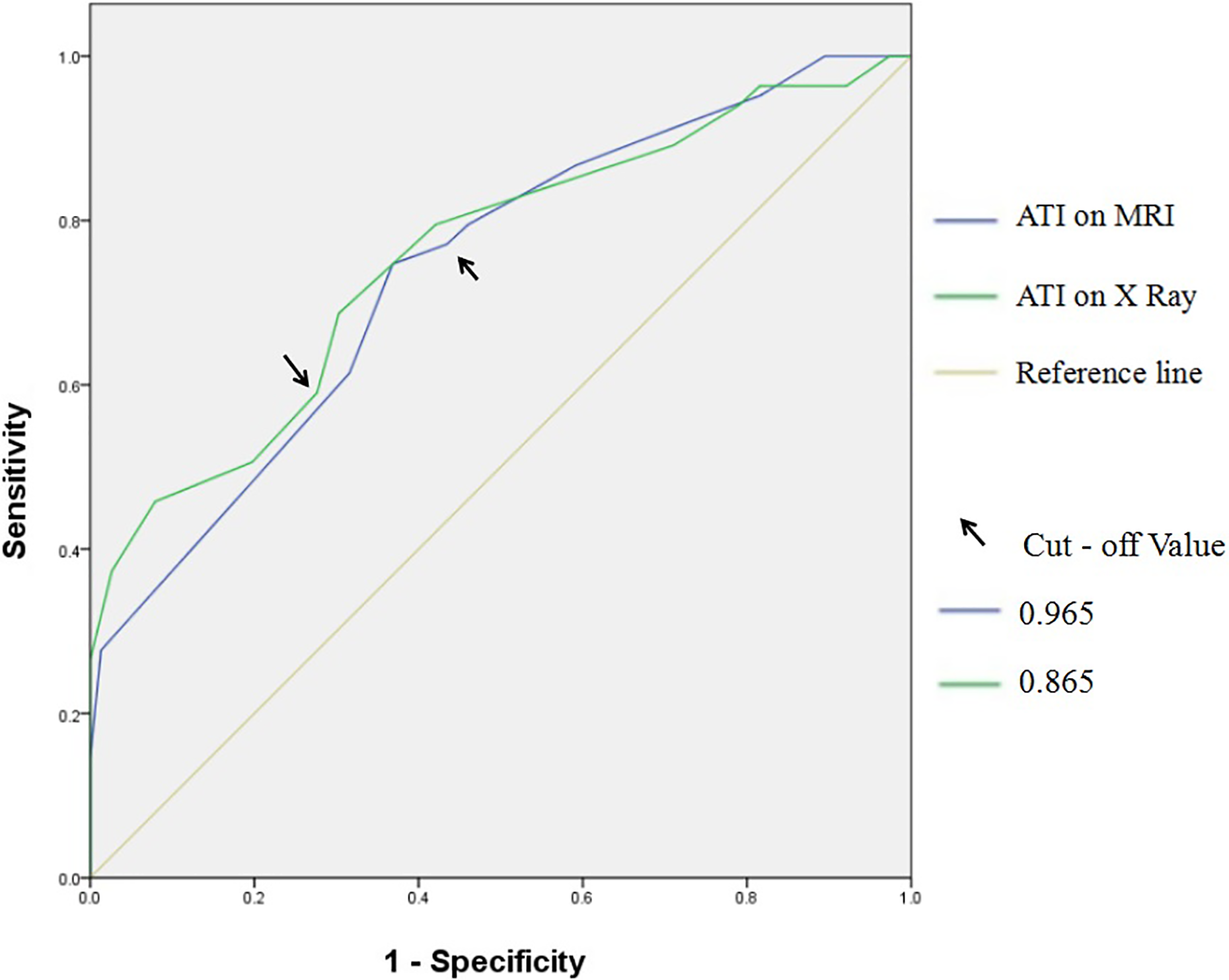
ROC curves for the prediction of degenerative RCT with ATI of MRI and ATI of X-ray. The cut-off value of the ATI on MRI and ATI on X-ray is 0.965 and 0.865, respectively. ROC: receiver operating characteristic; RCT: rotator cuff tear; ATI: acromion–greater tuberosity impingement index; MRI: magnetic resonance imaging.
The relationships among the radiographic acromial morphology parameters were evaluated (Table 3). The ATIs on X-ray and MRI were closely related (0.700, p = 0.001). The ATI on X-ray was negatively related to the LAA (−0.396, p = 0.001) and positively related to the AI (0.264, p = 0.001), the CSA (0.165, p = 0.038) and acromion type (0.303, p = 0.001). The ATI on MRI was also negatively related to the LAA (−0.207, p = 0.009) and positively related to the AI (0.192, p = 0.015) and acromion type (0.301, p = 0.001). The AI, a parameter of coronal morphology, was positively related to the CSA (0.260, p = 0.001) and negatively related to the LAA (−0.311, p = 0.001). Acromion type, a parameter of acromial sagittal morphology, was not related to coronal morphology (i.e. AI, CSA or LAA; each p > 0.05).
The correction between ATI and other parameters.a
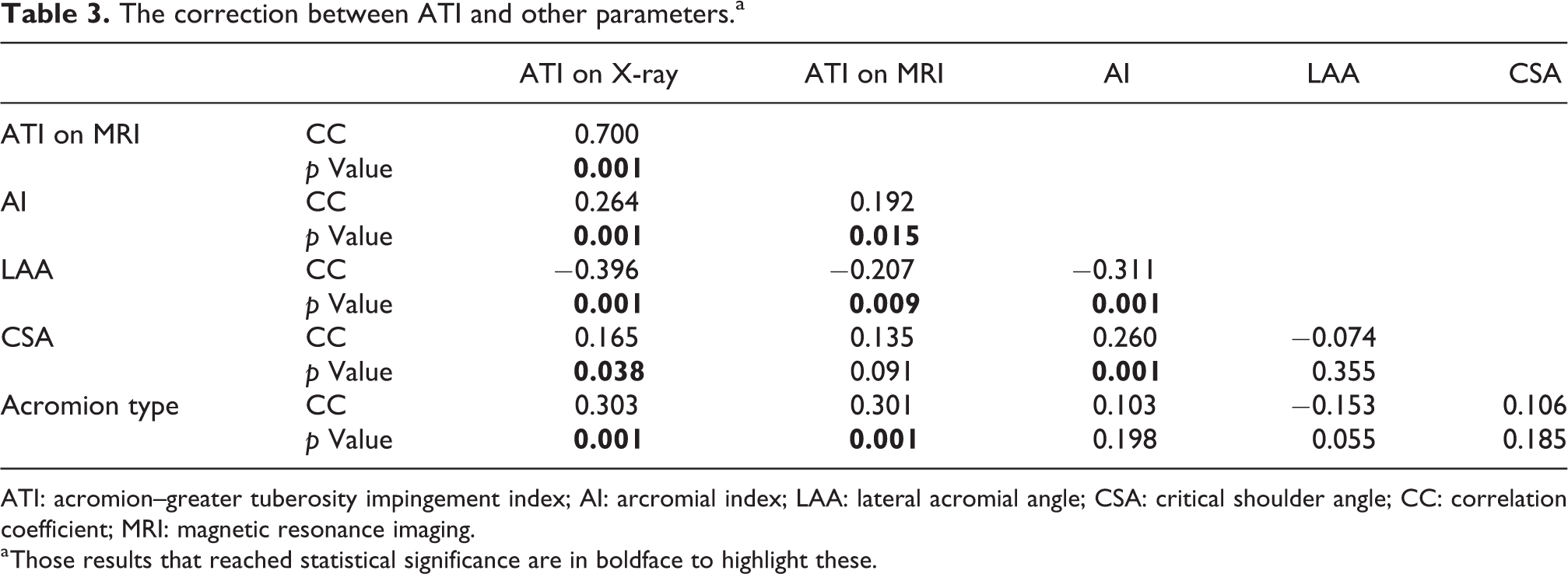
ATI: acromion–greater tuberosity impingement index; AI: arcromial index; LAA: lateral acromial angle; CSA: critical shoulder angle; CC: correlation coefficient; MRI: magnetic resonance imaging.
a Those results that reached statistical significance are in boldface to highlight these.
The ATI on X-ray and MRI accurately reflected postoperative changes in the lateral acromion. The ATI on MRI was more accurate and guided the choice of operation (i.e. acromioplasty or acromion decompression) according to the value of the ATI. More patients in the degenerative group needed acromioplasty than in the trauma group (36.1% vs. 15.8%, p = 0.002). More patients in the degenerative group needed acromion decompression (47.0% vs. 38.2%, p = 0.032; Table 4). The ATI on MRI was significant lower after surgery compared to before surgery in both the degenerative (0.96 vs. 0.99, p = 0.001) and the trauma (0.94 vs. 0.96, p = 0.015; Table 5 and Figure 5) groups. The ATI on X-ray after surgery was significantly lower in the degenerative group (0.86 vs. 0.89, p = 0.002), whereas there was no significant difference in the trauma group (0.85 vs. 0.84, p = 0.069; Table 5).
Comparison of acromion surgery type between the two groups.a

a Those results that reached statistical significance are in boldface to highlight these.
Comparison of ATIs between preoperation and postoperation in each group.a

ATI: acromion–greater tuberosity impingement index; MRI: magnetic resonance imaging.
a Those results that reached statistical significance are in bold to highlight these.

(a) Patient with traumatic RCT shows ATI of 0.95, (b) patient with subacromial impingement syndrome shows higher ATI of 1.05, patient with subacromial impingement syndrome shows ATI of 1.02 before acromion surgery (c) and lower ATI of 0.95 after acromioplasty (d). RCT: rotator cuff tear; ATI: acromion–greater tuberosity impingement index.
Discussion
This study proposes a new measurement, the ATI, for describing the potential dynamic correlation between the acromion and the greater tuberosity of the humerus, which is an accurate predictor of SAIS or degenerative RCTs. Patients with these lesions have a higher ATI than patients with traumatic injuries on both X-ray and MRI. As a potential dynamic parameter, the ATI is related to other coronal parameters and to a sagittal parameter. The ATI, the LAA and acromion type are associated with SAIS and degenerative RCTs, whereas the CSA and AI are not. The ATI on MRI is an accurate parameter for guiding acromion surgery and can reflect postoperative changes in acromial morphology.
Our findings show that the ATI on AP glenohumeral X-ray is related to both other coronal parameters and sagittal parameters. This is important for assessing degenerative rotator cuff pathology in the absence of outlet view radiographs. However, X-rays are more prone to error than MRI when it comes to assessing the acromion undersurface in patients with different shaped acromions. Moreover, measurements are affected when AP glenohumeral X-rays are taken in internal or external rotation. 14 MRI is accurate and is not affected by rotation. An acromiohumeral distance <7 mm has been used to predict degenerative rotator cuff pathology, 15 but this parameter differs markedly with the position of the arm and individual differences. 16 By contrast, the ATI on MRI is reliable and independent of individual differences and the shoulder adduction angle, because it is not an absolute value and the motion of the glenohumeral joint involves dynamic concentric circles in the coronal plane. 17
Static parameters such as the LAA, AI and CSA can predict degenerative RCTs. 3 –8 However, these parameters do not change with age or following acromioplasty. 11 Our new parameter directly reflects the severity of subacromial impingement and changes in the subacromial space after acromioplasty, which is usually performed in patients with SAIS after conservative treatment fails. During acromioplasty, the anterior and lateral borders of the acromion should be resected by about 5 mm. 1 However, there are no criteria for quantitative acromioplasty according to the preoperative imaging examination. To the best of our knowledge, the ATI on MRI is the first parameter that might directly and precisely guide acromion surgery. Using the preoperative ATI on MRI, the range of acromioplasty can be planned precisely and implemented (to reduce the ATI to below a cut-off value), which might reduce the incidence of recurrent RCT and subacromial impingement. The severity of SAIS can also be graded according to the ATI, although further studies are needed to evaluate the factors influencing the ATI criterion for guiding acromion surgery.
The relationship between acromial morphology and the pathogenesis of RCTs is controversial. Neer stated that up to 95% of RCTs result from chronic impingement at the undersurface of the acromion. 18 Many studies have examined the association between RCTs and different characteristics of the acromion. A greater incidence of RCTs has been reported with type III acromions compared to types II or I. 2 In another student, patients with a higher AI had a higher incidence of RCTs and recurrent tears after repair. 4 A low LAA angle is associated with rotator cuff disease. 3 A recent study showed that a CSA > 38° significantly increased the risk for re-tearing after rotator cuff repair. 19 In the current study, the LAA and acromial type parameters were also closely related to the pathogenesis of degenerative RCTs.
However, some studies have suggested that acromial morphology is unreliable. In one study, no positive correlation was reported between a higher AI and the rate of recurrent RCTs. 10 The CSA does not reflect the risk in tear progression, with no change in the CSA at an average follow-up of 6 years in another study. 11 Previous analyses showed that patients with degenerative RCTs had CSA values similar to controls. 20 One study comparing people of different ethnicities suggested that the AI can predict rotator cuff disease in Brazilians but not in Japanese. 21 In our study, the CSA and AI were not related to degenerative RCTs, perhaps because East Asians have longer acromions than North Americans. 22
This study has several limitations. First, measuring the ATI on X-ray might have biased the results because it depends on the quality of the radiographs, although nonstandardized radiographs were excluded. Second, measuring the parameter on MRI in the coronal plane, which is not necessarily parallel to the long axis of the humerus, might have caused errors. Third, the number of patients in each group was small. Finally, selection bias may have arisen because we included only symptomatic patients, which potentially decreased the accuracy of the control group, which might have included asymptotic individuals with shoulder pathology.
Conclusion
The ATI is a good parameter for predicting degenerative supraspinatus tendon tears or SAIS on both X-ray and MRI. The ATI on MRI was more accurate and can precisely guide acromion surgery.
Footnotes
Acknowledgements
We thank all authors of the included studies and the authors listed have made substantial contributions to the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was a retrospective study and was approved by the ethics committee at the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Suzhou Livelihood Science and Technology Project SS201814.